Practice Essentials
Infantile hemangiomas are benign vascular neoplasms that have a characteristic clinical course marked by early proliferation and followed by spontaneous involution. Hemangiomas are the most common tumors of infancy and usually are medically insignificant. See the image below.
See 13 Common-to-Rare Infant Skin Conditions, a Critical Images slideshow, to help identify rashes, birthmarks, and other skin conditions encountered in infants.
Signs and symptoms
Infantile hemangiomas may be cutaneous or extracutaneous. Frequency of cutaneous hemangiomas at particular sites is as follows:
-
Head and neck - 60%
-
Trunk - 25%
-
Extremities - 15%
Sites of extracutaneous hemangiomas include the following:
-
Liver
-
Gastrointestinal tract
-
Larynx
-
Central nervous system
-
Pancreas
-
Gallbladder
-
Thymus
-
Spleen
-
Lymph nodes
-
Lung
-
Urinary bladder
-
Adrenal glands
Superficial cutaneous hemangiomas progress sequentially through the following stages:
-
Blanching of the involved skin
-
Occasionally (especially with lip and buttock lesions), a shallow ulceration
-
Fine telangiectasias
-
A red or crimson macule or papule, often surrounded by a faint halo of vascular blanching
Deep or subcutaneous hemangiomas present with a skin-colored or bluish-hued nodule, plaque, or tumor.
Combined superficial and deep hemangiomas have features of both locations.
Features are as follows:
-
Usual maximum size 0.5-5 cm
-
Range from the size of a pinhead to greater than 20 cm in diameter
-
Most remain well circumscribed and focal
-
A minority are segmental in nature and more extensive
Infantile hemangiomas characteristically exhibit early rapid growth followed by slow involution, as follows [1, 2, 3, 4] :
-
Rapid growth during the neonatal period (birth to 4 wk) is the historical hallmark of infantile hemangiomas
-
The hemangioma becomes elevated and dome shaped, lobulated, plaquelike, tumoral, or any combination of these morphologies
-
The most growth occurs during the first 4-6 months of life
-
Proliferation slows considerably between 6-12 months of life
-
Complete involution in 50% of infantile hemangiomas by age 5 years and 70% by age 7 years
-
Complete involution may take an additional 3-5 years in the remainder
See Clinical Presentation for more detail.
Diagnosis
Skin biopsy can be performed if the diagnosis is in question after a thorough history and physical examination. Infantile hemangiomas uniformly stain positively for glucose transporter 1 (GLUT-1) during both the proliferation and the involution phases.
The following laboratory studies have been investigated as possible markers of hemangioma proliferation and differentiation [5, 6] :
-
Serum and urinary vascular endothelial growth factor (VEGF)
-
Urinary beta-fibroblast growth factor
-
Urinary matrix metalloproteinases (MMPs)
Magnetic resonance imaging (MRI) has the following uses:
-
Delineate the location and extent of cutaneous and visceral hemangiomas
-
Differentiate proliferating hemangiomas from other high-flow vascular lesions (eg, arteriovenous malformations)
Features of ultrasonography are as follows:
-
Can help differentiate hemangiomas from other deep dermal or subcutaneous structures, (eg, cysts, lymph nodes)
-
Cannot fully evaluate the magnitude and extent of the hemangioma
-
High vessel density (>5 vessels/cm2) and high peak arterial Doppler shift (>2 kHz) are sensitive and specific for infantile hemangiomas, as compared with other soft tissue masses [7]
See Workup for more detail.
Management
The vast majority of infantile hemangiomas do not require any medical or surgical intervention. [8] Treatment options for clinically significant hemangiomas include the following:
-
Medication
-
Laser surgery
-
Surgical excision
Features of pharmacologic treatment are as follows:
-
The FDA has approved an oral pediatric formulation of propranolol hydrochloride (Hemangeol) for the treatment of proliferating infantile hemangiomas requiring systemic therapy
-
Corticosteroids can slow the growth and decrease the size of proliferating infantile hemangiomas
-
Oral corticosteroids are preferred over intralesional injection
Features of laser surgery treatment are as follows:
-
Flashlamp-pumped pulsed-dye laser most widely used
-
Pulsed-dye laser surgery effective for treating ulcerated hemangiomas and thin superficial hemangiomas
-
Many ulcerated hemangiomas respond with decreased pain (sometimes as early as a few days after the initial treatment), rapid reepithelialization, and hastened involution
-
Laser treatments generally performed every 2-4 weeks until complete healing results
-
Scarring or residual skin changes may occur
-
Laser treatment may worsen ulceration, particularly of deep or combined superficial and deep lesions
Features of surgical excision are as follows:
-
Not uncommonly used for correction of cutaneous defects from involuted hemangiomas [14]
-
Specially trained surgeons needed for surgical excision of proliferating hemangiomas because of the risk of hemorrhage and damage to vital structures
-
Early excision may save life, preserve vision, or eliminate a cosmetically disfiguring lesion
Background
Infantile hemangiomas are benign vascular neoplasms that have a characteristic clinical course marked by early proliferation and followed by spontaneous involution. During the proliferative phase in the neonatal period or early infancy, a rapidly dividing endothelial cell proliferation is responsible for the enlargement of infantile hemangiomas. Finally, an involutional phase occurs, whereby most infantile hemangiomas are clinically resolved by age 9 years.
Hemangiomas are the most common tumors of infancy, and most infantile hemangiomas are medically insignificant. Occasionally infantile hemangiomas may impinge on vital structures, ulcerate, bleed, cause high-output cardiac failure or significant structural abnormalities or disfigurement. Rarely, a cutaneous infantile hemangioma may be associated with one or more underlying congenital anomalies.
Pathophysiology
Infantile hemangiomas are composed of proliferating, plump endothelial cells. Early in proliferation, the cells are in disarray, but, with time, they form vascular spaces and channels replete with blood cells (see image below).
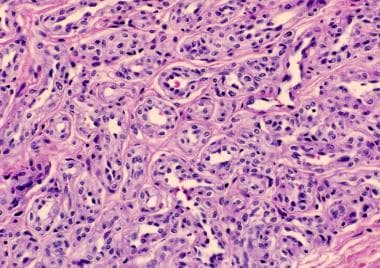 Histopathology of a proliferating infantile hemangioma with plump endothelial cells in the dermis.
Histopathology of a proliferating infantile hemangioma with plump endothelial cells in the dermis.
These benign-appearing endothelial cells produce limited basement membrane structures. Hemangiomas assume a lobular architecture as proliferation slows and ends. Mast cells appear to affect this process and are implicated in the promotion of feeding arterioles and veins that supply each lobule. They also have been found in high concentrations during involution.
Takahashi hypothesized that during the third trimester of fetal development, immature endothelial cells coexist with immature pericytes, which maintain their proliferative capacity for a limited period during postnatal life. [9] Angiogenic peptides, such as beta-fibroblast growth factor, vascular endothelial growth factor (VEGF), and proliferating cell nuclear antigen, induce proliferation of these immature cells, resulting in the development of the hemangioma. As the endothelial cells differentiate, an influx of mast cells, various myeloid cells, and tissue inhibitors of metalloproteinases (TIMPs) occurs. [15] TIMPs, along with interferon and transforming growth factor produced by the mast cells, terminate the endothelial cell proliferation and passively induce involution by senescence of endothelial cells.
Etiology
Neither the cause nor the cell of origin of infantile hemangiomas has been definitively elucidated. Theories abound and several lines of evidence support several divergent theories of the cell of origin, including placental tissue, endothelial progenitor cells (EPCs), and mesenchymal stem cells. [16]
A distinct group of tissue-specific markers, including Lewis Y, merosin, and FcγRII, but most notably glucose transporter 1 (GLUT-1), are uniquely coexpressed by hemangiomas and placental microvessels, suggesting a unique relationship between hemangiomas and placental microvessels. Two theories postulated to explain this observation include (1) colonization of receptive mesenchyme by potentially abnormal angioblasts switched toward a placental endothelial phenotype and (2) embolic placental endothelial cells that have reached fetal tissues from chorionic villi through right-to-left shunts.
The placenta and hemangioma share a similar life cycle of robust vascular growth. The placenta produces very high levels of the proangiogenic cytokine, vascular endothelial growth factor (VEGF). As a protective mechanism against uncontrolled angiogenesis in the fetus and mother, a soluble form of the VEGF receptor, sFlt-1, found in both amniotic fluid and maternal serum, is also produced by the placenta. sFlt-1 binds circulating VEGF, preventing excessive angiogenesis in nonplacental tissues. Postpartum, the connection to the placenta and sFlt-1 is removed, abrogating this negative feedback and allowing proliferation of cells, such as those in hemangiomas, responsive to VEGF. [17, 18]
Hemangiomas fail to stain for numerous trophoblastic markers, somewhat discounting the placental embolism theory. [19] Some reports suggest that infants born to mothers who have undergone chorionic villus sampling may be at an increased risk of developing hemangiomas, but this has not been uniformly observed. [20] One model suggests that infantile hemangiomas result from aberrantly displaced or embolized placental chorionic villous mesenchymal core cells into the fetus. These cells give rise to a primitive mesoderm-derived hemogenic endothelium that has a neural crest phenotype, which is regulated by the renin-angiotensin system. This hemogenic endothelium differentiates into neuroglial, mesenchymal, and hematopoietic stems cells as well as endothelial progenitor cells (EPC). During infantile hemangioma proliferation and stimulated by angiotensin II (ATII), the mesenchymal stem cells (MSC) produce VEGF, which stimulates the EPCs to grow, and osteoprotegerin (OPG), which prevents the apoptosis of the hemogenic endothelium, MSC, and EPC, creating an excitatory pathway from endothelial cell proliferation. [21] See Pathophysiology.
An in utero local tissue environment of hypoxia appears to influence the subsequent vasculature. [22] This microenvironmental condition is a potent inducer of angiogenesis, leading to increased production of hypoxia-inducible factor-1α (HIF-1α), which, in turn, causes VEGF gene transcription in association with cytokine-stromal cell-derived factor 1 (SDF-1). This appears to stimulate endothelial progenitor cells to proliferate and differentiate into endothelial cells. [23] The production of HIF-1α is stimulated by ATII, helping explain the effect of beta-blocker and angiotensin-converting enzyme inhibitor therapy in the accelerated involution of infantile hemangiomas, as both decrease ATII.
Several VEGF receptors (VEGFRs) may play a role in the development of hemangiomas. VEGFR1 on endothelial cells acts as a decoy receptor such that the binding of VEGF to this receptor does not effect a change in the endothelial cell. However, the binding of VEGF to VEGFR2 elicits robust endothelial cell proliferation and migration. Hemangioma endothelial cells exhibit low levels of VEGFR1, with marked constitutive activation of VEGFR2. Gene transcription for VEGFR1 in hemangioma cells is dependent on nuclear factor of activated T cells (NFAT). This, in turn, is dependent on a pathway involving beta1 integrin, VEGFR2, and integrinlike receptor tumor endothelial marker-8 (TEM8).
Missense mutations in genes encoding for VEGFR2 and TEM8 have been identified in a subset of infantile hemangiomas. These mutations are likely responsible for the constitutive activation of VEGFR2 and resultant hemangioma endothelial cell proliferation. Soluble VEGFR1 or anti-VEGF antibodies normalize the constitutive VEGFR2 signaling. Consequently, these or other similar molecules may be exploited in future hemangioma therapy. [24]
It is believed that infantile hemangiomas may be derived from endothelial progenitor cells (EPCs). EPCs are bone marrow-derived CD133 (or AC133)–positive, CD34-positive, and KDR (VEGFR-2)-positive pluripotent cells that demonstrate the ability to develop into Glut-1–positive endothelial cells. [25] A hemangioma model using these cells exhibits growth characteristics typical of an infantile hemangioma, with both proliferating and involuting phases and the development of fibrofatty residua during involution. The endothelial cells in an infantile hemangioma are thought to be primitive endothelial clonal cells that exhibit abnormal behavior. [26] Infantile hemangiomas express elevated levels of the embryonic stem cell reprogramming factors Oct4, Nanog, Sox2, and Klf4, similar to malignant tumors, suggesting that at least a subpopulation of cells with stem-cell properties exists within these lesions. [27]
Two possibly interrelated theories exist regarding the pathogenesis of hemangiomas with regard to the EPCs, intrinsic and extrinsic. The intrinsic theory proposes that EPCs are monoclonal and behave differently from normal endothelial progenitor cells. The extrinsic theory postulates that the EPCs are polyclonal and behave normally and proliferate in response to the surrounding tissue angiogenic and angiostatic factors. [28]
Mesenchymal stem cells may also play a role in the formation of infantile hemangiomas. These cells have been identified in hemangioma tissue. [29] Mesenchymal stem cells retain the capacity to differentiate into numerous mesodermal cells, including adipocytes, suggesting that these cells may be the source of the resultant adipose tissue found in involuted hemangiomas.
Evidence to support a hereditary/genetic component in the development of most infantile hemangiomas is minimal; most appear to be sporadic. However, at least one report described a kindred in which infantile hemangiomas may be the result of an autosomal dominant trait. [30] These infantile hemangiomas were seen in association with an increased incidence of vascular malformations (mostly capillary malformations) in various members of the same family.
Epidemiology
United States
Infantile hemangiomas occur in approximately 3% and 10% of white infants at birth and at age 1 year, respectively. [3, 4] Female, white, non-Hispanic newborns are more likely to be diagnosed with infantile hemangiomas. The incidence has increased in this cohort over the past several decades, likely reflecting the greater increase in prematurity in this population over the same period. [31, 32] The incidence of infantile hemangiomas is approximately 22-30% of preterm infants with birthweight less than 1 kg; for preterm infants with birthweight greater than 1.5 kg, [33] the incidence is the same as for term infants. An increased incidence is recognized in infants from multiple gestations.
The incidence is increased with older maternal age, maternal placenta previa, and preeclampsia. [34] Some, but not all, surveys have demonstrated increased incidence in infants born to mothers who have undergone prenatal chorionic villus sampling.
Race
Hemangiomas occur most commonly in white infants, with an incidence rate 10-12 times that of black and Asian infants.
Sex
Females are affected more often than males by a ratio of 3:1. This disparity is higher (9:1) in those infants with large cervicofacial segmental hemangiomas associated with PHACE syndrome.
Age
Thirty percent of infantile hemangiomas are present at birth, and 70% of them initially appear in the first several weeks of life.
Mortality/Morbidity
Most infantile hemangiomas are benign and do not cause any morbidity or mortality. Occasionally, they may impinge on vital structures and interfere with breathing, vision, eating, or hearing. Ulceration of certain areas (eg, diaper area, neck, mucosal surfaces) is not uncommon. Excessive bleeding is infrequent and rarely, if ever, life threatening. In the past, infantile hemangiomas were confused with other vascular neoplasms, particularly kaposiform hemangioendothelioma and tufted angiomas, which can incite a consumptive coagulopathy that may be life threatening. This is referred to as Kasabach-Merritt phenomenon (KMP). Infantile hemangiomas are not responsible for KMP. [35, 36]
Large cutaneous or visceral hemangiomas (particularly liver) can result in high-output cardiac failure resulting from increased vascular flow. Permanent significant structural abnormalities may result, particularly when facial structures are involved. The highest risk appears to be with involvement of the nasal tip, lips, and ears. [37] Segmental hemangiomas, which cover a particular section or area of skin, may be markers for underlying malformations or developmental anomalies of the heart, blood vessels, or nervous system (PHACE and PELVIS syndromes [see below] and lumbosacral hemangiomas) and, depending on the severity of the associated anomaly, can result in increased morbidity or mortality. [38, 39]
PHACE syndrome (see image below) is a multiple-congenital-anomaly syndrome composed of posterior fossa structural brain abnormalities (Dandy-Walker malformation and various forms of hypoplasia); hemangiomas of the face, head, and neck (segmental, >5 cm in diameter); arterial lesions (especially carotid, cerebral, and vertebral); cardiac anomalies (coarctation of the aorta in addition to many other structural anomalies); eye abnormalities; and, rarely, associated midline ventral defects such as sternal cleft or supraumbilical raphe). A consensus statement with detailed diagnostic criteria for both PHACE and possible PHACE syndromes was published in 2009. [40]
 Segmental infantile hemangioma in a female infant with PHACE syndrome involving the posterior neck and right forehead associated with an absent right vertebral artery and a laryngeal hemangioma.
Segmental infantile hemangioma in a female infant with PHACE syndrome involving the posterior neck and right forehead associated with an absent right vertebral artery and a laryngeal hemangioma.
PELVIS (or SACRAL) syndrome (see image below) is perineal hemangioma with any of the following: external genital malformations, lipomyelomeningocele, vesicorenal abnormalities, imperforate anus, and/or skin tags.
 Segmental infantile hemangioma with minimal or arrested growth of the bilateral buttocks and posterior thigh in this male infant with PELVIS syndrome (complicated by cutaneous ulceration, hypospadias, anal stenosis, intraspinal lipoma with tethered cord). The white material is a barrier diaper cream.
Segmental infantile hemangioma with minimal or arrested growth of the bilateral buttocks and posterior thigh in this male infant with PELVIS syndrome (complicated by cutaneous ulceration, hypospadias, anal stenosis, intraspinal lipoma with tethered cord). The white material is a barrier diaper cream.
Prognosis
The prognosis for most uncomplicated infantile hemangiomas is very good, with complete involution of 50% by age 5 years, 70% by age 7 years, and 90% by age 9 years. Despite resolution of the vascular component, residual skin changes are observed in roughly 50% of cases. Of hemangiomas that have involuted by age 6 years, 38% still have residual evidence with scar formation, telangiectasia, or redundant or anetodermic skin. Hemangiomas that take longer to involute have a higher incidence of permanent cutaneous residua. Eighty percent of lesions that complete involution after age 6 years may exhibit significant cosmetic deformities. An increased incidence of permanent residua exists when the lip, nasal tip, eyelid, and ear are involved.
Patient Education
Educating parents about the variable natural history, prognosis, risks, and benefits of potential treatments and possible complications is essential. [41] Emotional support should be offered for parents of children with severe or complicated hemangiomas. Birthmarks: A Guide to Hemangiomas and Vascular Malformations by Milton Waner, MD, a book for parents and caregivers of children with vascular lesions, can be quite helpful. The Vascular Birthmarks Foundation is a useful source for accurate information for patients and family members. The Yale Infantile Hemangioma Web site provides photos depicting the natural progression of infantile hemangiomas over the course of years. Use of educational tools like this can assist in alleviating caregiver concern, while improving understanding of the natural progression. [42]
-
Histopathology of a proliferating infantile hemangioma with plump endothelial cells in the dermis.
-
This proliferating superficial infantile hemangioma on the trunk required no therapy.
-
Exquisitely painful ulcerated mixed hemangioma (superficial and deep) of the left deltoid in a 6-month-old female infant. This lesion was treated successfully with pulsed dye laser.
-
This superficial and deep infantile hemangioma resulted in astigmatism of the left eye, requiring spectacles to correct the refractive error and to prevent amblyopia. Further growth of this hemangioma necessitated a course of oral prednisolone. The hemangioma shrunk rapidly, and the patient's astigmatism decreased such that the spectacles were unnecessary 1 month after beginning steroids.
-
Segmental infantile hemangioma in a female infant with PHACE syndrome involving the posterior neck and right forehead associated with an absent right vertebral artery and a laryngeal hemangioma.
-
Segmental infantile hemangioma with minimal or arrested growth of the bilateral buttocks and posterior thigh in this male infant with PELVIS syndrome (complicated by cutaneous ulceration, hypospadias, anal stenosis, intraspinal lipoma with tethered cord). The white material is a barrier diaper cream.
-
Superficial proliferating infantile hemangioma on the lower extremity
