Practice Essentials
Arthropod assaults on humans can have many manifestations clinically, histologically, and immunologically. Hemiptera is an order of insect species of "true bugs" that has piercing-sucking mouthparts and includes the family Cimicidae (bedbugs), which are blood-sucking ectoparasites of mammals or birds.
All Cimex species organisms are reddish brown insects. Cimex lectularius is 5-7 mm in size, with the females slightly larger than the males. Cimex hemipterus organisms are approximately 25% longer than C lectularius organisms. Females deposit fertilized eggs in cracks or crevices, with newborns emerging in 4-5 days. Note the images below.
 The bedbug is a flat, oval, reddish brown insect that turns violaceous after feeding. Courtesy of Colonel Dirk M. Elston, MD (from Elston, 2000).
The bedbug is a flat, oval, reddish brown insect that turns violaceous after feeding. Courtesy of Colonel Dirk M. Elston, MD (from Elston, 2000).
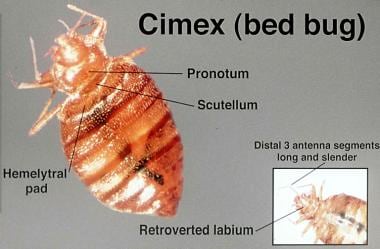
 Bedbugs are parasitic arthropods from the family Cimicidae. They are typically less than 1 cm in length and reddish brown in color. Bedbugs can be found in furniture, floorboards, peeling paint, or other small spaces, most commonly in areas of clutter. These insects come out at night in search of prey upon which to feed, with peak feeding times just before dawn. Bedbugs are typically attracted to body heat, carbon dioxide, vibration, sweat, and odor. The image of a Cimex lectularius is shown courtesy of the US Centers for Disease Control and Prevention (CDC).
Bedbugs are parasitic arthropods from the family Cimicidae. They are typically less than 1 cm in length and reddish brown in color. Bedbugs can be found in furniture, floorboards, peeling paint, or other small spaces, most commonly in areas of clutter. These insects come out at night in search of prey upon which to feed, with peak feeding times just before dawn. Bedbugs are typically attracted to body heat, carbon dioxide, vibration, sweat, and odor. The image of a Cimex lectularius is shown courtesy of the US Centers for Disease Control and Prevention (CDC).
Signs and symptoms
See Presentation.
Diagnostics
Consider appropriate laboratory studies in the context of the clinical picture. Bedbug bites seldom require laboratory tests.
Most reactions to bedbugs show a superficial and deep perivascular mixed inflammatory infiltrate, with eosinophils being prominent rather than neutrophils. Eosinophils may be prominent among collagen bundles, or they may be absent.
Management
Also see Prevention of Bedbug Bites and Special Concerns.
Medical care of bedbug bites depends on the patient's clinical picture. Treatment of these bites is not usually required. However, if secondary infection occurs, apply local antiseptic lotion or antibiotic cream or ointment. Creams with corticosteroids and oral antihistamines may be advised in the presence of an allergic reaction. Infestation often leads to nervousness, anxiety, and insomnia. [1]
Also see Papular Urticaria and Acute Urticaria for complete information on these topics.
Background
Bedbug infestations seem to be increasing around the world at an alarming rate, possibly due to insecticide resistance. [2] Resistance to pyrethroid insecticides is already widespread in the United States. The bedbug occurs in aggregations when conditions are favorable, but the arthropods disperse when conditions are unfavorable. [3] Active female dispersal can potentially lead to treatment failures and should be taken into account when using control methods.
New tactics may be needed for this escalating public health concern in locations with high occupant turnover, such as hotels, hospitals, and nursing homes. [1] Indeed, in the past decade bedbugs have become a worldwide urban pest, with the number of American households affected markedly increased. [4] Genetic data suggest that C lectularius may be undergoing lineage divergence through host association. [5]
Bedbugs have two barriers with distinct temperature-sensitive and lipid-based physicochemical properties to protect them against insecticides. [6] More research on the bedbug is desirable, including use of autofluorescence lifetime measurements to analyze the bedbug arthropod cuticle. [7]
The tropical bedbug (Cimex hemipterus) has reappeared in Florida after nearly 60 years [8] and has been described in Italy. [9] C hemipterus is behaviorally and biologically similar to C lectularius. How this particular type of bedbug was reintroduced is unknown, and more research is needed to determine its distribution and how established it is.
Pathophysiology
The mechanism of skin injury by arthropods depends on the structure of the mouthparts. These insects are categorized as vessel feeders if they insert the tip into a capillary or as pool feeders if they feed on the extravasated blood from damaged tissue. They often inject different pharmacologically active substances (eg, hyaluronidase, proteases, kinins), which may cause different skin reactions (eg, erythema, wheal, vesicle, hemorrhagic nodule). See the following images.
 Bedbugs feeding on a human host. Courtesy of Colonel Dirk M. Elston, MD (from Elston, 2000).
Bedbugs feeding on a human host. Courtesy of Colonel Dirk M. Elston, MD (from Elston, 2000).
 After bedbugs find a food source, they bite down with their mouths and inject anticoagulant and anesthetic compounds into the skin. Depending on the species, these parasites feed on the host blood via 1 of 2 mechanisms. Vessel feeders directly insert their mouthparts into superficial capillaries, whereas pool feeders damage the superficial tissue and feed on the accumulated blood. As bedbugs feed, their color may change as they swell with the host blood, as shown in this picture of a larval bedbug feeding on a volunteer host. Image courtesy of the US Centers for Disease Control and Prevention (CDC).
After bedbugs find a food source, they bite down with their mouths and inject anticoagulant and anesthetic compounds into the skin. Depending on the species, these parasites feed on the host blood via 1 of 2 mechanisms. Vessel feeders directly insert their mouthparts into superficial capillaries, whereas pool feeders damage the superficial tissue and feed on the accumulated blood. As bedbugs feed, their color may change as they swell with the host blood, as shown in this picture of a larval bedbug feeding on a volunteer host. Image courtesy of the US Centers for Disease Control and Prevention (CDC).
Bite reactions
The type of reaction provoked depends on previous exposure; repeated bites may lead to an allergic reaction, which may lead to pronounced cutaneous manifestations. Some patients show a severe systemic hypersensitivity to arthropod allergens. The site of the bite can also become secondarily infected with bacteria infection and lead to ecthyma, cellulitis, and/or lymphangitis.
See the image below.
 Bedbug bites themselves are typically painless. However, the subsequent allergic reaction that may develop can cause intense pruritus. While feeding, bedbugs may inject one of several pharmacologically active substances, including hyaluronidase, proteases, and kinins. These compounds may induce different skin reactions, such as erythema, wheals, vesicles, or hemorrhagic nodules. Repeated bites may sensitize individuals, leading to more pronounced cutaneous manifestations or systemic hypersensitivity reactions. The local trauma from bedbug bites can lead to secondary bacterial infection, causing ecthyma, cellulitis, or lymphangitis. There is some evidence that bedbugs may also be a vector for hepatitis B and Chagas disease. Histologic findings from bite-site biopsy specimens typically show eosinophilic infiltrates, which are indicative of the allergic nature of the reaction. The image shown is papular urticaria, which may develop from bedbug bites.
Bedbug bites themselves are typically painless. However, the subsequent allergic reaction that may develop can cause intense pruritus. While feeding, bedbugs may inject one of several pharmacologically active substances, including hyaluronidase, proteases, and kinins. These compounds may induce different skin reactions, such as erythema, wheals, vesicles, or hemorrhagic nodules. Repeated bites may sensitize individuals, leading to more pronounced cutaneous manifestations or systemic hypersensitivity reactions. The local trauma from bedbug bites can lead to secondary bacterial infection, causing ecthyma, cellulitis, or lymphangitis. There is some evidence that bedbugs may also be a vector for hepatitis B and Chagas disease. Histologic findings from bite-site biopsy specimens typically show eosinophilic infiltrates, which are indicative of the allergic nature of the reaction. The image shown is papular urticaria, which may develop from bedbug bites.
Thus, although these insects usually cause mild cutaneous reactions, more severe responses, including anaphylaxis, may occur. [10] Bullae may be noted. Skin responses at bite sites may evolve from immediate, pruritic, edematous macules into bullae within 24 hours. Histopathologically, an urticarial-like reaction can develop into a leukocytoclastic vasculitis, sometimes with a destructive, necrotizing, eosinophil-rich vasculitis with prominent infiltration of CD68+ histiocytes and collagen necrobiosis.
Insect bites, including those from the bedbug, have been proposed as a factor contributing to the formation of a cutaneous reaction termed papular urticaria. Patients with papular urticaria have been shown to demonstrate immunoglobulin (Ig) G antibodies to bedbug (C lectularius) antigens. [11] Thus, IgG against C lectularius, Cimex pipiens, and Pulex irritans in patients with papular urticaria may contribute the pathogenesis of this condition.
Host susceptibility
Susceptibility to arthropod bites depends on many external factors, such as occupation, conditions of employment, cohabitation with a variety of domestic animals, housing, climate, and clothing. An arthropod is usually attracted to its host by body heat, carbon dioxide in exhaled air, vibration, human sweat, and/or odor. The Cimex (bedbug) genus attacks both mammals and birds. C hemipterus (the tropical bedbug) bites mostly humans and is found in warm climates, whereas C lectularius (the common bedbug) also attacks bats and domestic animals, such as chickens.
Bedbug feeding
Bedbugs are 5-7 mm in length with reduced wings and modified mouthparts for piercing and sucking. These insects live between wooden floorboards, in furniture, in bed frames, in mattresses, or behind peeling paint. Bedbugs sneak out to grasp human skin with their forelegs, pierce the skin, and inject anticoagulant- and anesthetic-containing saliva.
Bedbugs normally feed at night, usually approximately 1 hour before dawn. However, if the conditions are favorable, they also feed during the day. Feeding takes 3-12 minutes. In proper conditions, adult bedbugs can survive without a meal for 1 year or longer. Each female lays approximately 300 eggs in her lifetime. The eggs hatch in 10 days. The nymph stage lasts 6 weeks, undergoing 5 molts.
Etiology
Bedbugs can be seen anywhere, but they tend to occur in environments in disarray. Old furniture makes an excellent home for bedbugs. These insects also like to hide in the seams and folds of mattresses and in bed frames and springs.
Passenger ships provide conditions suitable for the survival and growth of many pest populations. In a 2008 study, pest infestations were identified in 21 ferries: 18 with flies, 11 with cockroaches, and with 3 with bedbugs. [12]
Epidemiology
Bedbug infestations affect both sexes and people of all ages and races in the United States and globally, particularly in poor regions of the world. [13] The reported rate of bedbugs (Cimex hemipterus) was 37.5% in children's beds from a rural region of Gambia. Recently, bedbugs were allegedly reintroduced from abroad into Seoul, Korea, because there had been no reports on bedbugs in Seoul for more than 20 years. [14]
Prognosis
The prognosis for bedbug bites is excellent, although these bites can create considerable anxiety and localized and occasionally systemic reactions. Sometimes, if the bite reactions are intensely pruritic, scratching with excoriations may be complicated by impetigo.
In addition, bedbugs may be a vector for hepatitis B [15] and, in endemic areas, for American trypanosomiasis (Chagas disease). [16, 17] Of note, reports have indicated the risk of insect transmission of human immunodeficiency virus (HIV), if any, is extremely low and likely nonexistent. [18, 19]
Anaphylactoid reactions are well described. One such case occurred in a 41-year-old businessman in a first-class urban hotel in the United States.
Patient Education
Educate the patient and family about bedbugs and their habits. Patients should avoid scratching the bite sites to reduce local irritation and prevent secondary infection. See also Prevention of Bedbug Bites.
-
The bedbug is a flat, oval, reddish brown insect that turns violaceous after feeding. Courtesy of Colonel Dirk M. Elston, MD (from Elston, 2000).
-
Bedbugs feeding on a human host. Courtesy of Colonel Dirk M. Elston, MD (from Elston, 2000).
-
Human infestation with bedbugs, lice, and mites are common causes of dermatologic symptoms. Although these organisms thrive in conditions of overcrowding and decreased sanitation, Americans of all socioeconomic backgrounds may be at risk for infestation. Clinicians must maintain high suspicion in the appropriate set of clinical circumstances to identify and treat infestations, as they can cause substantial dermatologic and psychological discomfort for patients. Images courtesy of the US Centers for Disease Control and Prevention.
-
Bedbugs are parasitic arthropods from the family Cimicidae. They are typically less than 1 cm in length and reddish brown in color. Bedbugs can be found in furniture, floorboards, peeling paint, or other small spaces, most commonly in areas of clutter. These insects come out at night in search of prey upon which to feed, with peak feeding times just before dawn. Bedbugs are typically attracted to body heat, carbon dioxide, vibration, sweat, and odor. The image of a Cimex lectularius is shown courtesy of the US Centers for Disease Control and Prevention (CDC).
-
After bedbugs find a food source, they bite down with their mouths and inject anticoagulant and anesthetic compounds into the skin. Depending on the species, these parasites feed on the host blood via 1 of 2 mechanisms. Vessel feeders directly insert their mouthparts into superficial capillaries, whereas pool feeders damage the superficial tissue and feed on the accumulated blood. As bedbugs feed, their color may change as they swell with the host blood, as shown in this picture of a larval bedbug feeding on a volunteer host. Image courtesy of the US Centers for Disease Control and Prevention (CDC).
-
Bedbug bites themselves are typically painless. However, the subsequent allergic reaction that may develop can cause intense pruritus. While feeding, bedbugs may inject one of several pharmacologically active substances, including hyaluronidase, proteases, and kinins. These compounds may induce different skin reactions, such as erythema, wheals, vesicles, or hemorrhagic nodules. Repeated bites may sensitize individuals, leading to more pronounced cutaneous manifestations or systemic hypersensitivity reactions. The local trauma from bedbug bites can lead to secondary bacterial infection, causing ecthyma, cellulitis, or lymphangitis. There is some evidence that bedbugs may also be a vector for hepatitis B and Chagas disease. Histologic findings from bite-site biopsy specimens typically show eosinophilic infiltrates, which are indicative of the allergic nature of the reaction. The image shown is papular urticaria, which may develop from bedbug bites.
-
Treatment for bedbug bites is typically supportive. Local antiseptic lotions or antibiotic creams can be applied for secondary infections, whereas corticosteroid creams and oral antihistamines can be used for allergic reactions. Bedbugs can be eliminated through the use of permethrin insecticides, baited traps, special bedbug-free beds, and bed nets. Homemade methods, such as wrapping duct tape around bed legs as shown, may be effective, but bedbugs have been known to climb other objects and then fall down onto a bed. Image courtesy of Wikimedia Commons.
