Practice Essentials
Human papillomavirus (HPV) produces epithelial tumors of the skin and mucous membranes. The current classification system for HPV, which is based on similarities in genomic sequences, generally correlates with the 3 clinical categories applied to HPV infection [1] :
-
Anogenital or mucosal (further subclassified as latent [asymptomatic], subclinical, or clinical)
-
Nongenital cutaneous
-
Epidermodysplasia verruciformis (see the images below)
 Human papillomavirus (HPV). Verrucae and papillomas appear as frondlike epithelial proliferations. Verrucae tend to be more keratinized with sharper projections than papillomas.
Human papillomavirus (HPV). Verrucae and papillomas appear as frondlike epithelial proliferations. Verrucae tend to be more keratinized with sharper projections than papillomas.
 Human papillomavirus (HPV). Verruca vulgaris on the lateral border of the tongue exhibits the multiple, sharp-tipped, white, verrucous appearance, which is classic for this lesion in the oral cavity. Not all verrucae are so clinically diagnostic. Courtesy of Rose Yin Geist, DDS.
Human papillomavirus (HPV). Verruca vulgaris on the lateral border of the tongue exhibits the multiple, sharp-tipped, white, verrucous appearance, which is classic for this lesion in the oral cavity. Not all verrucae are so clinically diagnostic. Courtesy of Rose Yin Geist, DDS.


Signs and Symptoms
The clinical history and presentation of HPV infection vary depending on the anatomic area involved. The preference of certain viral genotypes for specific epidermal sites largely determines the areas of involvement. Conditions associated with HPV include the following [1] :
-
Anogenital warts (condylomata acuminata): Typically found near moist surfaces (eg, perianal area, vaginal introitus, vagina, labia, and vulva) but also may occur on dry surfaces (eg, penile shaft). These warts can be smooth and papular or keratotic. They generally are not painful but can be associated with pruritus or bleeding.
-
Cervical disease: Includes low-grade squamous intraepithelial lesion (LGSIL) and high-grade squamous intraepithelial lesion (HGSIL).
-
Anal cancer: About 50% of homosexual men with anal squamous cell carcinoma (SCC) have a history of anorectal warts. In contrast, only 20% of women with SCC and non-homosexual men have this history.
-
Nonanogenital mucosal disease: Includes oral warts, respiratory papillomas, and focal epithelial hyperplasia (Heck disease).
-
Nongenital cutaneous disease: Includes common cutaneous warts (verruca vulgaris), flat warts (verruca plana), and Bowenoid papulosis.
-
Epidermodysplasia verruciformis.
Physical findings vary depending on the tissues involved and may include the following [1] :
-
Typical condylomata: Discrete, papillary, cauliflower-like lesions involving multiple sites on moist surfaces.
-
Keratotic warts: Often seen on dry surfaces such as the labia majora.
-
Discrete papules: 1-3 mm in size can present on the shaft of the penis.
-
Cervical intraepithelial lesions: May be found upon examination of the cervix.
-
Subclinical infection: Tiny, slightly raised areas felt or visualized on the vagina or cervix.
See Clinical Presentation for more detail.
Diagnosis
Diagnosis of most cutaneous and external genital warts typically can be achieved through clinical examination or by applying acetic acid and conducting a biopsy. In cases of genital intraepithelial neoplasia, it is crucial to assess the extent of the disease through meticulous inspection and colposcopy.
Laboratory studies that may be considered include the following [2] :
-
Cervical cytologic testing with the Papanicolaou (Pap) test to screen for cervical neoplasia (current guidelines recommend delaying initiation and extending intervals between subsequent screens). [2]
-
HPV DNA testing (eg, Hybrid Capture II or polymerase chain reaction [PCR] assay) for detecting HPV and post-treatment follow-up of cervical intraepithelial neoplasia.
The acetic acid test may be used in conjunction with colposcopy to examine suspicious cervical lesions, but it is not recommended for routine screening. [1]
In certain cases, tissue biopsy may be necessary to confirm HPV infection. Biopsy is recommended in the following scenarios [1] :
-
Women with a history of vulvar dysplasia.
-
Postmenopausal women.
-
Cases where medical therapy fails.
-
When there is clinical doubt about the diagnosis.
Histologic findings useful for diagnosing include [1] :
-
Common cutaneous warts: Marked hyperkeratosis, acanthosis, parakeratosis, and papillomatosis. Koilocytes, vertical columns of parakeratosis, and foci of clumped keratohyaline granules distinguish warts from other papillomas.
-
Condyloma acuminatum: Epidermal disruption with hyperkeratosis, coarse keratohyaline granules, and koilocytes in a prominent granular layer. Flat condylomata exhibit acanthosis in the epidermis or mucosa.
Bowenoid papulosis: Psoriasiform hyperplasia and hyperkeratosis of the epidermis, increased mitotic figures at all epidermal levels, and keratinocytes with enlarged pleomorphic and hyperchromic nuclei.
See Workup for more detail.
Management
All medications used to treat HPV disease are applied topically and should not be applied to mucosal surfaces. They are not suitable for treating dysplastic lesions, squamous cell carcinoma, verrucous carcinoma, or Bowenoid papulosis. Medications fall into the following two broad categories:
- Immune response modifiers: Examples include imiquimod and interferon alfa. These primarily are used for treating external anogenital warts or condylomata acuminata.
- Cytotoxic agents: These include antiproliferative drugs such as podofilox, podophyllin, and 5-fluorouracil (5-FU), as well as chemodestructive or keratolytic agents like salicylic acid, trichloroacetic acid (TCA), and bichloracetic acid (BCA). The latter are recommended for treating nongenital cutaneous warts.
Sinecatechins ointment is another treatment option.
Surgical interventions commonly are considered for cases with a large number of warts, extensive affected areas, or refractory disease. Physical destruction or excision generally has proven more effective than medical therapy. Primary surgical options include the following:
-
Cryosurgery
-
Electrosurgery (electrodesiccation or loop electrosurgical excision procedure [LEEP])
-
Simple surgical excision using a scalpel, scissors, or curette
Alternative surgical procedures include the following:
-
Carbon dioxide laser ablation
-
Cavitron Ultrasonic Surgical Aspiration (CUSA)
-
Mohs surgery
Vaccines are available for preventing HPV infection, with recommended vaccination schedules established.
See Treatment and Medication for more detail.
Background
HPV produces epithelial tumors of the skin and mucous membranes. There are over 100 known HPV types, with genomes of more than 80 fully sequenced. Individuals with multiple sexual partners or persistent HPV infections are at higher risk of acquiring additional HPV strains. [3, 4, 5, 6] The current classification system, based on genomic similarities, generally corresponds to three clinical categories of HPV:
- Anogenital or mucosal
- Nongenital cutaneous
- Epidermodysplasia verruciformis (EV)
Mucosal HPV infections are classified as latent (asymptomatic), subclinical, or clinical. Clinical lesions are visibly apparent, whereas latent infections are detectable only through viral DNA tests. Subclinical lesions are identified using 3-5% acetic acid and magnification. Most HPV infections are latent; clinically visible infections typically manifest as warts rather than malignancies. [1]
HPV infections are common and result in various clinical manifestations on epidermal surfaces. Condylomata acuminata (genital warts) are benign proliferations of anogenital skin and mucosa caused by HPV infection. They are transmitted through sexual contact, with approximately two thirds of exposed individuals developing genital warts. The incubation period is estimated to be between 3 weeks and 8 months. [7, 8]
Although generally benign, certain HPV types can significantly increase the risk for anogenital cancer. [9, 10, 11] Some types also are associated with laryngeal, oral, and certain lung cancers.
HPV types 6 and 11 typically are classified as low-risk due to their low oncogenic potential, often causing condylomata and low-grade precancerous lesions. HPV types 16 and 18 are considered high-risk as they are responsible for most high-grade intraepithelial lesions that may progress to carcinomas, particularly in anogenital or mucosal regions.
HPV infection alone does not lead to malignant transformation of infected tissue. Co-factors such as tobacco use, ultraviolet radiation, pregnancy, folate deficiency, and immune suppression are implicated in this process. [1]
Physicians' understanding of HPV's natural history has significantly advanced in the last 2 decades, yet key questions remain unanswered. Areas needing further research include age-specific HPV outcomes, the likelihood of disease progression or regression, and factors. [12]
Pathophysiology
Papillomaviruses are nonenveloped viruses with icosahedral symmetry, characterized by 72 capsomeres that enclose a genome of double-stranded circular DNA, approximately 8000 base pairs long. Their genome is divided into the following three major functional regions:
- Early (E) region: Codes for six nonstructural genes, several of which are associated with cellular transformation.
- Late (L) region: Codes for two structural proteins, L1 and L2, that form the capsid.
- Long control region: A noncoding region that regulates replication and gene function.
Papillomaviruses are highly species-specific and do not infect other species, even under laboratory conditions. Humans are the only known reservoir for HPV. Papillomaviruses have never been cultured in vitro but have been characterized through molecular methods. These viruses are classified based on the molecular similarity of their genetic material and are assigned genotype numbers.
Although some overlap exists, most papillomaviruses have distinct anatomic preferences, infecting specific epidermal sites such as the skin or genital mucosa. The virus can integrate into host DNA, often resulting in the loss of early regulatory functions.
HPV infects basal keratinocytes of the epidermis, typically through disruptions of the skin or mucosal surface. In this location, the virus remains latent as a circular episome in low copy numbers. Autoinoculation of the virus into adjacent lesions is common. HPV infection spreads through skin-associated contact rather than blood-borne transmission. Cell-mediated immunity (CMI) plays a significant role in wart regression; patients with CMI deficiency are particularly susceptible to HPV infection and are notoriously difficult to treat. [13]
Papillomaviruses are thought to have two modes of replication:
- Stable replication: The episomal genome replicates in basal cells.
- Runaway (vegetative) replication: In more differentiated cells, generating progeny virus.
As epidermal cells differentiate and migrate to the surface, the virus undergoes replication and maturation. At the keratinized layer, the virus is present in high copy numbers and is shed with exfoliated cells. This replication process alters the character of the epidermis, resulting in cutaneous or mucosal excrescences known as warts.
Note the figures below detailing the mechanisms of action for HPV.
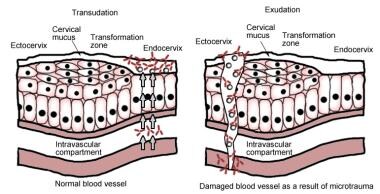 The left panel is transudation of serum antibodies to the site of human papillomavirus infection, and the right panel is exudation of serum antibodies to the site of human papillomavirus infection.
The left panel is transudation of serum antibodies to the site of human papillomavirus infection, and the right panel is exudation of serum antibodies to the site of human papillomavirus infection.
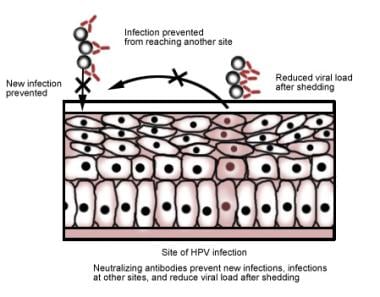 The figure shows proposed mechanisms used by the human papillomavirus vaccine to neutralize antibodies and protect against infection.
The figure shows proposed mechanisms used by the human papillomavirus vaccine to neutralize antibodies and protect against infection.
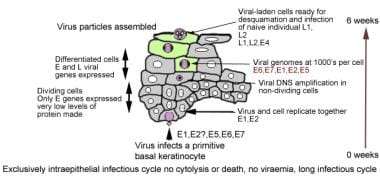 Figure showing how human papillomavirus penetrates the basal layer and eventually is released at the surface.
Figure showing how human papillomavirus penetrates the basal layer and eventually is released at the surface.
While all cells within a lesion contain the viral genome, the expression of viral genes is tightly linked to the cellular differentiation state. Most viral genes remain inactive until infected keratinocytes migrate out of the basal layer. Virus particles are only produced in highly differentiated keratinocytes, typically at the epithelial surface where these cells eventually shed into the environment.
HPV infections are non-cytolytic; instead, viral particles are released when desquamating cells degenerate. HPV can survive for months at low temperatures without a host, enabling transmission through barefoot contact in individuals with plantar warts.
Viral replication occurs exclusively within the nucleus, resulting in marked nuclear atypia in infected cells. Koilocytosis, characterized by perinuclear clearing (halo), a pyknotic nucleus, and a raisinoid appearance, is a hallmark of productive papillomavirus infection.
Several viral genotypes can induce cell transformation and are linked to epidermal malignancies. In benign or low-risk HPV lesions associated with types 6 and 11, the viral genome exists as circular episomal DNA separate from the host cell nucleus. In malignant lesions, high-risk types like HPV 16 and 18 typically integrate their genome into the host cell DNA, a key event in malignant transformation.
HPV proteins E6 and E7 from high-risk serotypes have been shown to deactivate host tumor suppressor proteins p53 and Rb, leading to unregulated host cell proliferation and malignant transformation.
Etiology
The definitive cause of anogenital warts is HPV infection. [9, 10, 11, 14] The HPV capsid lacks an envelope, which makes the organism very stable and resistant to various treatments. No serologic typing is available, because of the lack of consistent in vitro culture methods. Typing of HPV is based on genotype, which generally is determined by molecular hybridization using molecularly cloned HPV DNA of known type as the standard. Two HPV are of different types when their DNA hybridize (bind) less than 50% as efficiently to each other as to themselves.
The nearly 40 types of HPV that have been found in genital warts [15] are highly host-specific. These viruses do not infect laboratory animals and are not susceptible to acyclovir. In addition, HPV types demonstrate a high degree of site specificity, with some types only found on certain parts of the skin or mucous membranes. As a rule, HPV types causing common warts of the skin do not infect moist epithelium, and vice versa.
Multiple clinical associations with unique genotypes of HPV have been documented. Some of these associations are listed in the table below.
Table 1. Diseases Associated With Specific HPV Types (Open Table in a new window)
Nongenital Cutaneous Disease |
HPV Type |
Common warts (verrucae vulgaris) |
1, 2, 4, ,27,132,133,148,149,179,183 |
Plantar warts (myrmecias) |
1, 2, 4, 26,27,28,29,41,57,63,65,77,117,125,128,129,130,131 |
Flat warts (verrucae planae) |
3, 10, 27, 28, 38, 41, 49, 75, 76, 126 |
Butcher’s warts (common warts of people who handle meat, poultry, and fish) |
1-4, 7, 10, 28 |
Mosaic warts |
2, 27, 57 |
Ungual squamous cell carcinoma |
16 |
Epidermodysplasia verruciformis (benign) |
2, 3, 10, 12, 15, 19, 36, 46, 47, 50 |
Epidermodysplasia verruciformis (malignant or benign) |
5, 8-10, 14, 17, 20-25, 37, 38 |
Nonwarty skin lesions |
37, 38 |
Nongenital Mucosal Disease |
HPV Type |
6, 11 |
|
6, 11, 16, 18 |
|
Laryngeal papilloma (recurrent respiratory papillomatosis) [16] |
2, 6, 11, 16, 30, 40, 57 |
6, 11 |
|
Maxillary sinus papilloma |
57 |
Squamous cell carcinoma of the sinuses |
16, 18 |
Conjunctival papillomas |
6, 11,16 |
Conjunctival carcinoma |
16 |
Oral focal epithelial hyperplasia (Heck disease) |
13, 32 |
16, 18 |
|
16, 18 |
|
16, 18 |
|
Anogenital Disease |
HPV Type |
6,11,16,18,26,31,33,35,40,42,43,44,45,51,52,53,54,55,56,58,59,66,68,70,153,175,178,180,200,201,202 |
|
16, 18, 34, 39, 40, 42, 45 |
|
16, 18, 31, 34 |
|
Giant condylomata (Buschke-Löwenstein tumors) |
6, 11, 57, 72, 73 |
Unspecified intraepithelial neoplasia |
30, 34, 39, 40, 53, 57, 59, 61, 62, 64, 66-69 |
Low-grade squamous intraepithelial lesions (LGSIL) |
6, 11, 16, 18, 31,33,35,42,43,44,45,51,52,54,61,70,72,74 |
High-grade squamous intraepithelial lesions (HGSIL) |
6, 11, 16, 18, 31, 33, 43,35,39,42,44,45,51,52,56,58,66,67 |
6, 11, 16, 18 |
|
Carcinoma of vagina |
16 |
16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68, 70, 73, 82 |
|
Carcinoma of anus |
16, 31, 32, 33 |
Carcinoma in situ of penis (erythroplasia of Queyrat) |
16 |
16, 18 |
Risk Factors
HPV infection alone does not directly cause malignant transformation of infected tissue. However, cofactors such as tobacco use, ultraviolet radiation, pregnancy, folate deficiency, and immune suppression have been implicated in this process, particularly in the anogenital-mucosal category. Patients receiving immunosuppressive drugs and those with defects in cell-mediated immunity, including those infected with HIV, are especially susceptible to HPV infections. [1]
Sexual Activity:
There is a direct correlation between anogenital HPV infection and measures of sexual activity, such as the age of first intercourse and the lifetime number of sexual partners.
Women with a history of high-grade squamous intraepithelial lesions (HGSIL) of the cervix or invasive squamous cell carcinoma (SCC) of the cervix are at increased risk for subsequent development of invasive cancer in other tissues of the anogenital-mucosal category, particularly vaginal and anal carcinoma (relative risks of 5.6 and 4, respectively).
Anal cancer has been strongly associated with male homosexuality and specific male practices, such as engaging in receptive anal intercourse; the relative risk is 33. However, the overall disease prevalence is higher in women than in men, with a female-to-male ratio of 1.5:1.
Tobacco Smoking:
Women who smoke tobacco have an increased risk of developing cervical neoplasia. Measurable amounts of potent carcinogens, as well as several compounds from cigarette smoke, have been identified in the cervical mucus of females who smoke. These agents likely contribute to the increased prevalence of HPV malignant transformation observed in tobacco users.
Oral Contraceptive Use:
Women who take oral contraceptives for longer than 5 years have an increased relative risk of developing cervical carcinoma. This risk declines after discontinuation of oral contraceptive use, and no increased risk is demonstrated in women who took these agents for less than 5 years.
Chewing Indian Betel Quid:
A high incidence of oral cancer associated with HPV infection has been demonstrated in India among patients who chew betel quid. This stimulant, made from the leaves of the betel plant, is used similarly to chewing tobacco.
Ultraviolet and x-ray irradiation
Epidermodysplasia verruciformis (EV) is particularly susceptible to ultraviolet (UV) and x-ray irradiation; therefore, patients with EV should avoid activities that unnecessarily expose them to these forms of radiation.
Epidemiology
United States Statistics
Human papillomavirus (HPV) is the most common sexually transmitted infection in the United States. Each year, approximately 33,700 cancers in the United States are caused by HPV. These include 12,900 oropharyngeal cancers among men and women, 10,800 cervical cancers among women, and 6,000 anal cancers among men and women. Vaginal, vulvar, and penile cancers are less common. [19] The United States does not have a reporting system for HPV infections. HPV infections and the development of warts are common throughout life. Generally, genital HPV infection is considered to have become significantly more frequent over the past several decades.
Lewis et al reported the estimated prevalence and incidence of disease-associated HPV types among 15–59-year-olds in the United States. [20] In the 15–59 year age group, the prevalence of any HPV infection from 2013 to 2016 was 40.0% overall, 41.8% among males, and 38.4% among females, totaling 77.3 million individuals overall, with 40.5 million males and 37.0 million females having a prevalent HPV infection in 2018. The prevalence of disease-associated HPV infection was 22.0% overall, 24.2% in males, and 19.9% in females, amounting to 42.5 million individuals, with 23.4 million males and 19.2 million females having an infection of at least one disease-associated HPV type in 2018.
In the United States, young adults aged 15-24 years account for approximately half of new HPV infections each year. [21] The frequency of genital infections is associated with the number of sexual partners and the age of sexual debut. Patients receiving immunosuppressive drugs and those with defects in cell-mediated immunity, including those infected with HIV, are especially susceptible to developing HPV infections.
Using data and self-collected cervicovaginal specimens from 4,150 females in four consecutive National Health and Nutrition Examination Surveys (2003-2006), Hariri et al found HPV present in 42.5% of US females aged 14-59 years. The highest rate of infection was among young females aged 20-24 years. [22]
The population-based incidence of genital warts was estimated at 106 cases per 100,000 population in Rochester, Minnesota (1975-1978) [10] and at 160 cases per 100,000 population in Manitoba, Canada (1992), [23] with the highest incidence rate among residents aged 20-24 years.
Figures from five Blue Cross/Blue Shield Health Plans projected an incidence of 105 cases per 100,000 population (2004). [24] They estimated 340,000 cases nationwide in 2004, with an economic burden of more than $220 million. [24]
These figures differed from those indicated by data collected from STD clinics and private practitioners’ offices. Using data from these sources, the US Centers for Disease Control and Prevention (CDC) suggested much higher figures: an estimated incidence of more than 6 million new patients a year in the United States (2008) and an estimated prevalence of more than 20 million. [25, 26, 27, 28, 29] By comparison, the CDC estimated that 1.6 million people have genital herpes and 1.6 million have chlamydia or gonorrhea.
According to the “National Disease and Therapeutic Index: United States, 1966–2010,” the initial visits to physicians’ offices for STDs peaked at 351,000 visits in 1987, decreased over the following 10 years, then increased again, reaching 422,000 visits in 2006 before dropping to 357,000 in 2010.
Condylomata acuminata are clinically apparent in 1% of the sexually active population. Molecular studies indicate that 10-20% of men and women aged 15-49 years have been exposed to HPV. The prevalence of HPV is higher in certain populations, with a prevalence of 4-13% reported by STD clinics.
Several investigators report an increased prevalence of anogenital HPV infections during pregnancy. The prevalence of condyloma increases from the first to third trimester and then decreases significantly postpartum. The risk for condyloma acuminatum in pregnancy is twofold. Vulvar condylomata rarely can become large enough to obstruct labor. Cesarean delivery decreases, but does not completely prevent, HPV transmission, with the development of laryngeal papillomas in the infant. [30, 31, 32, 33]
HPV infection causes virtually all cases of cervical cancer. [34, 35] In cervical neoplasias, the HPV genome can be detected in more than 95% of tumors. No deaths due to cervical cancer have been documented in women younger than 20 years. The United States National Cancer Institute publishes data on the prevalence of worldwide cervical cancer via their online database.
The incidence of cervical cancer has decreased dramatically during the last century due to the implementation of the Papanicolaou test (Pap Test or Pap smear), beginning in the 1930s and 1940s. However, between 1990 and 2001, the annual number of estimated new invasive cervical cancers remained relatively constant (13,500 and 12,900, respectively). In the United States, 2.5 million women are estimated to have an annual cytologic diagnosis of a low-grade cervical cancer precursor.
The percentages of other cancers caused by oncogenic HPV are as follows [35] :
-
Anal cancer: 90%
-
Vulvar cancer: 40%
-
Vaginal cancer: 40%
-
Oropharyngeal cancer: 12%
-
Oral cancer: 3%
International Statistics
Globally, HPV infection is the most common STD. [36, 37] Genital warts have affected as many as 30 million individuals worldwide. A study in Finland in the mid-1980s found that the annual incidence of cytologic cervical HPV infection was 7%. [38] A study of Finnish males determined that 6.5% had evidence of HPV in exfoliative cells obtained from the urethra and genital epithelium. [39]
In many less-developed countries, cervical cancer is the most common cancer among women due to the lack of effective screening programs that monitor cervical cytology by Pap smear. [40] However, a single round of HPV screening has been demonstrated to be far superior to conventional cytology in reducing the incidence of cervical cancer morbidity and mortality. [41]
The prevalence of high-risk HPV in women with normal cervical cytology varies among different regions of the world. Although the global HPV prevalence is estimated to be approximately 12%, higher prevalences are noted in sub-Saharan Africa (24%), eastern Europe (21.4%), and Latin America (16.1%). [42]
In many developing nations, cervical cancer is the leading cause of cancer mortality among women. Worldwide, it is the second most common cause of cancer mortality among women. The World Health Organization (WHO) estimates that 570,000 new cases of cervical cancer occurred globally in 2018, and approximately 311,000 women died of cervical cancer during the same year. [43]
Age-related Demographics
People of any age may develop common warts. HPV infects more than 50% of sexually active adults. Genital infection generally occurs during the sexually active period in a person’s life, and infections increase with the number of sexual partners.
The prevalence of anogenital mucosal HPV infections is highest among college-aged women and men. The prevalence of HPV infection stratified by age in US females is as follows [44] :
-
Age 14-59 years: 26.8%
-
Age 14-19 years: 24.5%
-
Age 20-24 years: 44.8%
-
Age 25-29 years: 27.4%
-
Age 30-39 years: 27.5%
-
Age 40-49 years: 25.2%
-
Age 50-59 years: 19.6%
Thus, the highest rates of genital HPV infection are in young, sexually active females. This incidence is independent of the number of lifetime sexual partners. Most of these infections (90%) are transient. [45, 46, 47] An estimated 5.6% of sexually active adults in the United States aged 18-59 years have been diagnosed with genital warts by a medical provider. [48]
A cytologic screening of the cervix in more than 400,000 women supported a higher incidence of HPV in young women. This study found that the rate of HPV infection in women younger than 30 years is double that in women older than 30 years. [49]
The reason for the higher prevalence in younger women is not completely understood. Some investigators hypothesize that older women have fewer sexual partners and, consequently, less exposure to HPV. An alternative theory is that by age 30 years, women have acquired immunity to HPV. [50]
The presence of genital condyloma in the pediatric population presents a diagnostic and therapeutic challenge. [51] Vertical transmission of HPV can occur via in utero exposure to amniotic fluid or transmission of HPV from the maternal genital tract.
An incubation period of several months usually is required between virus infection at delivery and clinical manifestations in the infant. The average latency period is 3 months, but periods as long as 20 months have been reported. [52] Cases of childhood condylomata outside a reasonable incubation period after vertical transmission should arouse suspicion of child abuse. Treatment of condyloma in the infant includes excision under general anesthesia or the use of podophyllin. [53]
Nongenital cutaneous warts are more common among teenagers and adults who work as meat, poultry, and fish handlers. The incidence approaches 10% in child and young adult populations. However, nongenital cutaneous warts rarely occur in people younger than 5 years and usually regress within 2 years.
Epidermodysplasia verruciformis (EV) develops at an average age of onset of 6 years. Beginning in the fourth decade of life, the lesions can undergo malignant transformation into invasive squamous cell carcinoma (SCC).
Sex-related Demographics
HPV prevalence:
-
Women: 22-35%
-
Men: 2-35% (varies with sexual practices)
-
Female-to-male ratio: 1.4:1 according to a well-defined population study [10]
-
CDC Reports: Indicate higher prevalence in females compared with males
Condyloma acuminatum (genital warts):
Prevalence in STD Clinic Study [25] was as follows:
-
Men: 13%
-
Women: 9%
-
HPV infections in US college students: More frequently reported in females than males [54]
-
Detection bias: Higher incidence in females that may be due to cervical cancer screenings detecting HPV through cytologic smears
-
Medical care seeking: Females more frequently seek medical care for genital warts compared to males
Race-related demographics
HPV infection rates
-
African Americans vs Whites: African Americans have a 1.5 times higher rate of HPV infection than Whites.
-
Genital warts prevalence: Higher in non-Hispanic Whites compared to other racial or ethnic groups [48]
HPV infection by race among women [44]
-
Non-Hispanic Blacks: 39%
-
Non-Hispanic Whites and Mexican Americans: 24%
Cervical cancer death rate (1987-1991)
-
Black women vs White women: Age-adjusted death rate ratio of 6:1, higher in Black women according to the US National Cancer Institute [44]
Prognosis
HPV infection primarily involves the basal epithelial cells, leading to common recurrences and regressions. The prognosis generally is good, and most cases of genital warts are treatable. However, patients who do not develop immunity to HPV may face potentially serious sequelae.
Genital warts can spontaneously regress, remain unchanged, or increase in size. Treating these lesions does not impact the development of cervical cancer. Approximately two-thirds of patients with nongenital cutaneous warts experience spontaneous regression within 2 years, although new warts may appear.
HPV infection of the vulva can result in vulvar intraepithelial neoplasia (dysplasia) or squamous cell carcinoma of the vulva. Most research indicates a strong association between HPV infection and the development of cervical dysplasia and cervical carcinoma. HPV accounts for more than 99% of the attributable risk for cervical dysplasia. [55] Vaginal dysplasia and vaginal cancer also are linked to HPV exposure.
Histologic evidence of HPV infection on a cervical Pap smear resembles mild dysplasia. This subclinical disease often regresses spontaneously.
There is a direct correlation between anogenital HPV infection and measures of sexual activity, such as the age of first intercourse and the lifetime number of sexual partners. Women with a history of high-grade squamous intraepithelial lesion (HGSIL) of the cervix or invasive squamous cell carcinoma (SCC) of the cervix are at increased risk of developing invasive cancer in other anogenital mucosal tissues, particularly vaginal and anal carcinoma. In these patients, the relative risk for vaginal carcinoma is 5.6, and the risk of anal carcinoma is 4.
Women who are immunocompromised due to immunosuppressive drug therapy or HIV infection are at higher risk for persistent HPV disease. These women are more likely to develop dysplasia or cancer of the vulva, vagina, or cervix.
Anal cancer is strongly associated with male homosexuality and specific male practices, such as engaging in receptive anal intercourse. The relative risk is 33. However, the overall disease prevalence is higher in women than in men, with a female-to-male ratio of 1.5:1.
Men infected with HPV are at risk for genital warts. The 24-month risk varies from 57.9% in men infected with HPV type 6 or type 11 to 2% in men infected with other HPV types. [56]
Immunosuppressed patients, particularly those with cutaneous malignant lesions, have a much higher incidence of EV-HPV infection than the general population. These lesions can undergo malignant transformation. About 10% of patients with EV originate from consanguineous marriages, suggesting an autosomal recessive mode of inheritance (see Epidermodysplasia Verruciformis).
Most patients with EV experience disease progression in the third or fourth decades of life. Malignant transformation usually arises from actinic keratoses, especially in patients exposed to irradiation. Patients who avoid x-rays and sun exposure generally maintain satisfactory health.
As many as 20% of patients with genital warts have other sexually transmitted diseases concurrently. [24] In an Australian sexual health clinic, 5% of patients with genital warts also were found to have chlamydia and/or gonorrhea. [57]
Patient Education
Treating genital warts can be challenging and prolonged. Set patient expectations accordingly, counseling them on the risk of infecting others and their increased risk of having acquired other STDs. In about 60% of cases, genital warts resolve spontaneously. [1]
Educating women, particularly those who are socially and economically disadvantaged, about behaviors that reduce sexual risk has proven benefits in decreasing the incidence of STDs. Reducing STD incidence potentially could decrease HPV transmission and, consequently, cervical carcinoma incidence.
Inform patients that genital HPV is an STD, and the only way to prevent infection is to avoid direct contact with the virus, which is transmitted through skin-to-skin contact. Advise them to use condoms during vaginal, anal, or oral sex, as the virus may be present in semen even without visible warts. Emphasize that latex condoms offer some, but not complete, protection from transmission.
Evaluating the sexual partners of patients with genital warts is beneficial. Studies have documented that 30% of female partners and 80% of male partners have HPV infection, often with the same type of HPV, typically types 6, 11, 16, and 18. If a sexual partner has visible genital warts, sexual contact should be avoided until treatment is completed.
-
Human papillomavirus (HPV). Condyloma acuminatum in a patient with a history of an allograft renal transplant.
-
Human papillomavirus (HPV). Note the extensive labial involvement.
-
Human papillomavirus (HPV). Anal condyloma acuminatum.
-
Human papillomavirus (HPV). These condylomata extend to the anal verge.
-
Verrucous warts in patient with HIV infection.
-
Plantar warts.
-
Flat wart.
-
"Cauliflower" condyloma of penis.
-
Small papilloma on shaft of penis.
-
Human papillomavirus (HPV). Verruca vulgaris on the lateral border of the tongue exhibits the multiple, sharp-tipped, white, verrucous appearance, which is classic for this lesion in the oral cavity. Not all verrucae are so clinically diagnostic. Courtesy of Rose Yin Geist, DDS.
-
This is a verruca vulgaris of the anterior maxillary gingiva in a healthy young male. He had recently resolved a wart on his finger.
-
These small papillomas on the lateral tongue of a young woman showed histologic evidence of HPV in the form of extensive koilocytosis.
-
Human papillomavirus (HPV) lesion on the lingual frenum. Some patients with condyloma acuminatum present with multiple oral lesions. Courtesy of A.K. ElGeneidy, DDS.
-
Human papillomavirus (HPV). Condylomata on the lower lip, as well as other sites at the initial presentation. This presentation is unusually extensive. Multiple condylomata may be synchronous or metachronous. This patient did not present with genital condylomata. Courtesy of A.K. ElGeneidy, DDS.
-
Human papillomavirus (HPV). Heck disease in the buccal mucosa of a 7-year-old boy. Courtesy of Sheldon Mintz, DDS.
-
Human papillomavirus (HPV). Verrucae and papillomas appear as frondlike epithelial proliferations. Verrucae tend to be more keratinized with sharper projections than papillomas.
-
Human papillomavirus (HPV). Condyloma acuminatum generally has a papillary architecture and may microscopically resemble verruca vulgaris and papilloma (hematoxylin and eosin stain, original magnification X10). Courtesy of AK ElGeneidy, DDS.
-
Human papillomavirus (HPV). Koilocytes in the upper epithelium are a helpful, although not completely reliable, indication that a lesion is associated with human papillomavirus. Koilocytes display a dark small nucleus with clear cytoplasm (hematoxylin and eosin stain, original magnification X100). Courtesy of Sheldon Mintz, DDS.
-
Human papillomavirus (HPV). Condyloma acuminatum may show brisk mitotic activity, although oral condyloma acuminatum is not considered a premalignant lesion (hematoxylin and eosin stain, original magnification X40). Courtesy of A.K. ElGeneidy, DDS.
-
The left panel is transudation of serum antibodies to the site of human papillomavirus infection, and the right panel is exudation of serum antibodies to the site of human papillomavirus infection.
-
The figure shows proposed mechanisms used by the human papillomavirus vaccine to neutralize antibodies and protect against infection.
-
Figure showing how human papillomavirus penetrates the basal layer and eventually is released at the surface.
Tables
Nongenital Cutaneous Disease |
HPV Type |
Common warts (verrucae vulgaris) |
1, 2, 4, ,27,132,133,148,149,179,183 |
Plantar warts (myrmecias) |
1, 2, 4, 26,27,28,29,41,57,63,65,77,117,125,128,129,130,131 |
Flat warts (verrucae planae) |
3, 10, 27, 28, 38, 41, 49, 75, 76, 126 |
Butcher’s warts (common warts of people who handle meat, poultry, and fish) |
1-4, 7, 10, 28 |
Mosaic warts |
2, 27, 57 |
Ungual squamous cell carcinoma |
16 |
Epidermodysplasia verruciformis (benign) |
2, 3, 10, 12, 15, 19, 36, 46, 47, 50 |
Epidermodysplasia verruciformis (malignant or benign) |
5, 8-10, 14, 17, 20-25, 37, 38 |
Nonwarty skin lesions |
37, 38 |
Nongenital Mucosal Disease |
HPV Type |
6, 11 |
|
6, 11, 16, 18 |
|
Laryngeal papilloma (recurrent respiratory papillomatosis) [16] |
2, 6, 11, 16, 30, 40, 57 |
6, 11 |
|
Maxillary sinus papilloma |
57 |
Squamous cell carcinoma of the sinuses |
16, 18 |
Conjunctival papillomas |
6, 11,16 |
Conjunctival carcinoma |
16 |
Oral focal epithelial hyperplasia (Heck disease) |
13, 32 |
16, 18 |
|
16, 18 |
|
16, 18 |
|
Anogenital Disease |
HPV Type |
6,11,16,18,26,31,33,35,40,42,43,44,45,51,52,53,54,55,56,58,59,66,68,70,153,175,178,180,200,201,202 |
|
16, 18, 34, 39, 40, 42, 45 |
|
16, 18, 31, 34 |
|
Giant condylomata (Buschke-Löwenstein tumors) |
6, 11, 57, 72, 73 |
Unspecified intraepithelial neoplasia |
30, 34, 39, 40, 53, 57, 59, 61, 62, 64, 66-69 |
Low-grade squamous intraepithelial lesions (LGSIL) |
6, 11, 16, 18, 31,33,35,42,43,44,45,51,52,54,61,70,72,74 |
High-grade squamous intraepithelial lesions (HGSIL) |
6, 11, 16, 18, 31, 33, 43,35,39,42,44,45,51,52,56,58,66,67 |
6, 11, 16, 18 |
|
Carcinoma of vagina |
16 |
16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68, 70, 73, 82 |
|
Carcinoma of anus |
16, 31, 32, 33 |
Carcinoma in situ of penis (erythroplasia of Queyrat) |
16 |
16, 18 |
| Disease | HPV 9-valent |
|---|---|
| Cervical cancer, vulvar cancer, vaginal cancer, anal cancer | HPV types 16, 18, 31, 33, 45, 52, and 58 |
| Genital warts (condyloma acuminata) | HPV types 6 and 11 |
| Cervical intraepithelial neoplasia (CIN) grade 1-3 and cervical adenocarcinoma in situ (AIS) | HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58 |
| Vulvar intraepithelial neoplasia (VIN) or vaginal intraepithelial neoplasia (VaIN) grades 2 and 3 | HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58 |
| Anal intraepithelial neoplasia (AIN) grades 1-3 | HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58 |
| Disease | HPV 9-valent |
|---|---|
| Anal cancer | HPV types 16, 18, 31, 33, 45, 52, and 58 |
| Genital warts (condyloma acuminata) | HPV types 6 and 11 |
| Anal intraepithelial neoplasia (AIN) grades 1, 2, and 3 | HPV types 16, 18, 31, 33, 45, 52, and 58 |

What would you like to print?
- Overview
- Presentation
- DDx
- Workup
- Treatment
- Guidelines
- Guidelines Summary
- Guidelines on Human Papillomavirus Screening by the US Preventive Services Task Force (USPSTF)
- 2020 Updated cervical cancer screening for individuals at average risk by the American Cancer Society (ACS)
- 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors by ASCCP
- Guidelines on Human Papillomavirus Vaccination by the American Cancer Society
- Guidelines on Human Papillomavirus Vaccination by the Advisory Committee on Immunization Practices (ACIP)
- Show All
- Medication
- Media Gallery
- Tables
- References