Practice Essentials
In venous insufficiency states, venous blood escapes from its normal antegrade path of flow and refluxes backward down the veins into an already congested leg. Venous insufficiency syndromes are most commonly caused by valvular incompetence in the low-pressure superficial venous system (see the image below) but may also be caused by valvular incompetence in the high-pressure deep venous system (or, rarely, both). In addition, they may result from the congenital absence of venous valves.

Untreated venous insufficiency in the deep or superficial system causes a progressive syndrome (chronic venous insufficiency [CVI]). Historically, CVI was known as postphlebitic syndrome and postthrombotic syndrome, terms referring to the conditions that cause most cases. However, these terms have been largely abandoned because they do not include another common cause of the disease, the congenital absence of venous valves.
In addition to poor cosmesis, CVI can lead to chronic life-threatening infections of the lower extremities. Pain, especially after ambulation, is a hallmark of the disease. CVI causes characteristic changes, called lipodermatosclerosis, to the skin of the lower extremities, which lead to eventual skin ulceration. [1]
Venous insufficiency is neither uncommon nor benign. Treatment is aimed at ameliorating the symptoms and, whenever possible, at correcting the underlying abnormality. Graduated compression is the cornerstone of modern therapy. Deep system disease is often refractory to treatment, but superficial system disease can usually be treated by ablating the refluxing vessels. Refluxing superficial vessels can safely be removed or ablated without sequelae.
Over 2 million individuals have advanced chronic venous disease, from which around 20% percent present with venous ulcers as a complication, resulting in a reduction in the quality of life, exposure to financial constraints, and disability for patients. [2] The estimated annual expenditures dedicated to the management of venous ulcer disease exceeds $2.5 billion; [3] hence, it is important to reduce the risk factors and increase the therapeutic options that could prevent disease and disability from complications.
See Superficial Venous Insufficiency: Varicose Veins and Venous Ulcers, a Critical Images slideshow, to help identify the common risk factors and features of this condition and its management options.
Anatomy
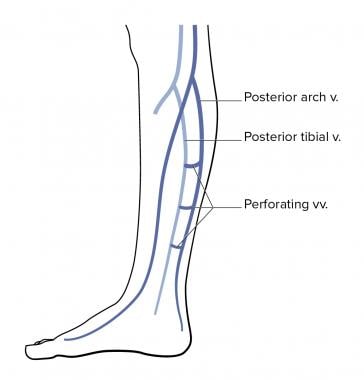
The venous network in the lower extremities commonly affected by CVI is divided into the following three systems (see the images below):
-
Superficial veins (including the great saphenous vein [GSV], the small saphenous vein [SSV], and their tributaries)
-
Deep veins (including the anterior tibial, posterior tibial, peroneal, popliteal, deep femoral, superficial femoral, and iliac veins)
-
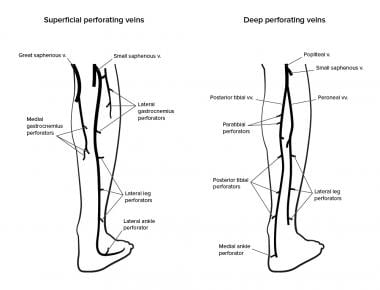
Perforating or communicating veins
When the venous network is functioning correctly, every movement of the leg causes blood to be pumped inward and upward past a series of valves (see the image below). During ambulation, the normal pressure in the venous system of the lower leg is nearly zero. Immediately after ambulation, the early standing pressure in the normal leg remains low. Arterial inflow fills the leg veins slowly, and the only source of venous pressure is the hydrostatic pressure of a column of blood as high as the nearest competent valve.
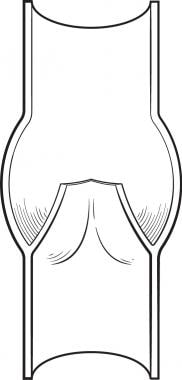 Venous valve. Thrombosis can begin as blood flow becomes turbulent, permitting platelets to remain in valve sinus. This forms nidus of thrombus.
Venous valve. Thrombosis can begin as blood flow becomes turbulent, permitting platelets to remain in valve sinus. This forms nidus of thrombus.
In venous insufficiency, after prolonged standing, the veins are completely filled, and all the venous valves float open. At this time, high hydrostatic venous pressure results from the unbroken column of fluid that extends from the head to the foot. Failed valves cause the column of standing blood in the vein to remain high even during ambulation. The hydrostatic pressure increases during and immediately after ambulation, which cause venous congestion.
Pathophysiology
Various mechanisms are associated with failure of superficial venous valves. Most commonly, congenitally weak vein walls dilate under normal pressures to cause secondary valve failure. Direct injury or superficial phlebitis may cause primary valve failure. Congenitally abnormal valves can also be incompetent at normal superficial venous pressures. Normal veins and normal valves may become excessively distensible under the influence of hormones (as in pregnancy).
High venous pressure is directly responsible for many aspects of venous insufficiency syndrome. Under normal conditions, two major mechanisms in the body operate to prevent venous hypertension. First, bicuspid valves in the veins prevent backflow and venous pooling. Deep venous thrombosis (DVT) commonly occurs at these valves, causing irreversible damage to the valve.
Second, during normal ambulation, calf muscles decrease venous pressures by approximately 70% in the lower extremities (see the image below). With rest, pressures return to normal in approximately 30 seconds. In diseased veins, ambulation decreases venous pressures by only 20%. When ambulation is stopped, pressure in the vein lumen increases slowly, returning to normal over a period of minutes.
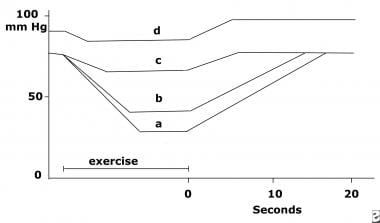 Hemodynamic charting of (a) healthy patients, (b) patients with only varicose veins, (c) patients with incompetent perforator veins, and (d) patients with deep and perforator incompetence.
Hemodynamic charting of (a) healthy patients, (b) patients with only varicose veins, (c) patients with incompetent perforator veins, and (d) patients with deep and perforator incompetence.
Venous hypertension in diseased veins is thought to cause CVI through the following sequence of events [4] :
-
Increased venous pressure transcends the venules to the capillaries, impeding flow
-
Low-flow states within the capillaries cause leukocyte trapping
-
Trapped leukocytes release proteolytic enzymes and oxygen free radicals, which damage capillary basement membranes
-
Plasma proteins (eg, fibrinogen) leak into the surrounding tissues, forming a fibrin cuff
-
Interstitial fibrin and resultant edema decrease oxygen delivery to the tissues, resulting in local hypoxia
-
Inflammation and tissue loss result
Most cases of superficial vein valve failure occur after primary points of high-pressure leakage develop between the deep system and the superficial system. High pressure leads to secondary valve failure when otherwise normal superficial veins become so widely dilated that the thin flaps of the venous valves can no longer make contact in the lumen of the vessel. Over time, these incompetent superficial veins become visibly dilated and tortuous, at which point they are recognized as varicose veins.
High pressure can enter the superficial veins as a result of the failure of key valves at any point of communication between the deep system and the superficial system. High-pressure leakage from the deep veins to the superficial system has 2 major sources, as follows:
-
Junctional valve failure
-
Perforator valve failure
Junctional high-pressure disease most often results from failure of the primary valve at the junction between the GSV and the common femoral vein at the groin (saphenofemoral junction). Vein incompetence then proceeds distally from the groin, and patients perceive that a large vein is growing down their leg. A less common form of junctional reflux results from failure of the primary valve at the junction between the SSV and the popliteal vein at the knee (saphenopopliteal junction).
Perforator high-pressure disease results from failure of the valves of any perforating vein. The most common sites of primary perforator valve failure are in the midproximal thigh (Hunterian perforator) and in the proximal calf (Boyd perforators). When the primary high-pressure entry point is distal, large clusters of veins are first noticed in the lower leg, with large veins eventually growing up the leg toward the groin.
Not all of the sequelae of venous insufficiency are related to venous hypertension, and not all patients with venous hypertension develop ulceration. Some patients with venous ulceration do not have marked venous hypertension.
Poor clearance of lactate, carbon dioxide, and other products of cellular respiration also contributes to the development of the syndrome. A defect in the clearance of extraneous substances can be quantified: If albumin labeled with a radioactive tracer is injected into the foot tissues, the clearance rate is markedly slowed by deep venous obstruction or by deep or superficial venous incompetence.
Although this effect is referred to as venous stasis, the reduced clearance of cellular metabolites is not always due to true venous stasis. In many cases, the venous blood is moving at a normal speed, but a local recirculation of this venous blood upward through normal veins and downward through varicosities prolongs the average time required for the blood to pass from the heart and lungs through the legs and back to the central circulation.
The time required for an aliquot of radiolabeled blood to pass from the femoral artery through the leg and back to the central circulation is highly correlated with the development of leg ulcers. The aliquot transit time and the clearance time for an extremity are closely related to the volume of retrograde flow through refluxing veins. Superficial varicosities always produce venous recirculation and can result in prolonged clearance that may be localized or affect the whole leg.
Experimental evidence shows that if the peak retrograde flows in the GSV, SSV, and popliteal vein add up to less than 10 mL/s, progressive visible stasis dermatitis and ulceration do not occur. If they add up to more than 15 mL/s, the incidence of ulceration is high. In some cases, purely superficial local reflux with a pressure of more than 7 mL/s can cause local ulceration.
In the San Diego Population Study, levels of circulating P-selectin were found to be correlated with the severity of CVI, though not with the incidence of CVI in general. [5] The study findings suggest that the pathogenesis of CVI may include activation of platelets and endothelial cells.
Etiology
CVI can be caused by congenital absence of or damage to venous valves in the superficial and communicating systems. It can also be caused by venous incompetence due to thrombus formation as favored by the Virchow triad (venous stasis, hypercoagulability, and endothelial trauma [6] ). Varicose veins rarely are associated with the development of CVI. Most cases of venous insufficiency are related to reflux through the superficial veins.
Chronic nonhealing wounds of the lower extremity have many different potential causes, but most chronic lower-extremity ulcers are of venous etiology. The majority of venous ulcers are caused by venous reflux that is purely or largely confined to the superficial venous system; only a minority are caused by chronic DVT or by valvular insufficiency in the deep veins.
Superficial venous insufficiency
In superficial venous insufficiency, the deep veins are normal, but venous blood escapes from a normal deep system and flows backwards through dilated superficial veins in which the valves have failed. More than 80% of varicose veins seen on the leg are caused by venous insufficiency or a leaky valve in the GSV, which terminates near the inguinal ligament as it joins the common femoral vein.
The initial valve failure may occur at any level between the groin and the ankle, but the saphenofemoral junction is the high point of reflux in most patients with severe superficial venous insufficiency. Valve failure can be spontaneous in patients with congenitally weak valves. Congenitally normal valves can fail as a consequence of direct trauma, thrombosis, hormonal changes, or chronic environmental insult (eg, prolonged standing).
Deep venous insufficiency
Deep venous insufficiency can be due to congenital valve or vessel abnormalities, but it most commonly occurs when the valves of the deep veins are damaged as a result of DVT. With no valves to prevent deep system reflux, the hydrostatic venous pressure in the lower extremity increases dramatically.
Klippel-Trénaunay-Weber syndrome
A less common cause of venous insufficiency is Klippel-Trénaunay-Weber (KTW) syndrome, which involves port-wine stains, varicose veins, and bony or soft-tissue hypertrophy. Patients with pure Klippel-Trénaunay syndrome have only venous involvement, whereas those with the Parkes Weber variant also have arteriovenous malformations.
The capillary hemangiomas (port-wine stains) of KTW syndrome, like those of other forms of venous insufficiency, can lead to local skin breakdown and ulceration, bleeding, and secondary infection. This can occur in any organ system of the body.
The sciatic vein is a large superficial vessel that is present during fetal development but usually does not persist. In patients with KTW syndrome, this vein may be noticed at birth, or it may become apparent later in life. The vein extends along the posterolateral aspect of the leg from the foot to the gluteal region. When present, it is invariably a reflux pathway rather than a pathway for antegrade flow.
Patients with KTW syndrome may have atresia of the deep veins, as well as many abnormal venous pathways involving the deep and superficial venous systems. KTW syndrome can produce such severe venous insufficiency that the otherwise normal lymphatic system becomes overwhelmed by the amount of lymph production, which leads to secondary lymphedema.
Surgical attempts to treat the abnormal refluxing veins in KTW syndrome are fraught with peril because postoperative worsening of venous abnormalities is common.
Risk factors
The incidence of CVI rises substantially with age. A history of DVT, which renders venous valves incompetent and thereby causes backflow and increased venous pressure, is a risk factor.
A sedentary lifestyle minimizes the pump action of calf muscles on venous return, causing higher venous pressure. CVI occurs more frequently in women who are obese. Vocations that involve standing for long periods predispose individuals to increased venous pressure in dependent lower extremities. A higher incidence of CVI is observed in men who smoke. Pregnancy is an important causative factor in the development of peripheral venous insufficiency. Contraceptive medication use, hypertension, previous leg injuries, and low intake of cellulose fibbers have also been considered. [7]
Epidemiology
United States statistics
Venous insufficiency is a significant public health problem in the United States with over 11 million males and 22 million females 40 years old or older having varicose veins, and over 2 million adults having advanced chronic venous disease. [3] It has been estimated that 2-5% of all Americans have some changes associated with CVI. Published estimates of the prevalence of varicosities range from 7% to 60% in the adult population, with most studies demonstrating clinical varicose reflux in about 40% of the population. [8] Venous stasis ulcers affect approximately 500,000 people. The mean incidence of hospital admission for CVI is 92 per 100,000 admissions.
International statistics
The frequency of venous insufficiency is believed to be higher in Westernized and industrialized nations than in developing nations, most likely because of differences in lifestyle and activity.
It has been estimated that approximately 1-2% of the adult population presents with lower-limb ulceration, from which 70-90% of these ulcers are attributed to CVI. [7, 9]
Age-related demographics
The prevalence of venous insufficiency increases with age. Peak incidence occurs in women aged 40-49 years and in men aged 70-79 years.
Reticular veins usually appear or are first noticed in adolescence and young adulthood, with only a small number of new cases developing after the childbearing years. Truncal varicosities and telangiectatic webs, on the other hand, are relatively less common in youth and can appear throughout life.
The Bochum study, which assessed a large number of children aged 10-12 years at one point (Bochum I) and again 4 years later (Bochum II), revealed that symptoms and abnormal venous test results occur before any abnormal veins are visible at the surface. Abnormal reticular veins appear first and are followed by incompetent perforatoring veins and truncal varicosities, which appear several years later. [10]
Although active venous ulceration affects less than 1% of the population, its prevalence slightly increases to 3% in individuals older than 65 years. [11]
Sex-related demographics
The incidence and prevalence of deep and superficial venous disease depend on the age and sex of the population, but at any age, such disease is more common in women than in men. In younger men, the incidence is lower than 10%, compared with 30% in similarly aged women. In men older than 50 years, the incidence is 20%, compared with 50% in similarly aged women. [12]
Prognosis
The syndromes of venous hypertension and reduced venous clearance are important causes of morbidity and disability in patients with varicose venous disease (see also Complications).
Without correction of the underlying cause, venous insufficiency is inexorably progressive. Subjective symptoms usually worsen over time.
In many patients, the skin eventually breaks down and nonhealing ulcers develop. A study by Abbade et al determined that longstanding and large ulcers and recurrences are the primary complications encountered by patients who have venous ulcers. [13] Risk factors for these complications include severe lipodermatosclerosis, a previous history of ulcers, and time since first ulcer episode of 2 years or longer.
Chronic nonhealing leg ulceration can be debilitating. Approximately 1 million Americans have an ulceration due to superficial venous disease, and approximately 100,000 are disabled because of their condition. Reflux need not be entirely eliminated for the ulceration to resolve. Ulcers will heal if the net volume and pressure of reflux are reduced below a threshold level. Tissue atrophy and staining are usually not reversible.
Patients have an increased lifetime risk of DVT and pulmonary embolism. Tsai et al, examining the National Inpatient Sample from 1988-2000, found that DVT affected 1.3% of patients and that amputation was necessary in 1.2%, with an overall mortality of 1.6%. [14]
As many as 50% of patients with untreated varicose veins develop superficial thrombophlebitis at some time. This is of grave concern, because unrecognized DVT is present in as many as 45% of patients with what appears to be purely superficial phlebitis. The risk of DVT is 3 times higher in patients with superficial varicosities than in the general population.
Bed rest and intercurrent illness place patients with venous insufficiency at higher risk for DVT. Phlebitis develops in 60% of hospitalized patients with clinically evident superficial venous insufficiency, and in nearly one half of cases, the condition progresses to DVT. Approximately one half of patients with DVT have detectable pulmonary embolism, and the death rate in this group exceeds 1 in 3.
Venous insufficiency syndromes can also lead to death from hemorrhage. Bleeding from lower-extremity varicosities can be fatal [15] ; 23 such fatalities were reported in England and Wales in 1973, [16] and, although there is no central registry to tabulate the frequency with which it occurs, such cases are not unusual in the United States. Bleeding is not a rare problem, but it is often managed incorrectly.
Outcomes for different therapies have varied. Clot lysis (eg, with tissue plasminogen activator or urokinase) and thrombectomy have been tried but have largely been abandoned because of the extremely high recurrence rates.
Saphenous vein crossover grafting for iliofemoral disease has a relatively high failure rate (20%), and thus, ringed polytetrafluoroethylene (PTFE) grafts are now being used. Long-term patency rates have not been determined. The Husni bypass for superficial femoral vein occlusion has an even higher failure rate (approximately 40%) and thus is now performed infrequently.
Surgery for CVI resulting from deep vein incompetence includes valvuloplasty and allograft or cadaveric vein transplant. Valvuloplasty for patients with congenital absence of functional valves, when combined with ligation of perforating veins, yields a superior outcome in 80% of cases after 5 years. Allograft or cadaveric vein transplants are undergoing further evaluation, with long-term results pending.
Patient Education
Patients with venous insufficiency syndromes should be instructed to wear compression stockings as much as they can, unless they also have arterial insufficiency or unless they cannot tolerate the stockings for some other reason.
Patients should also be instructed to avoid prolonged standing or sitting and to perform walking or calf-muscle exercises at regular intervals.
For patient education resources, see Blood Clot in the Legs, Varicose Veins, and Phlebitis.
-
Superficial venous insufficiency with skin changes.
-
Ulcer due to venous insufficiency.
-
Venous valve. Thrombosis can begin as blood flow becomes turbulent, permitting platelets to remain in valve sinus. This forms nidus of thrombus.
-
Hemodynamic charting of (a) healthy patients, (b) patients with only varicose veins, (c) patients with incompetent perforator veins, and (d) patients with deep and perforator incompetence.
-
Perforator vein bulging into subcutaneous tissue.
-
Chronic venous stasis ulcer.
-
Venous stasis ulcer and surrounding dystrophic tissue.
-
Venous insufficiency iliofemoral obstruction (Palma operation). Saphenous vein from contralateral leg tunneled subcutaneously to femoral vein of affected limb; cumulative patency of 75% at 5 years. Procedure relieves venous claudication but may not heal ulcers or relieve swelling.
-
Lower-leg venous anatomy.
-
Perforating veins of lower leg.
-
Venogram demonstrating incompetent perforating veins.
Tables

What would you like to print?
- New Evidence Supports DOACs in Cerebral Venous Thrombosis
- Cerebral Venous Thrombosis Linked to Increased Cancer Risk
- Cancer Surgery Tied to Increased Venous Thromboembolism Risk
-
 Jun 20, 2025 This Week in Cardiology Podcast
Jun 20, 2025 This Week in Cardiology Podcast
-
How Do CDK4/6 Inhibitors Affect HR+/HER2- Advanced Breast Cancer Outcomes in Real-World Clinical Practice?
-
Superficial Venous Thrombosis for Primary Care Physicians







