Practice Essentials
Electrical injuries have become a more common form of trauma with a unique pathophysiology and with high morbidity and mortality. They encompass several types, as follows: lightning injury, [1] high-voltage injury, and low-voltage injury. [2, 3, 4] Clinical manifestations range from transient unpleasant sensations without apparent injury to massive tissue damage. [5] Some electrocutions are instantly fatal. Familiarity with the mechanisms of injury and the principles of therapy improves patient care. [6]
Four classes of electrical injuries are as follows [7] :
-
True electrical injuries - The person becomes part of the electrical circuit and has an entrance and exit site
-
Flash injuries - Superficial burns caused by arcs that burn the skin; no electrical energy travels through the skin
-
Flame injuries - Caused by ignition of the persons clothing by arc; electricity may or may not travel through the person’s body
-
Lightning injuries - A unique type of injury that occurs at extremely high voltages for the shortest duration; the majority of electrical flow occurs over the body
See the images below.
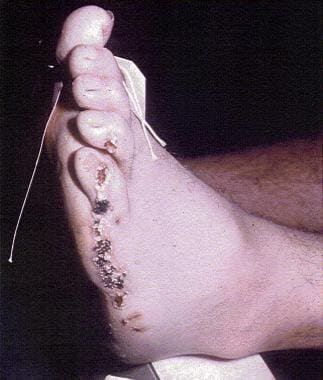 Arcing electrical burns through the shoe around the rubber sole. High-voltage (7600 V) alternating current nominal. Note cratering.
Arcing electrical burns through the shoe around the rubber sole. High-voltage (7600 V) alternating current nominal. Note cratering.
 Contact electrical burn. This was the ground of a 120-V alternating current nominal circuit. Note vesicle with surrounding erythema. Note thermal and contact electrical burns cannot be distinguished easily.
Contact electrical burn. This was the ground of a 120-V alternating current nominal circuit. Note vesicle with surrounding erythema. Note thermal and contact electrical burns cannot be distinguished easily.
 Contact electrical burns, 120-V alternating current nominal. The right knee was the energized side, and the left was ground. These are contact burns and are difficult to distinguish from thermal burns. Note entrance and exit are not viable concepts in alternating current.
Contact electrical burns, 120-V alternating current nominal. The right knee was the energized side, and the left was ground. These are contact burns and are difficult to distinguish from thermal burns. Note entrance and exit are not viable concepts in alternating current.

Signs and symptoms of electrical injuries
Clinical presentations range from a tingling sensation to a widespread tissue damage and even to instantaneous death. The main symptom of an electrical injury is often a skin burn. Cardiac arrhythmias can also occur. The following are the most common electrocardiographic abnormalities:
-
Sinus tachycardia
-
Nonspecific ST- and T-wave changes
-
Heart blocks
-
Prolongation of the QT interval
Diagnosis
Laboratory studies
Indicated laboratory studies include the following:
-
Complete blood cell count
-
Serum electrolyte levels
-
Liver function tests
-
Blood urea nitrogen and creatinine levels
-
Creatine kinase measurement
-
Urinalysis
Imaging studies
Radiographs of the cervical spine, chest, and pelvis should be ordered if the patient was previously unconscious. In addition, appropriate extremity radiographs should be obtained in patients with obvious extremity injuries
Other tests
An electrocardiogram should be obtained in all patients. If smoke inhalation is suspected, arterial blood gas analysis and pulse oximetry may be indicated.
See Workup for more detail.
Management
Patients with electrical injury should be initially evaluated as a trauma patient. Airway, breathing, circulation, and inline immobilization of the spine should be performed as a part of the primary survey. Maintain a high index of suspicion and evaluate for hidden injuries. Intravenous access, cardiac monitoring, and measurement of oxygen saturation should be started during the primary survey. Fluid replacement is the most important aspect of the initial resuscitation.
See Treatment for more detail.
Patient education
Since most electrical injuries are preventable, prevention, education, and adherence to safety measures both at home and at work constitute the most important aspect of management. [8]
History of the Procedure
Ever since Franklin's experiments with lightning, people have been fascinated with electricity; however, the widespread use of electricity and the application of electrically powered machinery have caused an increase in the number of electrical injuries. [9] Samuel W. Smith was the first person in the United States to die after electrocution by a generator in Buffalo, New York, in 1881.
Problem
To fully understand such injuries, understanding certain basic electrical principles is necessary.
Direct current (DC) flows in a constant direction. Batteries, for example, deliver direct current. High-voltage direct current is used as a means for the bulk transmission of electrical power.
Alternating current (AC) is an electric flow that regularly reverses its direction. Each forward-backward motion interval is called a cycle. Electric current in the United States alternates with a frequency of 60 hertz (Hz). The usual waveform of an AC power circuit is a sine wave, because this results in the most efficient transmission of energy, but, at the same time, it is also more dangerous than DC. AC is standard in US electrical outlets.
A volt is a unit of electromotive force or pressure that causes current to flow. In US household wiring, 120 volts are present between the hot wire and the ground wire. Most electrical shocks come from constant voltage sources; that is, the actual number of volts present does not change appreciably over time, despite variable current drainage from the source. Nonconstant voltage sources, such as cardiac defibrillators and capacitors, deliver varying voltages.
The use of a higher voltage leads to more efficient transmission of power; therefore, it is advantageous when transmitting large amounts of power to distribute the power with extremely high voltages (sometimes as high as hundreds of kilovolts). However, high voltages also have disadvantages, the main ones being the increased danger to anyone who comes into contact with them, the extra insulation required, and the increased difficulty in their safe handling.
An ampere is a unit of electrical current. More precisely, it is the flow of a certain number of electrons per second.
An ohm is a unit of electrical resistance. Conductance is defined as 1/resistance (ie, the inverse of resistance). The resistance of a material to current flow depends on the physical and chemical properties of the material. The amount of current flow often determines the magnitude of injury. Ohm law states that current is directly proportional to the voltage and inversely proportional to resistance (I=V/R) and can be useful for calculating the current flow during electric shock. [10, 11]
Heat generated in a material due to current flow is an indication of power. A watt is the unit of electrical power that is delivered when 1 ampere flows through 1 ohm for 1 second. Power is equal to voltage multiplied by current (P=VxI). Energy is defined in terms of a watt-second. One watt-second is equal to 1 joule. One watt of power delivered for 1 second produces 0.24 calories of heat. [10, 11]
Epidemiology
Electrical injuries result in an estimated 1000 deaths per year and about 3000 admissions to specialized burn centers per year. Up to 40% of serious electrical injuries are fatal. [2, 3, 4] A retrospective study reported that patients who had sustained high-voltage injuries (>1000 volts) were more likely to be male. [12]
According to the Centers for Disease Control and Prevention (CDC), 444 lightning-related deaths were reported in the United States between 2006 and 2021. There were 19 deaths in 2022 and 13 in 2023. [13] The chances of being struck by lightning are increased by wearing or carrying a metal object or simply being wet.
An epidemiological study of 383 cases in China underscores the need for stronger preventive measures. [14]
Etiology
Approximately 20% of all electrical injuries occur in children, with a bimodal peak incidence highest in toddlers and adolescents. Most electrical injuries that occur in children are at home, with extension cords (60-70%) and wall outlets (10-15%) being by far the most common sources in this age group. [15] Electrical burns account for 2-3% of all burns in children that require emergency department care.
In adults, most electrical injuries happen at the workplace and constitute the fourth leading cause of work-related traumatic death. One third of all electrical traumas and most high-voltage injuries are job related. More than 50% of these occupational electrocutions result from power line contact (5-6% of all work-related deaths), and 25% result from using electrical tools or machines. The annual occupational death rate from electricity is 1 death per 100,000 workers, with a male-to-female ratio of 9:1. [4]
Pathophysiology
The 3 major mechanisms of electricity-induced injury are as follows [6, 10, 11] :
-
Electrical energy causing direct tissue damage, altering cell membrane resting potential, and eliciting muscle tetany.
-
Conversion of electrical energy into thermal energy, causing massive tissue destruction and coagulative necrosis.
-
Mechanical injury with direct trauma resulting from falls or violent muscle contraction.
Factors that determine the degree of injury include the magnitude of energy delivered, resistance encountered, type of current, current pathway, and duration of contact. Systemic effects and tissue damage are directly proportional to the magnitude of current delivered to the victim. Current flow (amperage) is directly related to voltage and inversely related to resistance, as dictated by Ohm law (I=V/R; where I=current, V=voltage, R=resistance). Of the parameters described by Ohm law, voltage usually can be determined and is used to gauge the potential magnitude of current exposure and, therefore, the magnitude of injury. [6, 10, 11]
Electrical shock is classified as high voltage (>1000 volts) or low voltage (< 1000 volts). As a general rule, high voltage is associated with greater morbidity and mortality, although fatal injury can occur at household current (110 volts).
AC is substantially more dangerous than DC. Contact with AC may cause tetanic muscle contraction, preventing the victim from releasing the electrical source and, thereby, increasing the duration of contact and current delivery. Thoracic muscle tetany involving the diaphragm and intercostal muscles can result in respiratory arrest. The repetitive nature of AC increases the likelihood of current delivery to the myocardium during the vulnerable recovery period of the cardiac cycle, which can precipitate ventricular fibrillation. In contrast, DC usually causes a single violent muscle contraction, often thrusting the victim away from the source. Lightning is a unidirectional massive current that lasts from 1/10 to 1/1000 of a second, but often has voltages that exceed 10 million volts.
The most important difference between lightning and high-voltage electrical injuries is the duration of exposure to the current. [2, 3] Body tissues differ in their resistance. In general, tissues with high fluid and electrolyte content conduct electricity better. Bone is the tissue most resistant to the flow of electricity. Nerve tissue is the least resistant, and together with blood vessels, muscles, and mucous membranes offers a path of low resistance for electricity. Skin provides intermediate resistance and is the most important factor impeding current flow. Skin is the primary resistor against electrical current, and its degree of resistance is determined by its thickness and moisture. It varies from 1000 ohms for humid thin skin to several thousand ohms for dry calloused skin.
The current pathway determines which tissues are at risk and what type of injury is observed. Electrical current that passes through the head or thorax is more likely to produce fatal injury. Transthoracic currents can cause fatal arrhythmia, direct cardiac damage, or respiratory arrest. [16] Transcranial currents can cause direct brain injury, seizure, respiratory arrest, and paralysis.
Electrothermal tissue injury results in tissue edema; therefore, the development of a compartment syndrome can occur in any body compartment. The leg is the site most commonly involved for the development of compartment syndrome.
The current intensity will have a probable effect in the body, determined by the factors discussed above. There may be individual variation on the energy dose for a specific effect. Less energy is generally required in children, who have more water content and thin skin and, hence, better conductivity and less resistance, and in patients under moist conditions.
Current intensity and its expected clinical manifestation are outlined below:
-
1 mA - Not perceptible, probable tingling sensation
-
3-5 mA - "Let go" current for an average child
-
6-8 mA - "Let go" current for an average woman
-
7-9 mA - "Let go" current for an average man
-
16 mA - Maximum current a person can grasp and "let go"
-
16-20 mA - Tetany of skeletal muscles
-
20-50 mA - Paralysis of respiratory muscles (respiratory arrest)
-
50-100 mA - Threshold for ventricular fibrillation
-
Greater than 2 A - Asystole
-
15-30 A - Common household circuit breakers
-
240 A - Maximal intensity of US household current
Presentation
Clinical presentations range from a tingling sensation to a widespread tissue damage and even to instantaneous death. The external resistance to electric flow is offered primarily by the skin and appendages and by the internal resistance of all other tissues, including nerves, blood, muscles, tendons, bone, and fat. Since the skin resistance can be affected by moisture, electric current can be transmitted to deeper structures before it causes significant skin damage. Electric current may be retained in the bones, causing heat and leading to necrosis and coagulation of small- to medium-sized vessels within the muscles and other tissues, almost completely sparing the skin.
Often, the main symptom of an electrical injury is a skin burn. A specific type of burn, called the "kissing burn," occurs at the flexor creases and is related to the current flowing through the opposing skin at the joint when the flexor muscles contract due to tetany. Not all electrical injuries cause external damage; high-voltage injuries may cause massive internal burns and coagulation necrosis along with edema and compartment syndrome. [17] Lightning injury usually causes superficial surface burns. [2, 3]
The heart can be damaged by direct necrosis to the myocardium and by cardiac dysrhythmias. [18] Cardiac arrhythmia can occur and range from benign to fatal. High voltage or DC current usually causes asystole, and AC current usually causes ventricular fibrillation. Ventricular fibrillation is the most common fatal arrhythmia, occurring in up to 60% of patients in whom the current pathway goes from one hand to the other hand. The most common abnormalities seen on an electrocardiogram (ECG) are sinus tachycardia, nonspecific ST- and T-wave changes, heart blocks, and prolongation of the QT interval. [16] In a retrospective analysis that included 480 patients, no late-onset malignant arrhythmias were observed. [19] A case report described coronary artery dissection after electrical injury. [20]
The most common electrical injury seen in children younger than 4 years is the mouth burn. [15] These burns may cause facial deformities and growth problems of the teeth, jaw, and face. If a current travels close to the eyes, it may lead to cataracts. Cataracts can develop within days of the injury or years later.
Acute renal failure can complicate the hospital course due to acute tubular necrosis secondary hypovolemia from third spacing and huge volume shift. Rhabdomyolysis that results from massive tissue necrosis can also cause pigment-induced renal failure.
About two thirds of patients struck by lightning have ruptured eardrums. Autonomic dysfunction can cause pupils that are fixed and dilated or asymmetric, and this finding should not be used as a reason to stop resuscitation. [21] The "locking-on" phenomenon refers to a refractory state of neuromuscular stimulation with tetanic contractions that prevents the victim's hand to release the electrical source.
Electric burn patients may present with bone fractures from either severe muscle contractions (eg, avulsion fractures) or as a result of falls. This is more commonly seen in upper limb long bones and in vertebrae.
Indications
Indications to pursue an evaluation depend on the history. A thorough documentation is essential in the physical examination. As noted above, the type of injury depends on the voltage and the type of current. [22] A low threshold for fasciotomy is indicated because an early fasciotomy may prevent limb ischemia and also may prevent or limit the extent of amputation. Importantly, remember that the superficial appearance of an electrical burn may underestimate the degree of underlying tissue destruction.
Relevant Anatomy
Current travels down the path of least resistance. Nerve and muscle tissues have lower resistance than skin tissue. Understanding that an injured extremity may not show external signs of injury is important. Moreover, injury to deeper tissues may lead to edema and increased intracompartmental pressure.
Contraindications
The liberal indications for fasciotomy cannot be overemphasized because the morbidity associated with a failure to perform a needed fasciotomy far outweighs that caused by the procedure itself. The most important contraindication would be the failure to treat more severely life-threatening injuries or complications of electrical shock or a failure to adequately resuscitate the patient prior to surgical intervention.
Prognosis
The location and extent of injury, the development of complications, and the functional result determine outcome and prognosis. Recent advances in ICU care, resuscitation, nutritional support, and surgical techniques, along with new skin substitutes, have significantly improved outcomes.
Complications
Hopefully, compartment syndrome can be avoided. Other complications include local infection (as with any burn injury), neurologic injury from the initial insult, and complex regional pain syndrome (CRPS). Other associated injuries carry their own list of complications. [23]
Treat wound infections in the standard manner. Early physical and occupational therapy can reduce limb dysfunction (eg, CRPS).
A 10-year retrospective study by Pawlik et al that assessed electrical accident related possible cardiac complications in the emergency department found that of the 149 out of 240 patients who received follow-up cardiac monitoring, four dysrhythmias were recorded; however, no serious cardiac complications occurred. [24]
A retrospective study of 465 patients admitted for electrical injuries in Norway reported no in-hospital or 30-day mortality, and no serious arrhythmias. The results suggest that conscious patients with normal ECGs who have sustained low-voltage injuries can be safely discharged after a clinical assessment. [25]
A study by Stockly et al found that adult patients with electrical injuries reported poorer physical health and were 50% less likely to be employed at 24-month follow-up, compared with patients who had fire-related injuries. They were also more likely to have neuropathy (16.2% vs 7.9%) and to have required an amputation (29.4% vs 5.7%). [26]
-
Arcing electrical burns through the shoe around the rubber sole. High-voltage (7600 V) alternating current nominal. Note cratering.
-
Contact electrical burn. This was the ground of a 120-V alternating current nominal circuit. Note vesicle with surrounding erythema. Note thermal and contact electrical burns cannot be distinguished easily.
-
Contact electrical burns, 120-V alternating current nominal. The right knee was the energized side, and the left was ground. These are contact burns and are difficult to distinguish from thermal burns. Note entrance and exit are not viable concepts in alternating current.
-
Electrical burns to the hand.
