Practice Essentials
Most urethral injuries are associated with well-defined events, including major blunt trauma such as caused by motor vehicle collisions or falls. Penetrating injuries in the area of the urethra may also cause urethral trauma. Straddle injuries may cause both short- and long-term problems. Iatrogenic injury to the urethra from traumatic catheter placement, transurethral procedures, or dilation is not uncommon.
Urethral injuries can be classified into 2 broad categories based on the anatomical site of the trauma. Posterior urethral injuries are located in the membranous and prostatic urethra. These injuries are most commonly related to major blunt trauma such as motor vehicle collisions and major falls, and most of such cases are accompanied by pelvic fractures. Injuries to the anterior urethra are located distal to the membranous urethra. Most anterior urethral injuries are caused by blunt trauma to the perineum (straddle injuries), and many have delayed manifestation, appearing years later as a urethral stricture.
External penetrating trauma to the urethra is rare, but iatrogenic injuries are quite common in both segments of the urethra. Most are related to difficult urethral catheterizations.
The diagnosis of urethral trauma is made with retrograde urethrography, which must be performed prior to insertion of a urethral catheter to avoid further injury to the urethra. Extravasation of contrast demonstrates the location of the tear. Further management is predicated on the findings of urethrography in combination with the patient's overall condition. See the images below.


Trauma to the male urethra must be efficiently diagnosed and effectively treated to prevent serious long-term sequelae. Patients with urethral stricture disease secondary to poorly managed traumatic events are likely to have significant voiding problems and recurring need for further interventions. Many of these men have significant orthopedic and neurologic injuries, as well. Rehabilitation requires reconstruction of the urinary tract in a manner that does not interfere with the healing process.
Relevant Anatomy
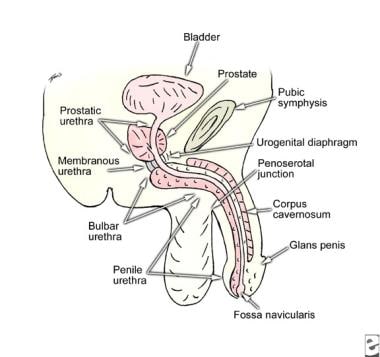
The male urethra may be divided into 2 portions. The posterior urethra includes the prostatic urethra, which extends from the bladder neck through the prostate gland. It then joins the membranous urethra, which lies between the prostatic apex and the perineal membrane. The anterior urethra begins at that point and includes 3 segments. The bulbar urethra courses through the proximal corpus spongiosum muscles to reach the penile urethra. The penile urethra then extends through the pendulous portion of the penis to the final segment, the fossa navicularis. The fossa navicularis is invested by the spongy tissue of the glans penis. See image below.
Potential areas for injury can be deduced from further study of the urethral anatomy. The membranous urethra is prone to injury from pelvic fracture because the puboprostatic ligaments fix the apex of the prostate gland to the bony pelvis and thus cause shearing of the urethra when the pelvis is displaced. The bulbar urethra is susceptible to blunt force injuries because of its path along the perineum. Straddle-type injuries from falls or kicks to the perineal area can result in bulbar trauma. Conversely, the penile urethra is less likely to be injured from external violence because of its mobility, but iatrogenic injury from catheterization or manipulation can occur, which is also possible in the fossa navicularis.
Pathophysiology
Injury to the posterior urethra occurs when a shearing force is applied at the prostatomembranous junction in blunt pelvic trauma. The prostatic urethra is fixed in position because of the attachments of the puboprostatic ligaments. Displacement of the bony pelvis from a fracture type injury thus leads to either tearing or stretching of the membranous urethra. [1]
Anterior urethral injury most often results from a blunt force blow to the perineum, producing a crushing effect on the tissues of the urethra. The initial injuries are often ignored by the patient, and urethral injury manifests years later as a stricture. The stricture results from scarring induced by ischemia at the site of the injury. Penetrating injuries also occur in the anterior urethra as a result of external violence.
Etiology
As with many traumatic events, the etiology of a urethral injury can be classified as blunt or penetrating. In the posterior urethra, blunt injuries are almost always related to massive deceleration events such as falls from some distance or vehicular collisions. These patients most often have a pelvic fracture involving the anterior pelvis. [2] In a study of 12,374 motorcycle accident victims (11,926 riders, 94.5% of them male, and 448 pillion passengers, 52.9% of them male), urethral injury occurred in 81% of patients with pelvic fractures. [3]
Blunt injury to the anterior urethra most often results from a blow to the bulbar segment such as occurs when straddling an object or from direct strikes or kicks to the perineum. [4] Blunt anterior urethral trauma is sometimes observed in the penile urethra in the setting of penile fracture.
Penetrating trauma most often occurs to the penile urethra. Etiologies include animal bites [5] and gunshot and stab wounds. Insertion of foreign bodies is another rare cause of anterior injury. It is usually a result of autoerotic stimulation or may be associated with psychiatric disorders. [6]
Iatrogenic injuries to the urethra occur when difficult urethral catheterization leads to mucosal injury with subsequent scarring and stricture formation. Catheter placement is the most common cause of iatrogenic urethral trauma. Iatrogenic urethral injuries also occur after radical prostatectomy, pelvic radiotherapy, and other abdominopelvic surgery. [7]
Epidemiology
Posterior urethral injuries are most commonly associated with pelvic fracture, with an incidence of 5%-10%. With an annual rate of 20 pelvic fractures per 100,000 population, these injuries are not uncommon. [8] Anterior urethral injuries are less commonly diagnosed emergently; thus, the actual incidence is difficult to determine. However, many men with bulbar urethral strictures recall an antecedent perineal blunt injury or straddle injury, making the true frequency of anterior urethral injury much higher. Penetrating injury to the urethra is rare, with major trauma centers reporting only a few per year.
Prognosis
Men with urethral injuries have an excellent prognosis when managed correctly. Problems arise if a urethral injury is unrecognized and the urethra is further damaged by attempts at blind catheterization. In those instances, future reconstruction may be compromised and recurrent stricture rates rise. When managed well, these men have an excellent chance of becoming totally rehabilitated from a urinary standpoint.
Continence rates approach 100% in all series, particularly if the bladder neck is not involved. Potency status is probably related to the extent of the injury itself rather than the management of the problem. Several series have demonstrated only a small group of men losing erectile capabilities following the urethroplasty when they were potent following the initial injury. [9]
The main complication following reconstruction of posterior injuries is recurrent stricture. When managed with standard urethroplasty techniques, recurrent stricture requiring major repeat operation should be observed in only 1%-2% of patients, although 10%-15% may require either dilation or incision of a short recurrence. [10]
Endoscopic realignment by experienced physicians appears to produce similar results. When performed at 5-7 days postinjury, rare infectious complications occur despite the presence of the organized pelvic hematoma.
Complications of reconstruction of anterior urethral injuries are similar to those observed in posterior urethral repairs.
-
Urethrogram demonstrating partial urethral disruption.
-
Urethrogram demonstrating complete urethral disruption.
-
Male urethral anatomy
