Practice Essentials
Ankle dislocation is a relatively common type of dislocation encountered in the emergency department. It occurs in 2 forms: (1) true dislocation without fracture and (2) fracture-dislocation, which occurs in the vast majority of cases. The ankle joint is composed of 3 main articulations: the talocalcaneal (subtalar), transverse-tarsal (talocalaneonavicular), and tibiotalar (talocrural) joints. The true ankle joint is the tibiotalar joint (between the tibia, fibula, and talus). The combination of these joints gives the foot the ability to compensate for loads placed during walking and other activities. [1]
The human ankle maintains its range of motion under extremely heavy loads and can support several times the human body weight for short periods. Because of stress placed on the ankle as one pushes off in different directions, it is possible to dislocate it by exceeding the ligamentous strength that encloses the ankle. [1]
The stability of the ankle is maintained by 3 groups of ligaments: the tibiofibular syndesmosis, the deltoid ligament, and the lateral collateral ligaments. These ligaments collaboratively limit motion, provide support, and act to resist inversion. [1]
Inspection of the ankle reveals significant edema, with deformity ranging from trace to obvious. Tenting of the skin by the malleoli may be noted. Palpation of the joint reveals tenderness along the joint line, corresponding to areas of capsular or ligamentous disruption. In associated fractures, tenderness, deformity, or tenting proximal to the joint may be seen.
Possible risk factors that may predispose a patient to dislocation include joint hyperlaxity, internal malleolar hypoplasia, peroneal muscle weakness, and a history of prior ankle sprains. [2]
True ankle dislocation without fracture
Dislocation of the upper ankle joint without fracture is described in the literature as very rare. In 33-50%, ankle dislocations are at least first-degree open and are associated with fracture of the tibia, fibula, or talus. [3] Ankle dislocations without fracture occur when significant force applied to the joint results in loss of opposition of the articular surfaces. Because of the large amount of force required and the inherent stability of the tibiotalar joint, dislocation of the ankle joint is rarely seen without an associated fracture. Researchers argue that this is due in part to the strength of the ankle joint ligaments and the relative weakness of the bones that make up the ankle. [2]
A systematic review of English literature identified 154 cases of pure ankle dislocation and demonstrated that sporting accidents (31%) and motor vehicle accidents (30%) are the most common causes. A total of 73% (112/154) of cases occurred in males, and 50% (77/154) were open. [4]
Ankle dislocations are orthopedic emergencies that require immediate treatment to avoid neurovascular impairment. They are usually accompanied by 1 or more comminuted fractures of the ankle mortis. Primary goals of treatment are immediate reduction of the joint and relief of neurovascular stress. External fixation is a prompt, fairly easy treatment that one should keep in mind for pure ankle dislocations. [5]
For ankle dislocations without fracture, imaging via magnetic resonance imaging (MRI) and computed tomography (CT) scan allows a detailed evaluation of injury severity. The decision for further treatment should be based on findings on these scans. Reconstructing the medial and lateral capsular ligaments may be necessary. With a consequent treatment algorithm, a good functional outcome can be achieved. [6]
Fracture-dislocation of the ankle
Fracture-dislocation of the ankle represents substantial injury to the bony and soft tissue structures of the ankle. [7] Bone stabilization, joint immobilization, anatomic reduction, and intervention for soft tissue protection should be performed as early as possible. [8]
Clinical and functional results have been found to be worse in patients with open ankle fractures. [8] Researchers report that with open ankle fractures, the rate of arthrosis increased with age, and use of a syndesmosis screw had a positive but not a statistically significant effect on clinical and functional outcomes. [8]
Open reduction internal fixation (ORIF) is an accepted treatment for displaced tarsometatarsal joint (TMTJ) fracture-dislocations. In general, hardware is routinely removed after 4 months to allow restoration of joint motion and to avoid complications of hardware failure. Little consensus has been reached regarding the optimal time for hardware removal, or whether hardware retention leads to adverse outcomes. Older age has been correlated with lost reduction, and elevated body mass index is correlated with hardware failure. [9]
Distraction arthroplasty is a viable acute and definitive treatment option for ankle fracture in patients with significant medical comorbidities. [10]
A study that aimed to compare functional outcomes after ORIF in ankle fractures with and without dislocation found that ankle fracture-dislocation occurred more frequently in patients who were older, female, and diabetic. At a median follow-up of just over 3 years, functional outcomes after fracture-dislocation were generally poorer than after fracture without dislocation, and patients rated pain on a subscale of the Foot and Ankle Outcome Score (FAOS) assessment as statistically significantly worse. [7]
Some controversy exists regarding the treatment of ankle dislocations. However, outcomes appear to be satisfactory in cases treated with immediate reduction of the joint and relief of neurovascular stress as the primary goals of treatment. [11]
Pathophysiology
The ankle joint is designed for a balance of stability and flexibility, particularly the former. Joint stability is provided by close articulation of the talus with the tibia and fibula. The mortise design further enhances the stability of the configuration.
The ankle joint is composed of 3 main articulations: talocalcaneal (subtalar), transverse-tarsal (talocalaneonavicular), and tibiotalar (talocrural) joints. The true ankle joint is the tibiotalar joint (between the tibia, fibula, and talus). The combination of these joints gives the foot the ability to compensate for loads placed during walking and other activities. [1]
The stability of the ankle is maintained by 3 groups of ligaments: the tibiofibular syndesmosis, the deltoid ligament, and the lateral collateral ligaments. These ligaments collaboratively limit motion, provide support, and act to resist inversion. [1]
The human ankle maintains its range of motion under extremely heavy loads and can support several times the human body weight for short periods. This factor is increased several-fold during running and jumping activities. Because of stress placed on the ankle as one pushes off in different directions, it is possible to dislocate it by exceeding the ligamentous strength that encloses the ankle. [1]
(See the image below.)
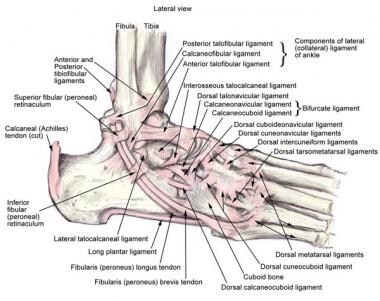 Anatomy of the lateral ankle ligamentous complex and related structures.
Anatomy of the lateral ankle ligamentous complex and related structures.
Epidemiology
Associated fractures are the rule rather than the exception with ankle dislocations. Ligamentous disruption varies according to the type of dislocation. Neurovascular injury is the principal concern, as with any dislocation. Vascular compromise may result in avascular compromise of the talus, permanent sensation or nerve damage, and lower extremity tissue necrosis; gangrene may occur if the fracture is not promptly reduced. Tented skin may be subject to ischemic necrosis
Children and adolescents have the most ankle dislocations. Dislocations of the ankle are seen more frequently in young males than in any other group. This presumably is related to their increased risk overall for traumatic injury.
A retrospective study of patients with major intra-articular fracture-dislocations reported that major joint fracture-dislocations were most common in the hip and least common in the knee and occurred more often in men than in women. The hip was the most commonly affected joint in men, and the ankle was most commonly affected in women. [12]
Postmenopausal women are at higher risk for associated fractures with ankle dislocation. Increased fracture risk probably is related to osteoporotic changes in this subset of patients.
Prognosis
Dislocated ankles should not be expected to return to premorbid function.
The amount of force and the level of capsular disruption required to dislocate the inherently stable joint can lead to significant injury with lasting effects. To a limited extent, prompt intervention can reduce the risk of complications.
Most cases of pure ankle dislocation treated with early reduction followed by a short period of immobilization and functional rehabilitation have good clinical outcomes. [4]
A study of ankle dislocation involving posterior ankle comminuted fractures reported that the intraoperative ankle dislocation approach appears to be a promising surgical option, providing better functional outcomes and a lower incidence of posttraumatic arthritis than conventional approaches, while not compromising primary healing and healing time. [13]
-
Anatomy of the lateral ankle ligamentous complex and related structures.
