Background
Ocular burns consist of burns to the sclera, conjunctiva, cornea, and eyelids. Chemical burns, particularly those involving the cornea, are considered a true ophthalmologic emergency and require prompt assessment and intervention to minimize morbidity. [1] Ocular burn injuries are classified by etiologic agents as either chemical injuries (eg, those caused by acid or alkali) or radiant energy injuries (eg, those caused by heat, electricity or ultraviolet [UV] radiation).

Many ocular burns can be adequately managed in the emergency department (ED). Transfer may be required for specialized ophthalmologic care; however, the emergency physician must evaluate the patient’s stability for transfer. In some situations, life-threatening conditions (eg, airway burns) must be addressed (securing of the airway) prior to transfer. For patients with thermal burns, transfer to a burn center is indicated in the presence of significant facial involvement or inhalation injury.
Pathophysiology
The severity of an ocular burn is directly correlated with the duration of exposure and the causative agent. In particular, chemical burn severity relates to the solution pH, contact duration, solution quantity, and solution penetrability.
Burns damage tissues primarily by denaturing and coagulating cellular proteins and secondarily by causing vascular ischemic damage. For both thermal and chemical burns, severity is determined by the depth and degree of epithelial damage and limbal ischemia. If the limbus is affected significantly, the cornea may develop recurrent epithelial defects, and conjunctival invasion onto the cornea may occur as a result of the loss of stem cells responsible for renewing corneal epithelium. Laser injuries from radiant energy cause injury to the retina through the transfer of light energy into heat, leading to tissue necrosis. [2]
A rare type of ocular injury comes from electrical burns. [3]
Radiant energy burns
Injury from radiant energy usually results from contact with hot liquids, hot gases, fireworks or molten metals. Cell death from thermal burns is limited to the superficial epithelium; however, thermal necrosis and penetration can occur.
With UV burns, epithelial injury results in punctate keratitis. Although the pain is often delayed, UV corneal burns are exquisitely painful. Lasers also can lead to direct retinal injury and, rarely, corneal injury. [2]
Chemical burns
Alkali substances are lipophilic and penetrate more rapidly than acids. Saponification of cell membrane fatty acids causes cell disruption and death. In addition, the hydroxyl ion hydrolyzes intracellular glycosaminoglycans and denatures collagen. The damaged tissues stimulate an inflammatory response, which damages the tissue further by the release of proteolytic enzymes. This is termed liquefactive necrosis.
Alkali substances can pass into the anterior chamber rapidly due to the inability to buffer alkali (within approximately 5-15 min), exposing the iris, ciliary body, lens, and trabecular network to further damage. Irreversible damage occurs at a pH value above 11.5.
Acid burns cause protein coagulation in the corneal epithelium, which limits further penetration. As a rule, these burns are nonprogressive and superficial. Hydrofluoric acid, however, is an exception to this rule: it is a weak acid that rapidly crosses the cell membrane as it remains nonionized. In this way, hydrofluoric acid acts as an alkali, causing liquefactive necrosis.
In addition, fluoride ions are released into the cells. Fluoride ions may inhibit glycolytic enzymes and may combine with calcium and magnesium to form insoluble complexes. The extreme local pain is believed to result from calcium immobilization, which leads to nerve stimulation by shifting potassium ions. Acute fluorosis can occur as the fluoride ions enter the systemic circulation, resulting in cardiac, respiratory, gastrointestinal, and neurologic symptoms. Severe hypocalcemia, which is resistant to large doses of calcium, can occur.
Etiology
Radiant energy
Thermal injuries can be caused by hot substances (eg, curling irons, hot curlers, cigarettes, and hot liquids). Hot liquids have been known to splash into the eye from substances that explode after removal from a microwave; steam from hot liquids is also a potential cause. Fire is a common cause of burns to the face and eyes.
UV keratitis may be caused by bright sunlight, particularly when the light is reflected from snow or cement. Skiers at high altitudes are particularly susceptible to this injury. Welders who view the arc without protective goggles are at risk for injury. Lasers used in industry, military, and medical practice also can cause ocular burns. [2]
Chemical agents
Multiple chemicals used in the home and work environment can lead to injury. Common acids causing ocular burns include sulfuric acid, sulfurous acid, hydrochloric acid, nitric acid, acetic acid, chromic acid, and hydrofluoric acid. Automobile battery explosion, which causes a sulfuric acid burn, is perhaps the most common acidic burn of the eye.
Hydrofluoric acid may be found at home in rust removers, aluminum brighteners, and heavy-duty cleaners. Certain industries use hydrofluoric acid in brick cleaning, glass etching, electropolishing, and leather tanning. Hydrofluoric acid also is used to control fermentation in breweries. Ocular hydrofluoric toxicity can occur from liquid or gaseous exposure.
Common alkali substances contain ammonium hydroxide, potassium hydroxide, sodium hydroxide, calcium hydroxide, and magnesium hydroxide. Substances that contain such compounds and can be found in a home include lye, cement, lime, and ammonia. Laundry detergent pods are becoming a new source of exposure in the pediatric population. [4] Air bags aerosolize sodium hydroxide on inflation and may cause alkali keratitis. [5] Additionally, sparklers and flares contain magnesium hydroxide and phosphorus.
Certain chemical agents, such as mustard gas, can result in chronic and delayed-onset keratitis. [6]
Epidemiology
United States statistics
Ocular burns represent 7-18% of the eye injuries seen in EDs. [7] Eye injuries account for 3-4% of all occupational injuries. [8] The vast majority (84%) are chemical burns. Thermal burns account for 16% of ocular burn cases. Approximately 15-20% of patients with facial burns exhibit ocular injury. The ratio of the relative frequencies of acids and alkalis as the causative agents of chemical injury ranges from 1:1 to 1:4, according to several studies.
International statistics
A report from a developing country found that up to 80% of ocular chemical burns were due to industrial or occupational exposure. A report from Norway indicated that fish bile was the cause of 14% of the ocular chemical burns reported in northern Norway. [9] Acid attacks on women that often include the eyes and lead to serious morbidity have been a serious problem in the developing world. [10]
Age- and sex-related demographics
Any age group may be at risk for ocular burns. One study indicated that the average age of patients with ocular burns was 36 years. There is a strong association of ocular burns with younger age groups within the occupational setting.
Ocular burns are more common in males than in females. This difference probably reflects the male predominance in the industrial occupations at highest risk for ocular injuries, such as construction and mining.
Prognosis
See the image below.
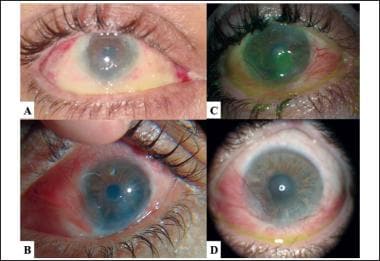 Photographs of right eye after airbag-related alkali burn at 1 week (a), 2 months (b), 4 months (c), and 6 months (d) after the initial motor vehicle accident with airbag deployment. Note severe limbal ischemia at 1 week (a) leading to severe conjunctivalization of the cornea at later time points. Courtesy of Shawn S Barnes, MSIV, University of Hawaii, John A Burns School of Medicine.
Photographs of right eye after airbag-related alkali burn at 1 week (a), 2 months (b), 4 months (c), and 6 months (d) after the initial motor vehicle accident with airbag deployment. Note severe limbal ischemia at 1 week (a) leading to severe conjunctivalization of the cornea at later time points. Courtesy of Shawn S Barnes, MSIV, University of Hawaii, John A Burns School of Medicine.
Prognosis depends on both prompt recognition and emergent irrigation. This is especially important in those with concurrent polytrauma in whom other injuries are often prioritized, but careful attention should be given to ocular burns that are time sensitive. [11]
The prognosis depends on the depth of the injury. Corneal burns are classified into 4 grades by the Roper Hall scale, as follows:
-
Grade 1 - Only corneal epithelial loss is present, and no conjunctival ischemia is found; the prognosis is very good
-
Grade 2 - Some corneal edema and haze are present, and the conjunctival ischemia affects less than one third of the limbus; some permanent scarring may occur
-
Grade 3 - The cornea has significant haziness, and limbal ischemia is less than one half of the limbus; the prognosis is variable, and vision usually is impaired
-
Grade 4 - The cornea is opaque, and limbal ischemia is greater than one half of the limbus, with a possibility of globe perforation; the prognosis is poor
A newer scale by Dua et al subdivides the grade 4 of Roper Hall since they may be treated by autolimbal transplantation or amniotic sheets by corneal specialists and fare better than in the past. [12] The grading scheme then splits the limbus into 12 clock hours as follows:
-
Grade 1 - 0 clock hours of limbal involvement; 0% conjunctival involvement; prognosis is very good
-
Grade 2 - ≤3 clock hours of limbal involvement; ≤30% conjunctival involvement; prognosis is good
-
Grade 3 - >3-6 clock hours of limbal involvement; >30-50% conjunctival involvement; prognosis is good
-
Grade 4 - >6-9 clock hours of limbal involvement; >50-75% conjunctival involvement; prognosis is good to guarded
-
Grade 5 - >9 to < 12 clock hours of limbal involvement; >75% to < 100% conjunctival involvement; prognosis is guarded to poor
-
Grade 6 - Total limbal involvement; total conjunctival 100% involvement; prognosis is very poor
Gupta et al showed a clinically significant difference between outcomes in the Roper Hall and Dua classification, with the subdivision of the grade 4 Roper Hall being split into 3 categories and leading to differences in visual acuity when managed with amniotic membrane transplantation. [13, 14] Both systems may present a challenge to those with less experience in grading limb ischemia than corneal specialists. [15]
The major concerns with ocular burns are final visual acuity (ie, degree of visual impairment) and cosmetic appearance (eg, extent of scarring).
Radiant energy burns
Thermal burns can cause significant corneal and ocular adnexal injuries. Stern et al, reviewing 127 patients who sustained ocular injury secondary to thermal burns, found that eyelid burns were the most common complication, occurring in 52 patients. [16] Of those 52 burn victims, approximately 60% developed eyelid contractures.
Early surgical consultation and aggressive intervention have been recommended to protect the globe. Other thermal ocular injuries include corneal burns or abrasions, conjunctivitis, cataracts, and corneal perforation. Fortunately, the need for enucleation is rare; only 2 of the 127 burn victims in the study by Stern et al lost the injured eye. [16] With prompt treatment and early ophthalmologic intervention, thermal burns generally have good visual outcomes. Laser injuries typically affect the retina, with corneal sparing, although there are cases of corneal damage. They often heal over time without intervention, but they require specialized referral. [2]
Chemical burns
The following images show chemical burns to the eyes.


Chemical burns are often bilateral and frequently result in devastating vision loss. Ocular complications of severe burns include glaucoma, corneal perforation, cataracts, scarring of the cornea, conjunctival cul-de-sac, conjunctiva and eyelid complications, retinal detachment, and corneal ulcerations.
As much as 1-2 years of corrective surgery may be needed to correct damage from more severe burns. A study by Kuckelkorn et al reported that one third of 131 patients with ocular burns were considered disabled; approximately 15% were considered blind. [17] In 1995, almost one third of corneal transplants were for eyes that sustained a chemical injury. Unfortunately, the success rate for transplants for this condition is less than 50%. Some patients require 4-5 transplants before success is achieved.
Patient Education
Primary prevention and patient counseling on proper eye protection is essential because more than 90% of injuries can be avoided with the use of eye protection. [18] Additionally emphasis on proper treatment with immediate irrigation should be emphasized on product labels and in settings where exposures may occur.
Welders must be informed of the importance of keeping on safety goggles while working. People who spend significant amounts of time outdoors must be made aware of the danger of UV keratitis, particularly at high altitudes. In addition, workers in laboratories and other industrial fields are at risk. In the United States, the Occupational Safety and Health Administration (OSHA) mandates that eye-wash stations are readily available in work environments with injurious corrosive materials. [19]
An estimated 90% of chemical eye injuries are avoidable. It is essential to emphasize the importance of wearing safety glasses when working with hazardous materials or in hazardous situations. Children sustain chemical burns most often when they are unsupervised. It is therefore critical to keep all hazardous home products in an area that is difficult for a child to access.
For patient education resources, see the Burns Center, as well as Eye Injuries, Chemical Eye Burns, Thermal (Heat or Fire) Burns, and How to Instill Your Eyedrops.
-
Severe chemical injury with early corneal neovascularization.
-
Photographs of right eye after airbag-related alkali burn at 1 week (a), 2 months (b), 4 months (c), and 6 months (d) after the initial motor vehicle accident with airbag deployment. Note severe limbal ischemia at 1 week (a) leading to severe conjunctivalization of the cornea at later time points. Courtesy of Shawn S Barnes, MSIV, University of Hawaii, John A Burns School of Medicine.
-
Stromal haze with opacification of the cornea.
-
Complete cicatrization of the corneal surface.




