Background
Tungiasis is an infestation by the burrowing flea Tunga penetrans or related species. [1] The flea has many common names, being known in various locations as the chigger flea, sand flea, chigoe, jigger, nigua, pigue, or le bicho de pe (see the image below). Painful infections with T penetrans can cause significant morbidity. (See Etiology.)
Tungiasis was first reported in crewmen who sailed with Christopher Columbus. The flea is indigenous to the West Indies/Caribbean/Central America region, but it has spread to Africa, India, Pakistan, and South America. Tungiasis is rarely diagnosed in North America, but it should no longer be obscure to physicians because of increasing international travel to tropical destinations. (See Epidemiology, Clinical Presentation, and Workup.) [2]
To reproduce, the flea requires a warm-blooded host. In addition to humans, reservoir hosts include pigs, dogs, cats, cattle, sheep, horses, mules, rats, mice, and other wild animals (see the image below). (See Etiology.) [3, 4, 5, 6]
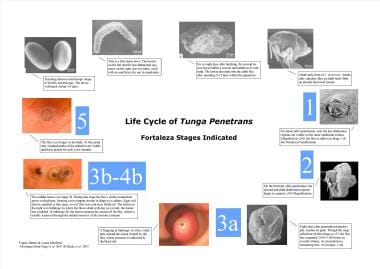 Life cycle of Tunga penetrans - Fortaleza stages included. Compiled and designed by Fausto Bustos and Lucas Manfield.
Life cycle of Tunga penetrans - Fortaleza stages included. Compiled and designed by Fausto Bustos and Lucas Manfield.
See also 7 Bug Bites You Need to Know This Summer, a Critical Images slideshow, for helpful images and information on various bug bites.
The World Health Organization has listed tungiasis as a neglected disease of marginalized populations and has encouraged more significant research of the disease. [7]
Patient Education
Risk Factors
Travelers to affected countries, as well as people native to those areas, must be advised to wear shoes (not sandals) when walking along sandy areas in affected regions and to refrain from sitting or lying in the sand.
The major risk factor for exposure to T penetrans is failure to wear shoes when walking in sand in an area with active infestation. Wearing shoes and not sitting or lying in the sand are the most important steps to reduce infection risk. If available, the repellent Zanzarin has been shown to be effective when applied to the feet once daily. [8]
Risk factors for developing tungiasis include dirt floors, open toed shoes, and unsanitary living conditions. To address these factors, cement floors and closed toed shoes should be implemented. [9] The entire sand flea life cycle can be completed inside a home without a solid floor. When the released eggs fall onto the floor, they can be transferred into crevices in the floor, which are full of organic material to sustain the larvae. Then once adults, the flea attaches as the host walks over the contaminated floor area. [10]
In Trinidad, tungiasis reaches a peak infestation rate of 54% among males aged 25-35 years. Among females, the peak occurs in those aged 55 years and older. [11] In a village in northeastern Brazil, bimodal prevalence peaks were noted in children aged 5-9 years and in adults older than age 60 years. [12] Similar trends were observed in sub-Saharan Africa. Children within the 4-15 year age group experienced the highest tungiasis prevalence of 42.9%, followed by those aged 60 and older with a prevalence of 24.7%. [9, 10]
Low educational attainment has been found to be strongly associated with tungiasis diagnosis and infection. In southern Ethiopia, children with mothers who are illiterate are at a higher risk of being infected with tungiasis. [13] Stigma towards adults and children infected with tungiasis has decreased their quality of life, often due to teasing, discrimination, and bullying. [9] Difficulty concentrating and disruptive sleep have also been associated with tungiasis infection among children. [9]
Etiology
The main habitat for T penetrans is warm, dry soil and sand of beaches, stables, and stock farms. Upon contact, the flea invades unprotected skin. The most common site of involvement is the feet (interdigital skin and subungual area). The flea has limited jumping ability, so infection occurs only on areas of skin that were directly exposed to sand or soil in which the fleas live.
Both the male and the unfertilized female flea feed intermittently on warm-blooded hosts, but only the female flea can produce the typical skin lesion of tungiasis. [14] Once impregnated, the female flea anchors herself to the skin by using biting mouthparts and burrows into the epidermis of the host near the plantar surfaces of the foot, [15] in the webbing between the toes, and around the periungual region. Because the process is painless, a keratolytic enzyme may be involved.
The flea expands, often reaching 1 cm in diameter. The head is down into the upper dermis, feeding from blood vessels, while the caudal tip of the abdomen is at the skin surface, often forming a punctum or an ulceration (see the images below). The flea breathes through this opening. In many cases, this is described as a white patch with a black dot. Very heavy infestation may cause ulceration and fibrosis that may result in secondary infections, such as bacteremia, tetanus, lymphangitis, and gas gangrene. [16]
The process of a sand flea burrowing into the host’s skin to the eventual elimination of the dead flea by the host encompasses the Fortaleza stages. The life cycle image by Bustos and Manfield further details these stages. [17]
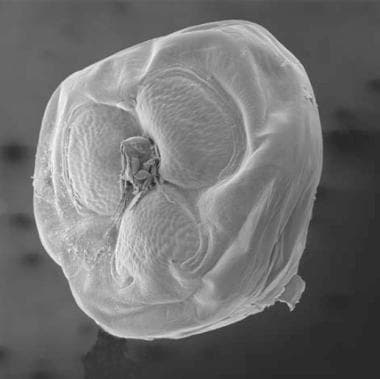
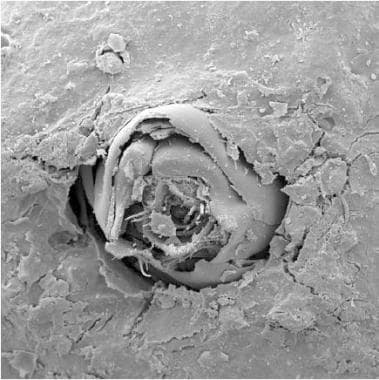 Scanning electron micrograph of flea 6 hours after beginning of penetration. The penetration is almost completed; only the last abdominal segments protrude through the skin (x240).
Scanning electron micrograph of flea 6 hours after beginning of penetration. The penetration is almost completed; only the last abdominal segments protrude through the skin (x240).
 Scanning electron micrograph of flea in stage 2. The rear end, the genital opening, and the 4 pairs of stigmata form a miniature cone, which towers above the crater caused by pushing in abdominal segments 7 and 8 (x190).
Scanning electron micrograph of flea in stage 2. The rear end, the genital opening, and the 4 pairs of stigmata form a miniature cone, which towers above the crater caused by pushing in abdominal segments 7 and 8 (x190).
 Scanning electron micrograph of flea on day 3 after penetration. The hypertrophic zone between abdominal segments 2 and 3 is gaining a bulging shape and looks like a life-belt (x100).
Scanning electron micrograph of flea on day 3 after penetration. The hypertrophic zone between abdominal segments 2 and 3 is gaining a bulging shape and looks like a life-belt (x100).
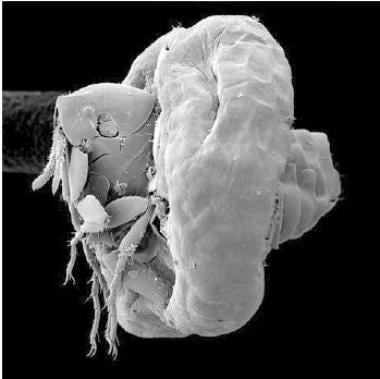
 Scanning electron micrograph of flea on day 8 after penetration. The hypertrophy zone has taken the shape of a sphere. The 3 parts of abdominal segment 2 are completely bent apart. Together with the newly developed, crescent-shaped chitinous clasps, the anterior part of the flea looks like a 3-leafed clover (x32).
Scanning electron micrograph of flea on day 8 after penetration. The hypertrophy zone has taken the shape of a sphere. The 3 parts of abdominal segment 2 are completely bent apart. Together with the newly developed, crescent-shaped chitinous clasps, the anterior part of the flea looks like a 3-leafed clover (x32).
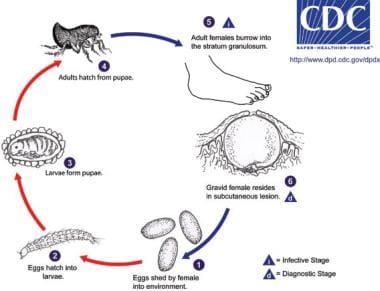
Within 2 weeks of penetration, the flea that has burrowed under the skin increases its volume by a factor of 2000. [18] Over 1-2 weeks, more than 100 eggs, which fall to the ground, are individually released from the exposed orifice. Afterward, the flea dies and is slowly sloughed by the host. The eggs hatch on the ground in 3-4 days, go through larval and pupal stages, and become adults in 2-3 weeks. The complete life cycle lasts approximately 1 month.
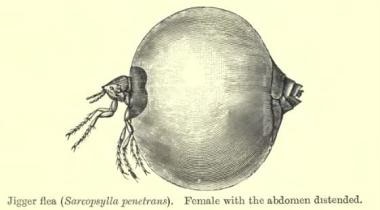 Illustration of Tunga penetrans (sand flea) in its enlarged state. Courtesy of Wikimedia Commons [https://commons.wikimedia.org/wiki/File:ChiggerBMNH.jpg].
Illustration of Tunga penetrans (sand flea) in its enlarged state. Courtesy of Wikimedia Commons [https://commons.wikimedia.org/wiki/File:ChiggerBMNH.jpg].
Epidemiology
Worldwide, tungiasis has been reported to have a prevalence of 80% in children and 60% in adults. [19]
Occurrence in the United States
The incidence of tungiasis is unknown because it is not a reportable disease. As of 2000, only 20 cases had been reported in the United States, with 15 of them being reported prior to 1989. [20, 21, 22, 23] Since 2000, sporadic cases have been reported in the United States. [24] All of these cases were imported from outside of the United States.
International occurrence
Tungiasis is potentially endemic in 88 countries worldwide. [25] Tungiasis is especially prevalent in low-resource communities. [18] Estimates on the occurrence of tungiasis rely primarily on community-based studies. Recent prevalence of tungiasis in rural and urban resource-poor communities in Brazil, Nigeria, and Madagascar was up to 60%. [26, 27, 28, 29, 30, 31, 32] Between 2003 and 2015, 96 of the 135 tungiasis cases with known geographic origin came from Brazil. Additionally, using an ecological niche model, Argentina, Bolivia, Brazil, Colombia, Ecuador, French Guyana, Guatemala, Haiti, Mexico, Paraguay, Peru, Trinidad and Tobago, and Venezuela were all identified as countries where tungiasis may or does exist. [9]
Tungiasis has reemerged to epidemic levels in many countries across sub-Saharan Africa. [33, 34, 35] 668 million individuals living in sub-Saharan African countries (62% of the total population) reside in environments suitable for sand flea proliferation. [36] Across 7 sub-Saharan African countries (Ethiopia, Cameroon, Tanzania, Kenya, Nigeria, Rwanda, and Uganda), tungiasis affected 33.4% of the pooled population. [19]
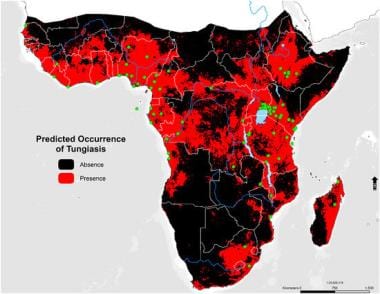 Graphical abstract of predicted tungiasis occurrence within sub-Saharan Africa. Courtesy of MDPI [Deka MA. Mapping the Geographic Distribution of Tungiasis in Sub-Saharan Africa. Tropical Medicine and Infectious Disease. 2020 Jul 24;5(3):122. Online at: https://www.mdpi.com/2414-6366/5/3/122#.].
Graphical abstract of predicted tungiasis occurrence within sub-Saharan Africa. Courtesy of MDPI [Deka MA. Mapping the Geographic Distribution of Tungiasis in Sub-Saharan Africa. Tropical Medicine and Infectious Disease. 2020 Jul 24;5(3):122. Online at: https://www.mdpi.com/2414-6366/5/3/122#.].
In April 2012, a community-based cross-sectional study was performed in 2 villages in Western Tanzania. A total of 586 individuals older than 5 years were enrolled, and 249 (42.5%) were diagnosed with tungiasis. Those aged 45 years and older had the highest prevalence of tungiasis at 71.1% and the most severe parasite load (median number of embedded fleas: 17.5; interquartile range: 15-22.5). [37]
In September 2012, an outbreak of tungiasis occurred in a group of Israeli travelers to Ethiopia. The attack rate in the group was 53%, affecting 9 patients, and most skin lesions appeared on the feet, where lesions are most commonly found. [38]
Approximately 45.2% of a Nigerian community in Lagos State was observed to be infected, with most of the cases occurring in children aged 5-14 years. [39] In a traditional fishing village in northeastern Brazil, the overall prevalence was 51%. [12, 40] In a village in rural Haiti, nearly 75% of the population was observed to have tungiasis lesions. [41] Six percent of the patients visiting a travel-associated dermatosis clinic in Paris had tungiasis. [5]
In March 2012, 12 free-ranging jaguars in the Mato Grosso do Sul state of Brazil were captured and examined for the presence of T penetrans. They found the prevalence of tungiasis to be 100% in this group of jaguars. T penetrans presence was based on observations of embedded fleas and morphological identification of free-living fleas. This study was performed during the dry season in Brazil and all of the jaguars were in good health. [42]
Studies have shown that the development of eggs from adult fleas can take place indoors and outdoors. In rural and urban communities in Brazil, tungiasis has been acquired peridomiciliary and intradomiciliary. [43] In many countries with the greatest presence of T penetrans, lack of health education, poor housing (particularly houses with dirt floors), and close proximity to animals are risk factors for tungiasis. [44, 45, 46]
Race-, sex-, and age-related demographics
No racial predisposition is apparent. Infection rates among native inhabitants of developing countries, however, are much higher than among visitors.
In endemic regions, such as Trinidad, males were found to be consistently more likely than females to have an infestation. Males also had higher chigoe flea burdens, with about twice the number of fleas detected per subject. [11]
In Trinidad, tungiasis reaches a peak infestation rate of 54% among males aged 25-35 years. Among females, the peak occurs in those aged 55 years and older. [11] In a village in northeastern Brazil, bimodal prevalence peaks were noted in children aged 5-9 years and in adults older than age 60 years. [12]
Low educational attainment has been found to be strongly associated with tungiasis diagnosis and infection. In southern Ethiopia, children with mothers who are illiterate are at a higher risk of being infected with tungiasis. [13]
Prognosis
The prognosis of tungiasis is excellent if proper sterile methods are followed for the extraction of fleas and if extraction occurs soon after infection. Uncomplicated infestation results in pain, swelling, tenderness, and some limitation in mobility (although sometimes lesions are pruritic or even asymptomatic).
To prevent superinfection, sand fleas should be surgically extracted immediately after penetration and the crater should be treated with topical antibiotic. [47] When secondary infection is already present, an oral antibiotic should be considered. [2]
Complications
Secondary infections, such as bacteremia or septicemia, lymphangitis, tetanus, and gas gangrene, can occur. Among a native population in Brazil, the most common causes of bacterial superinfection included Staphylococcus aureus and various Enterobacteriaceae; anaerobic streptococci and Clostridium species also were found. [47] Sores caused by burrowed fleas can be a potential entry point for clostridial and other infections, or these infections may follow attempts to extract the flea. Autoamputation of digits or other extensive soft tissue debridement is also a possibility.
Death from tetanus associated with tungiasis has been reported. [4] For example, a case series from Haiti demonstrates a high incidence of tetanus in areas where the prevalence of tungiasis is high. In areas of Northeast Brazil, monthly incidence of tetanus cases has paralleled the seasonal variation of tungiasis. Thus, tetanus prophylaxis should be kept up to date in areas where tungiasis is common. [48]
Pathophysiology
The primary complicating factor of tungiasis infection is the bacterial superinfections that can result from loss of integrity of the skin structures on the feet and thus a cellulitis and spreading infection. With repeated and extensive infections, pain and difficulty walking are significant contributors to morbidity.
-
A. Tangential cut through a fully developed, gravid flea embedded in the stratum corneum of the epidermis. The flea's head and thorax are enfolded in the hypertrophic anterior abdominal segments. The epidermis is hyperplastic and shows papillomatosis, parakeratosis, and hyperkeratosis.B. Tangential cut through the posterior abdominal segments of an embedded sand flea. Next to the chitinous cuticle, a microabscess has formed.C. Dead parasite; the exoskeleton of the posterior abdominal segment has remained intact; the cuticle has disintegrated at the epidermal–dermal interface. The carcass is infiltrated by neutrophils, and pus has formed.D. The head of the flea is located at the epidermal–dermal interface, has penetrated the basal membrane, and is surrounded by many erythrocytes, presumably having leaked from a blood vessel. The abdomen of the parasite is separated from host tissue by a thick, chitinous cuticle.
-
A tungiasis lesion in substage 3a.
-
Scanning electron micrograph of flea on day 3 after penetration. The hypertrophic zone between abdominal segments 2 and 3 is gaining a bulging shape and looks like a life-belt (x100).
-
Scanning electron micrograph of flea on day 8 after penetration. The hypertrophy zone has taken the shape of a sphere. The 3 parts of abdominal segment 2 are completely bent apart. Together with the newly developed, crescent-shaped chitinous clasps, the anterior part of the flea looks like a 3-leafed clover (x32).
-
Scanning electron micrograph of flea 6 hours after beginning of penetration. The penetration is almost completed; only the last abdominal segments protrude through the skin (x240).
-
Scanning electron micrograph of flea in stage 2. The rear end, the genital opening, and the 4 pairs of stigmata form a miniature cone, which towers above the crater caused by pushing in abdominal segments 7 and 8 (x190).
-
Life cycle of Tunga penetrans - Fortaleza stages included. Compiled and designed by Fausto Bustos and Lucas Manfield.
-
Histopathologic findings in tungiasis.
-
Life cycle of the chigoe flea, Tunga penetrans. Courtesy of the CDC.
-
Complicated Tungiasis infection. Courtesy of Dermatology Atlas (https://www.atlasdermatologico.com.br/index.jsf) and Samuel Freire da Silva, MD.
-
Tungiasis lesion under toenail. Courtesy of Dermatology Atlas (https://www.atlasdermatologico.com.br/index.jsf) and Samuel Freire da Silva, MD.
-
Example of complicated infection with multiple tungiasis lesions and possible secondary infection. Courtesy of Wikimedia Commons [author R Schuster, https://commons.wikimedia.org/wiki/File:Jigger_infested_foot_(2).jpg].
-
Illustration of Tunga penetrans (sand flea) in its enlarged state. Courtesy of Wikimedia Commons [https://commons.wikimedia.org/wiki/File:ChiggerBMNH.jpg].
-
Removed parasite shown with needle. Courtesy of Wikimedia Commons [https://commons.wikimedia.org/wiki/File:Puce_chique_(Tonga_penetrans).jpg].
-
Tunga penetrans flea. Courtesy of Wikimedia Commons [author Philipp Weigell, https://commons.wikimedia.org/wiki/File:Tunga_penetrans_%281%29.JPG].
-
Image of Tungiasis infection on both feet. Courtesy of PLOS [Miller H, Ocampo J, Ayala A, Trujillo J, Feldmeier H. Very severe tungiasis in Amerindians in the Amazon lowland of Colombia: A case series. PLOS Neglected Tropical Diseases. 2019 Feb 7. Online at: https://journals.plos.org/plosntds/article?id=10.1371/journal.pntd.0007068.].
-
Graphical abstract of predicted tungiasis occurrence within sub-Saharan Africa. Courtesy of MDPI [Deka MA. Mapping the Geographic Distribution of Tungiasis in Sub-Saharan Africa. Tropical Medicine and Infectious Disease. 2020 Jul 24;5(3):122. Online at: https://www.mdpi.com/2414-6366/5/3/122#.].
Tables
Medication Name |
Dosage/Application |
Contraindications |
Availability |
Notes |
|---|---|---|---|---|
Apply directly to the affected area once or twice daily.
If legion numbers are under 40 or legions are in clusters: Apply 3 drops of NYDA® (approximately 50 μL each) to the exposed posterior side of the flea. Repeat the procedure 3x over 10 minutes.
If fleas are in excessive hyper-keratotic skin and located on top of each other: NDYA® must be used to wet the skin intensely and repeatedly. |
No known contraindications. Shown to be safe for extended use. |
Available under the brand name NYDA®. But not available in all tungiasis endemic areas. |
||
0.8% ivermectin, 0.2% metrifonate and 5% thiabendazole lotions, applied 2 consecutive days. |
No contraindications reported. |
All are readily available except for metrifonate, which is no longer commercially available. |
||
Apply to all infected areas and areas at risk for tungiasis infection twice daily. |
No known contraindications. |
No longer commercially available, but made of ingredients that could be locally manufactured in areas where tungiasis is common. |
||
One drop (approximately 0.05 ml) of a mixture of 20% cold-pressed virgin neem seed oil and 80% virgin coconut oil applied to the embedded flea’s abdominal tip on days 1 and 3. |
Actives in cold-pressed neem oil are not toxic following oral, inhalation, or dermal exposure. |
May be locally available where both neem trees and coconut palms grow. |
The mixture requires proper storage as azadirachtin has a high sensitivity to ultraviolet light, pH, and temperature. |
