Background
Sebaceous glands are part of epidermal appendages. Neoplasms of the sebaceous glands may be benign, such as sebaceous hyperplasia or sebaceous gland adenomas. The malignant sebaceous gland carcinoma most commonly arises in the periocular area. [1, 2] Fewer than 120 cases of sebaceous cell carcinoma have been reported at extraocular sites. The most common site of origin is the meibomian glands of the eyelids, leading to the term meibomian gland carcinoma. [1] However, this neoplasm can occur in other sebaceous glands, such as in the caruncle, the glands of Zeis, and in the eyebrow. Sebaceous cell carcinoma is a lethal eyelid malignancy and can masquerade as benign conditions. Error or delay in diagnosis is common, and this tumor carries a significant mortality rate with metastasis.
History of the Procedure
This type of tumor has been confused with other tumors, both clinically and histologically. [1]
Epidemiology
Frequency
From 2000 through 2016, sebaceous carcinoma had an overall incidence of 2.4 cases per million individuals, with an average of 800 cases per year in the United States. The incidence was higher in males (3.5 cases per million) compared to females (1.7 cases per million) and increased with age, with the highest incidence seen in individuals aged 80 years and older (22.7 cases per million). Additionally, 78% of cases were reported in non-Hispanic Whites, who had approximately four times the incidence rate compared to African Americans. [3]
In a retrospective study, 31 patients were diagnosed with sebaceous cell carcinoma of the ocular adnexa on histopathology. Twenty (65%) of the patients were women and 11 were men. The upper eyelid was involved in 18 patients, the lower eyelid in 10, the upper and lower eyelids in 1, and the caruncle in 2. [4]
Although sebaceous cell carcinomas are more common in elderly patients, they may be seen in younger patients with a history of radiation to the face.
Etiology
In the periocular area, the most common sites for sebaceous carcinoma typically are the Meibomian glands, which are specialized sebaceous glands. However, tumors also can originate from the Zeiss glands and sebaceous glands in the ocular caruncle. [1]
Pathophysiology
Sebaceous cell carcinoma may mimic either chalazion or chronic blepharitis. [1] It tends to invade locally, as well as spreading to regional lymph nodes. Sebaceous cell carcinomas may grow in nests with central necrosis. The intraepithelial spread may lead to the erroneous histologic diagnosis of epithelial dysplasia or carcinoma in situ.
Foamy cytoplasm is seen only in sebaceous carcinoma, but it is absent in conjunctival or cutaneous squamous cell carcinoma. It also can histologically mimic basal cell carcinoma, squamous carcinoma, or Merkel cell tumor.
Either fresh tissue or formalin-fixed tissue not exposed to alcohol can be frozen, and positive fat stains, such as oil red O, can confirm the diagnosis of sebaceous carcinoma.
Presentation
The clinical appearance of sebaceous gland carcinoma is highly variable. They simulate such benign conditions as chalazion, blepharoconjunctivitis, keratitis, and other malignant or benign skin lesions.
Many of the skin tumors have a predilection for the upper eyelid and have a yellowish appearance. Tumors at the eyelid margin commonly cause loss of eyelashes. Classically, this lesion is a firm, painless, indurated mass or ulceration associated with the loss of cilia, in an area that has been treated for recurrent chalazia.
Both the history and the presentation of sebaceous cell carcinoma are variable. Typically, there is an insidious onset of a painless firm eyelid mass. This mass easily can appear clinically as a recurrent or chronic chalazion. Sebaceous cell carcinoma also can mimic unilateral blepharoconjunctivitis, meibomitis, basal or squamous cell carcinoma, conjunctival or corneal carcinoma in situ, orbital inflammation, or superior limbic keratoconjunctivitis.
Sebaceous cell carcinoma is shown in the images below.
 A 63-year-old white man with lower eyelid sebaceous cell carcinoma and lash loss is shown.
A 63-year-old white man with lower eyelid sebaceous cell carcinoma and lash loss is shown.
 Gross pathology slide of sebaceous cell carcinoma, from same man as seen in image above.
Gross pathology slide of sebaceous cell carcinoma, from same man as seen in image above.
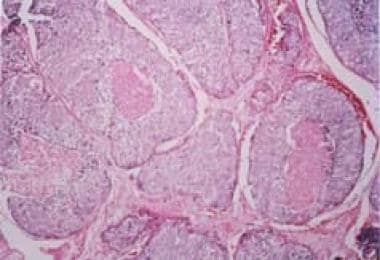 Microscopic pathology slide of sebaceous cell carcinoma, from same man as seen in images above.
Microscopic pathology slide of sebaceous cell carcinoma, from same man as seen in images above.
Indications
Perform a biopsy on all recurrent or resistant chalazia, as well as new nonresolving lesions of the eyelid.
Relevant Anatomy
Sebaceous tumors of the eyelid may arise from meibomian glands, Zeis glands, or glands associated with the caruncle.
The meibomian glands originate in the tarsus and number approximately 25 in the upper eyelid and 20 in the lower eyelid. They are oil-producing sebaceous glands. A chalazion is an inflammation caused by obstruction of the meibomian glands and occasionally can be confused with sebaceous cell carcinoma.
Zeis glands are small, modified, sebaceous glands that open into the hair follicles at the base of the eyelashes.
Contraindications
There are no contraindications. This tumor can masquerade as other tumors, both benign and malignant.
Prognosis
Sebaceous carcinoma is a fast-growing form of skin cancer that has a 5-year survival rate of 78% for localized/regional disease and 50% for metastatic disease. The incidence of this cancer has been on the rise in the United States for many years, but the factors contributing to this increase are not fully understood. [3]
Aside from its aggressive nature, sebaceous carcinoma can lead to substantial treatment-related complications owing to the fact that these tumors primarily develop on the head and neck. Management often involves complex facial reconstruction and radiotherapy, further adding to the potential morbidity associated with the disease. [3]
-
A 63-year-old white man with lower eyelid sebaceous cell carcinoma and lash loss is shown.
-
Gross pathology slide of sebaceous cell carcinoma, from same man as seen in image above.
-
Microscopic pathology slide of sebaceous cell carcinoma, from same man as seen in images above.
Tables

What would you like to print?
- Immunotherapy Reduces Skin Cancer Precursors
- 'Superclinic' Powers Through Skin Cancer Referrals
- Darker Skin Tones Underrepresented on Skin Cancer Education Websites
-
 Response to Neoadjuvant Therapy in Desmoplastic Melanoma
Response to Neoadjuvant Therapy in Desmoplastic Melanoma
-
How Can Clinicians Address the Impact of Financial Toxicity on Cancer Survivors?
-
European Academy of Dermatology and Venereology (EADV) 2024 Congress





