Practice Essentials
Cherry hemangiomas are the most common cutaneous vascular proliferations. They are often widespread and appear as tiny cherry-red papules or macules. Longstanding lesions enlarge slowly over time and take on the appearance of a dome topped with cherry-red to deep-purple papules.
Signs and symptoms
Cherry angiomas typically present in the third or fourth decades of life, and early lesions may appear as small red macules. Lesions may be found on all body sites, but usually, the mucous membranes are spared. Most patients report an increase in number and size of individual lesions with advancing age.
Cherry angiomas can be found on every aspect of the integument—both in sun-exposed and in non‒sun-exposed areas, even including the scalp and genitalia. [1]
A study of a general population cohort of 163 subjects in Brisbane, Australia found the anterior trunk to be the most common site of cherry hemangiomas, followed by the posterior trunk. [2]
On physical examination, lesions may have a variable appearance, ranging from a small red macule to a larger dome-topped or polypoid papule. The color of the lesions typically is described as bright cherry red, but the lesions may appear more violaceous (purple) over time (see the image below).
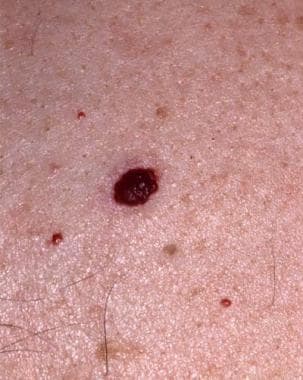 A large polypoid angioma, deeply red to violaceous cherry, appears in the center of the field. Surrounding the angioma are several small bright red macules and papules that represent cherry hemangiomas in the earlier stages of evolution.
A large polypoid angioma, deeply red to violaceous cherry, appears in the center of the field. Surrounding the angioma are several small bright red macules and papules that represent cherry hemangiomas in the earlier stages of evolution.
Rarely, a lesion demonstrates a dark brown to an almost black color when a hemorrhagic plug occupies the vascular lumen, often raising concern about the possibility of a malignant melanoma.
Complications
Cherry angiomas are, by definition, benign; however, periodically these lesions may experience trama and bleed profusely or become inflamed and thrombosed. Hemorrhages and secondary infection may complicate the course of traumatized lesions, often requiring surgical removal of the inflamed angioma.
The gradual appearance of multiple cherry angiomas over many years is common and often is expected; however, the sudden appearance of multiple cutaneous lesions always should raise concerns that the lesions may accompany the development of an internal malignancy.
Diagnostics
The diagnosis of cherry hemangioma is usually made clinically; however, skin biopsy (shave or punch) allows histopathologic confirmation in doubtful situations.
On scanning magnification, a sharply circumscribed vascular proliferation usually is noted, often embraced in part by a collarette of epithelium and adnexal structures. Higher magnification demonstrates numerous venules in a thickened papillary dermis. Older lesions often display prominent collagen bundles, which is an appearance suggesting septa.
On dermoscopy, cherry hemangiomas may show a red to reddish-white area without structures, similar to pyogenic granuloma. [3]
Management
Medical intervention is not helpful and not indicated in the treatment of the benign vascular proliferations of cherry hemangiomas. Perform biopsy on lesions in which the diagnosis is doubtful. The biopsy procedure may be used as a therapeutic measure to remove traumatized or bleeding lesions.
Treatment for cherry hemangioma lesions is recommended only in situations of irritation or hemorrhage or in instances in which the lesions are deemed by the patient to be cosmetically undesirable.
Shave excision allows delicate removal of the lesion by blade and histologic confirmation of the diagnosis. Hemostasis following removal may be obtained by chemical means (aluminum chloride) or by performing electrocautery.
Curettage and electrodesiccation techniques permit reliable elimination of the lesion through tissue destruction. The risk of scarring usually is minimal when the technique is performed by a skilled operator.
Pulsed-dye laser ablation of lesions may be performed for cosmesis. The use of a pulsed dye laser with a green light source allows selective absorption of the laser energy by the hemoglobin contained within the red blood cells and subsequent obliteration of the vascular lumen. [4, 5, 6]
Cryotherapy is a less well-controlled means by which lesions are eliminated through irritation, coagulation, and subsequent destruction.
Sclerotherapy of individual lesions has been shown to have limited therapeutic benefit in treating cherry angiomas. [7]
Calik et al reported good results from focused, high-intensity ultrasound treatment at 20 MHz of cherry hemangiomas in a single patient. [8]
Follow-up evaluations usually are arranged approximately 1 month after initial therapy. Occasionally, more than a single treatment is required to eliminate the lesion(s). If the lesions are numerous and present as small macules, consider a bleeding disorder such as thrombocytopenia.
Dermatologist consultation may be indicated. For multiple cherry hemangiomas that have appeared over a short period, refer the patient for evaluation to exclude an internal malignancy. In several patients, cherry hemangiomas that have erupted over a very short period were associated with an internal malignancy. [9]
Pathophysiology
Involvement of cherry hemangiomas is limited to the skin. These benign lesions are formed by a proliferation of dilated venules.
Etiology
Little is known about the factors that contribute to the formation of cherry hemangiomas. Several reports have described the appearance of many small red papules histologically resembling cherry hemangiomas in patients with malignancies, [9, 10] in association with segmental dyschromatosis and blue nevi, [11] as part of a viral xanthem, [12] , as a manifestation of immunoglobulin type gamma 4-related disease (IgG4-RD), [13] and following treatment with topical nitrogen mustard therapy. [14, 15] However, the vast majority of cherry angiomas occur in healthy patients.
Notably, there is a reported case of cherry hemangioma appearance in a 12-year-old boy after COVID vaccine (Pfizer BioNTech) administration. [16]
Epidemiology
Frequency
Frequency of cherry hemangiomas increases with age in both sexes and all races. The incidence of cherry angiomas is uniform across all races, but individual lesions are most noticeable in pale-skinned individuals. Approximately 5% to 41% of people begin to have cherry hemangiomas in their twenties. [17]
Race-, sex-, and age-related information
Cherry hemangiomas are found in individuals of all races and ethnic backgrounds.
No distinction can be made on the basis of sex. However, a general population cohort study of 163 participants found that males had a median of 16 cherry angiomas versus 12 for females. [2]
Cherry hemangiomas occur more frequently with increasing age. In the past, the lesions often were referred to as senile angiomas.
Prognosis
Lesions are benign and usually do not undergo spontaneous involution. Patients may demonstrate considerable concern regarding the cosmetic appearance of the lesions.
In very rare situations, eruptive cherry angiomas have been observed to portend the diagnosis of a systemic malignancy [9] or be associated with topical nitrogen mustard therapy. [14, 15]
Patient Education
Patients rarely require little more than the reassurance that cherry angiomas are benign lesions and are not skin cancer. Occasionally, removal of a lesion that has been traumatized is necessary, or a patient requests removal of lesions because of cosmetic concerns.
-
A large polypoid angioma, deeply red to violaceous cherry, appears in the center of the field. Surrounding the angioma are several small bright red macules and papules that represent cherry hemangiomas in the earlier stages of evolution.
