Overview
The lips are two fleshy folds that surround the oral orifice. The perioral region is bounded superiorly by the nasolabial folds, laterally by the oral commissures, and inferiorlyby the mentolabial sulcus. [1] The lips are composed of multiple layers: skin, subcutaneous tissue, muscle, glandular tissue, and mucosa. [1] They function to provide competence to the oral cavity during mastication and at rest. The lips affect uttered sounds that facilitate spoken language and provide changes in facial expression that facilitate unspoken language. They provide sensory information about food prior to its placement in the oral cavity. To accomplish this multitude of functions, lips require a complex system of muscles and supporting structures. [2, 3, 4]
Superficial anatomy
The upper lip extends from the base of the nose superiorly to the nasolabial folds laterally and to the free edge of the vermilion border inferiorly. The lower lip extends from the superior free vermilion edge superiorly, to the commissures laterally, and to the mandible inferiorly. Around the circumferential vermilion-skin border, a fine line of pale skin accentuates the color difference between the vermilion and normal skin. Along the upper vermilion skin border, two paramedian elevations of the vermilion form the Cupid bow. Two raised vertical columns of tissue form a midline depression called the philtrum. The philtrum is located between the paramedian elevations of the vermilion and the columella above. The philtrum and paramedian elevations provide structural and aesthetic prominence to the upper lip. [1] The labiomental crease passes horizontally in an inverted U-shape across the lower lip, which intraorally corresponds to the depth of the gingivolabial sulcus.
Histology
From superficial to deep, the layers of the upper and lower lips include the epidermis, subcutaneous tissue, orbicularis oris muscle fibers, and mucosa. Thick bundles of skeletal muscle fibers (orbicularis oris, incisivus superior and inferior, and the direct labial tractors) along with their attachments to the skin, mucosa, or other muscle fibers pass through the center of each lip. [1] In a cross-section, the superior and inferior labial arteries can be observed as they course between the orbicularis muscle fibers and the mucosa. The vermilion is composed of nonkeratinized squamous epithelium that covers numerous capillaries, which give the vermilion its characteristic color. The dermis of the vermilion border is thinner (approximately 0.5 mm) than that of the other regions due to its proximity to the underlying musculature. [5] Numerous minor salivary glands can be observed on a histologic section of the lip. Hair follicles and sebaceous glands are located throughout the lip skin; however, these structures are absent in the vermilion border. [6] Glycogen content increases progressively from the skin to the mucosa, reflecting functional adaptations for hydration and barrier maintenance. [5]
Epidermis
The epidermis of the lips is the outermost layer, consisting of stratified squamous epithelium. Unlike the skin of other body parts, the lip epidermis is thinner, which contributes to its sensitivity and susceptibility to environmental factors. The epidermis of the vermilion border is particularly unique as it transitions from keratinized to nonkeratinized squamous epithelium, which is crucial for maintaining moisture and color. [5, 7]
Subcutaneous tissue
Beneath the epidermis lies the subcutaneous tissue, which includes connective tissue that provides structural support and elasticity. This layer is relatively sparse in the adipose tissue compared with other body areas, contributing to the lips' flexibility and mobility. The submucosa contains minor salivary glands and neurovascular structures. The minor salivary glands are predominantly mucous-secreting and are distributed throughout the inner aspect of the lips, aiding in lubrication. [1, 5, 7]
Orbicularis oris muscle
The orbicularis oris muscle forms a continuous band of striated muscle fibers that encircle the oral cavity. Histologically, this muscle is composed of striated muscle fibers that are interspersed with connective tissue, allowing for complex and coordinated movements. It plays a critical role in lip movement, enabling functions such as speech, mastication, and facial expressions. The superior and inferior labial arteries course between this muscle layer and the mucosa, providing an extensive vascular supply to the lips. [1, 5, 7]
Mucosa
The internal surface of the lips is lined by nonkeratinized squamous epithelium with an underlying lamina propria. This epithelium is thicker than that of the vermilion border, measuring approximately 218 μm on average. The lamina propria contains dense connective tissue with a rich capillary network. The mucosal layer also houses numerous minor salivary glands that contribute to oral moisture. [5, 7]
Blood Supply
Blood supply to both lips stems from the external carotid system. [8] The facial artery ascends from the neck over the midbody of the mandible just anterior to the insertion of the masseter muscle. The facial artery branches into the submental artery that passes under the mandibular body in an anteromedial direction. The facial artery ascends in a plane deep to the platysma, risorius, and zygomaticus major and minor muscles and superficial to the buccinator and levator anguli oris. This artery branches into an inferior and a superior labial artery, which course beneath the orbicularis oris and anastomose with the contralateral vessel. [9]
The superior labial artery usually branches from the facial artery 1.1 cm lateral (SD 0.43) and 0.9 cm (SD 0.20) superior to the oral commissure. The external diameter of the artery at its origin averages around 1.6 mm (range: 0.6-2.8 mm). The superior labial artery supplies the upper lip, nasal septum, and ala of the nose. It also contributes columellar branches. The SLA forms connections with contralateral vessels and branches of the internal carotid system (e.g., dorsal nasal artery). [1, 9]
The inferior labial artery branches from the facial artery 2.6 cm (SD 0.70) lateral and 1.5 cm (SD 0.45) inferior to the oral commissure. Its external diameter ranges from 0.5 mm to 1.5 mm at its origin. The inferior labial artery supplies the lower lip by running beneath the depressor anguli oris (triangularis) muscle and piercing the orbicularis oris. It anastomoses with its contralateral counterpart and other arteries such as the mental branch of the inferior alveolar artery. [1, 9]
The facial artery then ascends in the nasolabial groove as the angular artery, forming branches with the nasal ala and anastomosing with the dorsal nasal artery. The facial and labial arteries communicate with the subdermal plexus through a dense population of musculocutaneous perforators.
In contrast, the submental artery usually has only one main perforator, which penetrates the platysma and ramifies to supply 3-4 areas of the subdermal plexus.
Lymphatic Drainage
Lymphatic drainage from the upper lip is unilateral except for the midline. The lymphatics coalesce to form five primary trunks that mainly lead to the ipsilateral submandibular nodes, with some drainage also going to the periparotid lymph nodes (see the image below).
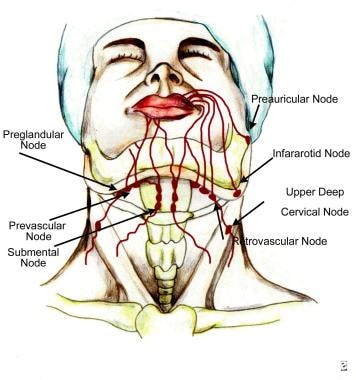
Occasionally, some drainage may be available to the ipsilateral submental lymph nodes. The lower lip lymphatics also coalesce to form five primary trunks that lead to the bilateral submental nodes from the central lip and the unilateral submandibular lymph nodes from the lateral lip.
The submental, submandibular, and parotid lymph nodes are the first echelon nodes for the lips. Submental nodes secondarily drain into the ipsilateral submandibular nodes, and both submandibular and parotid nodes secondarily drain into the ipsilateral jugulodigastric lymph nodes.
Motor Innervation
Motor innervation to the perioral musculature uniformly is from the seventh cranial nerve. The facial nerve has temporal, zygomatic, buccal, marginal mandibular, and cervical branches. The buccal and marginal branches primarily supply innervation to the perioral musculature. Interconnection between the branches is common, with at least four connections formed after exiting the parotid gland. The fibers supply a majority of the muscles of the face from their undersurface. The exceptions are the three deepest perioral muscles, i.e., the buccinator, levator anguli oris, and mentalis.
Skandalakis described partial innervation of the depressor muscles by an anterior ramus of the cervical branch in addition to the primary marginal branch innervation. [10] Dingman and Grabb reported that in 100 dissections, the mandibular branches were superior to the mandibular border and anterior to the facial artery. [11] In contrast, Nelson and Gingrass found that multiple branches ascending from below the mandibular border provided frequent innervation to the lip depressors. [12] Nelson believed that any branch supplying the lip depressors should be classified as a mandibular branch, as opposed to Skandalakis’ classification.
Studies have identified additional axonal subtypes within the facial nerve branches that may contribute to motor control. These include sympathetic axons hypothesized to regulate involuntary muscle tone and proprioceptive fibers providing feedback for fine-tuned movements of facial expressions. [13]
Sensory Innervation
Sensory innervation to the perioral region is from the maxillary and mandibular branches of the fifth cranial nerve. The infraorbital nerve, which is a terminal branch of the maxillary nerve, innervates the upper lip. This nerve exits the infraorbital foramen 4-7 mm below the inferior orbital rim on a vertical line that descends from the medial limbus of the iris. The nerve runs beneath the levator labii superioris and superficial to the levator anguli oris to supply the lateral nasal sidewall, ala, columella, medial cheek, and upper lip.
The lower lip and chin receive sensory innervation from the branches of the mandibular nerve. The inferior alveolar nerve, a branch of the mandibular nerve, forms the nerve to the mylohyoid just proximal to entering the lingula of the mandible. The terminal branches of this nerve inconsistently supply the chin and the region immediately lateral to it. The inferior alveolar nerve travels through the body of the mandible to exit from the mental foramen. The mental foramen is located below the apex of the second mandibular bicuspid with 6-10 mm of lateral variability. The mental nerve ramifies to supply the lower lip skin down to the labiomental fold and, occasionally, down the chin as well. This nerve is located in the submucosa as it exits the foramen and is frequently visible in this location.
Studies have highlighted additional aspects of lip innervation. Proprioceptive fibers associated with mechanoreceptors (e.g., Merkel cells and Meissner's corpuscles) are present in both lips, contributing to the fine tactile sensitivity essential for speech and oral function. Mechanosensitive ion channels such as PIEZO2 have been identified in the sensory corpuscles within lip tissues, playing a role in detecting mechanical stimuli such as pressure or stretch. [14]
Muscle Groups
Knowledge pertaining to a structure called the modiolus is essential for understanding the insertions of the lip musculature. The modiolus is a tendinous thickening at each commissure that serves as an attachment site for several of the upper and lower lip muscles. [15]
The perioral musculature can be classified into three groups based on insertion. Group I muscles insert into the modiolus, group II muscles insert into the upper lip, and group III muscles insert into the lower lip (see the image below).
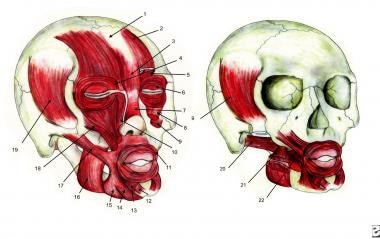 Facial muscles: 1) Galea aponeurotica, 2) Frontalis, 3) Procerus, 4) Depressor supercilii, 5) Corrugator supercilii, 6) Orbicularis oculi, 7) Nasalis, 8) Levator labii superioris, 9) Levator anguli oris, 10) Levator labii superioris alaeque nasi, 11) Orbicularis oris, 12) Mentalis, 13) Depressor labii inferioris, 14) Depressor anguli oris, 15) Platysma, 16) Masseter, 17) Zygomaticus major, 18) Zygomaticus minor, 19) Temporalis, 20) Lateral pterygoid, 21) Medial pterygoid, 22) Buccinator.
Facial muscles: 1) Galea aponeurotica, 2) Frontalis, 3) Procerus, 4) Depressor supercilii, 5) Corrugator supercilii, 6) Orbicularis oculi, 7) Nasalis, 8) Levator labii superioris, 9) Levator anguli oris, 10) Levator labii superioris alaeque nasi, 11) Orbicularis oris, 12) Mentalis, 13) Depressor labii inferioris, 14) Depressor anguli oris, 15) Platysma, 16) Masseter, 17) Zygomaticus major, 18) Zygomaticus minor, 19) Temporalis, 20) Lateral pterygoid, 21) Medial pterygoid, 22) Buccinator.
Group I muscles consist of the following:
-
Orbicularis oris
-
Buccinator
-
Levator anguli oris
-
Depressor anguli oris
-
Zygomaticus major
-
Risorius
Group II muscles consist of the following:
-
Levator labii superioris
-
Levator labii superioris alaeque nasi
-
Zygomaticus minor
Group III muscles consist of the following:
-
Depressor labii inferioris
-
Mentalis
-
Platysma
Group I Muscles
Orbicularis oris
The orbicularis oris forms a sphincter around the mouth. This muscle purses the lips and presses them against the teeth upon contraction. It is divided into two main parts: a superficial, marginal layer with longitudinal fibers and a deeper, peripheral layer of circular fibers. The muscle's actions include closing the mouth, puckering the lips, and facilitating speech and facial expressions. Its intricate structure allows fine movements through contributions from the radiating perioral muscles. The marginal and peripheral fibers work together to achieve the unique dynamic actions required for articulation and expressions. [1]
The superficial portion of the orbicularis oris receives fibers from several other perioral muscles that insert into the orbicularis to provide fine movements of the lips. The deep orbicularis oris is responsible for the sphincteric action of the lips.
In a cross-section, the orbicularis oris is composed of a long, vertical segment that curls outward at the superior and inferior free margins to form a marginal protrusion. The buccal and marginal mandibular nerves provide motor innervation to the orbicularis oris from its deep surface. In the upper lip, the orbicularis oris fibers decussate in the midline and have dermal insertions approximately 4-5 mm lateral from the midline, sparing the central region. This serves to pull the skin medially at these dermal insertion points, forming the philtral columns. The central region between the philtral columns is devoid of dermal attachments and is pulled into a concave depression.
Buccinator
The buccinator arises from the posterior alveolar process of the maxilla, the pterygomandibular raphe, and the body of the mandible and inserts into the modiolus. It functions to press the lips and cheek against the teeth. The buccinator receives motor innervation from the buccal branches of the facial nerve that enter the muscle on its superficial surface. The parotid duct pierces the buccinator after it crosses the anterior edge of the masseter muscle.
Levator anguli oris
The levator anguli oris arises from the canine fossa of the maxilla beneath the infraorbital foramen and descends vertically to insert into the modiolus. Its action is to superiorly elevate the commissure. The buccal and zygomatic branches of the facial nerve innervate this muscle. These branches enter the muscle on its superficial surface. The facial artery and infraorbital nerve travel in a plane on the superficial surface of the muscle. Notably, its superficial relationship with the facial artery and infraorbital nerve makes it clinically relevant during surgical or dental procedures. [1]
Depressor anguli oris
The depressor anguli oris arises from the oblique line on the anterior mandible below the canine and premolar teeth. Its fibers pass superiorly and twist medially to insert on the modiolus. The marginal mandibular branch of the facial nerve supplies the depressor anguli oris and enters the muscle on its deep surface. The depressor anguli oris functions to depress and laterally move the commissure.
Zygomaticus major
The zygomaticus major arises from the zygomatic bone just anterior to the zygomaticotemporal suture line and passes inferiorly and medially over the buccinator and levator anguli oris to insert on the modiolus. Superiorly, its fibers are deep to the orbicularis oculi muscle. Inferiorly, the fibers are superficial to the facial vessels and facial nerve. The zygomatic and buccal branches of the facial nerve supply the zygomaticus major from its deep surface. Upon contraction, this muscle elevates and laterally moves the commissure.
Risorius
The risorius arises from the parotid fascia and passes medially and anteriorly in a transverse plane to insert on the modiolus. The buccal branch of the facial nerve enters the muscle on its deep surface, providing innervation. Upon contraction, the risorius draws the commissure laterally and produces a sardonic smile.
Group II Muscles
Levator labii superioris
The levator labii superioris is a paired, triangular muscle of facial expression belonging to the buccolabial group. [1] It arises from the inferior orbital rim on the maxilla, deep to the orbicularis oculi and superior to the infraorbital foramen. Its fibers pass inferiorly to insert into the dermis of the upper lip skin and into the orbicularis oris muscle. Upon contraction, the levator labii superioris elevates the upper lip. The buccal branch of the facial nerve innervates this muscle.
Levator labii superioris alaeque nasi
The levator labii superioris alaeque nasi arises from the frontal process of the maxilla. Its fibers pass inferiorly to insert on the lateral nasal alar cartilage, the dermis of the upper lip, and the orbicularis oris muscle. The buccal branch of the facial nerve innervates this muscle. Upon contraction, the levator labii superioris alaeque dilates the nostril and elevates the upper lip.
Zygomaticus minor
The zygomaticus minor arises from the zygoma deep to the orbicularis oculi and just lateral to the zygomaticomaxillary suture. Its fibers pass inferiorly to insert on the upper lip. The buccal branch of the facial nerve innervates this muscle. Upon contraction, the zygomaticus minor elevates and pulls the commissure laterally. Its contraction contributes to a nasolabial fold.
Group III Muscles
Depressor labii inferioris
The depressor labii inferioris arises from the anterolateral mandible and medial to the insertion of the depressor anguli oris. It lies deep to the depressor anguli oris. The fibers pass superiorly to insert in a fan shape into the lower lip dermis and orbicularis oris. The marginal mandibular branch of the facial nerve innervates this muscle. The depressor labii inferioris acts to depress the lower lip and pull it slightly laterally.
Mentalis
The mentalis muscle is a paired central muscle of the lower lip. This muscle arises from the incisive fossa of the mandible and descends to attach to the skin of the chin. [1] Intraorally, its insertion can be observed at the base of the midline gingivolabial sulcus, which deepens laterally to the centrally positioned muscle belly. Since its muscle fibers pass in an inferior direction, the action of the mentalis upon contraction is to elevate the lower lip. The insertion site of the mentalis fibers into the dermis can be observed in the pout expression. The marginal mandibular nerve innervates the mentalis.
Platysma
The platysma is a paired sheet of muscle in the anterior neck. It arises from the fascia overlying the pectoralis major and deltoid muscles and inserts on the inferior border of the anterior mandible. The fibers cross superiorly just before reaching the mandibular border. The platysma is a lip depressor. The cervical branch of the seventh cranial nerve innervates the platysma.
-
Lips and perioral region anatomy. Lymphatic drainage of the lips.
-
Facial muscles: 1) Galea aponeurotica, 2) Frontalis, 3) Procerus, 4) Depressor supercilii, 5) Corrugator supercilii, 6) Orbicularis oculi, 7) Nasalis, 8) Levator labii superioris, 9) Levator anguli oris, 10) Levator labii superioris alaeque nasi, 11) Orbicularis oris, 12) Mentalis, 13) Depressor labii inferioris, 14) Depressor anguli oris, 15) Platysma, 16) Masseter, 17) Zygomaticus major, 18) Zygomaticus minor, 19) Temporalis, 20) Lateral pterygoid, 21) Medial pterygoid, 22) Buccinator.
Tables

What would you like to print?
- Poor Oral Health Tied to Worse Brain Health
- Vaping Could Be as Dangerous to Oral Health as Cigarettes
- What's the Connection Between Diabetes and Oral Health?
-
 The Five Things Dentists Wished PCPs Weren't Missing
The Five Things Dentists Wished PCPs Weren't Missing
-
Not Enough Evidence for Primary Care to Routinely Conduct Dental Screenings
-
New Guideline for Managing Toothache in Kids




