Background
Facial fractures occur for a variety of reasons related to sports participation: contact between players (eg, a head, fist, elbow); contact with equipment (eg, balls, pucks, handlebars); or contact with the environment, obstacles, or a playing surface (eg, wrestling mat, gymnastic equipment, goalposts, trees). Direct body contact accounts for the majority of sports-related injuries, and the most commonly associated soft tissue injuries were found in the head and neck region. [1] Sports such as football, baseball, and hockey account for a high percentage of facial injuries among young adults.
Although most sports-related facial injuries are minor, the potential for serious damage exists. A physician examining these injuries must rapidly assess the patient in a consistent and methodical manner, allowing for prompt diagnosis and appropriate treatment, while considering the physical demands of the sport, as well as the athlete's return to play.
Facial fractures may be associated with head and cervical spine injuries. [2, 3] A review by Boden et al of catastrophic injuries associated with high school and college baseball demonstrated 1.95 direct catastrophic injuries annually, including severe head injuries, cervical injuries, and associated facial fractures. [3]
Fractures of the facial bones require a significant amount of force. The physician must take into account the mechanism of the injury as well as the physical examination findings when assessing the patient.
Forces that are required to produce a fracture of the facial bones are as follows:
-
Nasal fracture – 30 g
-
Zygoma fractures – 50 g
-
Mandibular (angle) fractures – 70 g
-
Frontal region fractures – 80 g
-
Maxillary (midline) fractures – 100 g
-
Mandibular (midline) fractures – 100 g
-
Supraorbital rim fractures – 200 g
Interpersonal facial trauma tends to be of lower energy than vehicular trauma, thus resulting in generally less severe injuries.
Epidemiology
United States statistics
In 2025, Xu and Abramowicz noted that sports injuries account for 11.3-42.1% of facial fractures. [4] Reehal reported that facial fractures represent 4-18% of all sports injuries. [5] A review by Romeo of facial fractures sustained by athletes during sports participation noted that sporting activities account for 3-29% of facial injuries and 10-42% of all facial fractures. [6] Tanaka and colleagues showed that 10.4% of all maxillofacial fractures are related to sports. [7]
In another report, Laskin stated that 250,000 individuals, many of whom were children, experience facial trauma while engaged in athletic activities. [8] The review by Hwang et al demonstrated that athletes aged 11-20 years were the population that accounted for most (40.3%) sports-related facial bone fractures. [1] Additionally, it is estimated more than 100,000 sport-related injuries could be prevented by wearing appropriate head and face protection. [8]
A retrospective study of pediatric sports-related facial fractures identified the most common fractures in the cohort as orbital, mandibular, nasal, and maxillary. Fractures were most often related to participation in baseball/softball and bicycling. [9]
Retrospective analysis demonstrated a significant male predominance (13.75:1) among athletes who sustained sports-related facial bone fractures. [1] The sports most commonly associated with facial fractures were soccer (38.1%), baseball (16.1%), basketball (12.7%), martial arts (6.4%), and skiing/snowboarding (4.7%). [1]
Nearly 75% of facial fractures occur in the mandible, zygoma, and nose. [10] Sports participation is the most common cause of mandibular fractures (31.5%), followed closely by motor vehicle accidents (27.2%). Most mandibular fractures (83% in one study) occur in men. [11] A study of facial fractures sustained during recreational baseball and softball demonstrated that the zygoma or zygomatic arch was the most common fracture subtype, followed by temporoparietal skull fractures and orbital blow-out fractures. [12]
A number of studies in the medical literature, however, indicate that the nasal bones are the most commonly fractured bones in the face, but because many of these patients do not seek medical treatment or the injuries are managed in the outpatient setting, the statistics may not reflect this trend. [2] It is likely that the nasal bones are more commonly fractured because of the lesser degree of force that is required to fracture the bone.
In a study of patients who presented to US emergency departments (EDs) with sports- or recreation-related nasal fracture, Xiao et al found that the most common causes of injury were basketball (23.2%), baseball (17.1%), softball (9.8%), soccer (7.4%), and football (7%). Among pediatric patients, the most frequent cause was baseball (25.1%). [13]
Fractures of the orbit occur more commonly in young adult and adolescent males: the mean age for adult males is 32 years; the mean age for children, 12.5 years, and the majority of orbital fractures occur in boys. In addition to sports-related injuries, injuries sustained in motor vehicle collisions, assaults, and occupational injuries account for the majority of orbital fractures.
International statistics
A UK study of patients with football-related facial injuries showed that 54% of these patients received a diagnosis of facial fracture. The researchers found that the most frequent injury was a midface fracture, and the most common cause was a clash of heads. [14]
In a Finnish study of patients with sports-related nasal fractures, the majority of fractures (56%) were associated with team sports, and contact with another player was the most frequent cause of injury (52% of fractures). Among team sports, basketball posed the highest risk of nasal fracture. [15]
Functional Anatomy
Frontal sinus: Both the anterior and posterior wall may be damaged. Because the posterior wall is adjacent to the dura mater, damage in this region could result in central nervous system (CNS) complications such as a cerebrospinal fluid (CSF) leak or meningitis.
Orbital: The bony orbit (see image below) is composed of 7 bones of varying thickness. The frontal bone forms the supraorbital rim and orbital roof. The medial surface consists of the ethmoid, whereas the greater wing of the sphenoid and the zygoma create the lateral margin. Inferiorly, the floor and infraorbital rim are formed by the zygoma and maxilla. This portion is very thin; therefore, it is the most common site of fracture within the orbit. Fracture of the orbital floor, also known as a blow-out fracture, can result in entrapment of the inferior rectus muscle, limiting upward gaze.
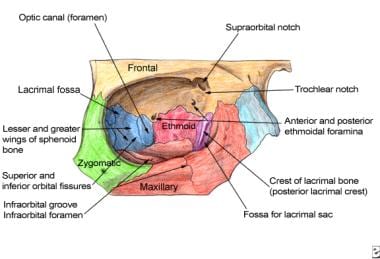
The most common fracture to the orbital rim involves the orbital zygomatic region; this fracture, which typically results from a high-impact blow to the lateral orbit, often results in a fracture to the orbital floor as well.
Nasal: The nose is the most prominent feature of the facial structures and is the most commonly fractured of all facial bones. [5] The upper third of the nose is supported by the paired nasal bones and the frontal process of the maxilla, whereas the lower two thirds of the nose are maintained by cartilaginous structures. A more serious injury, a nasoorbitoethmoid fracture, occurs with trauma to the bridge of the nose. This injury involves extension into the frontal and maxillary bones and can result in disruption of the cribriform plate with concomitant CSF rhinorrhea.
Zygomatic/zygomaticomaxillary complex: The zygoma, like the nasal bones, is a prominent facial bone and, therefore, is prone to injury. Commonly, a breakage in this area involves a central depression with fractures at both ends. The central fragment may impinge upon the temporalis muscles, resulting in trismus. Because of its thickness, isolated fractures of the zygoma are rare, often involving extension into the thinner bones of the orbit or maxilla, otherwise known as zygomaticomaxillary (ie, tetrapod or tripod fractures).
Maxillary (Le Fort): Rene Le Fort first described fractures of the maxillary region in the 1900s (see image below). Classification of maxillary fractures is based on the most superior level of the fracture site. [5]
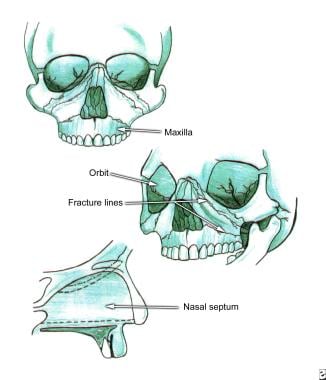
Le Fort I injuries involve a transverse fracture of the maxilla above the level of the root apices and through or below the level of the nose.
Le Fort II injuries traverse the nose, infraorbital rim, and orbital floor and then proceed laterally through the lateral buttress and posteriorly through the pterygomaxillary buttress.
Le Fort III injuries, also known as craniofacial dysjunction, result from motor vehicle or motorcycle accidents and are the result of the mid face being separated from the cranial base.
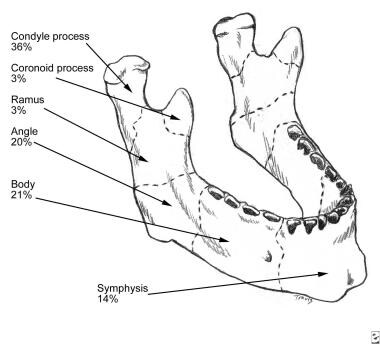
Mandibular: Fractures of the mandible (see image below) can involve the symphysis, body, angle, ramus, condyle, and subcondyle regions. Fractures of the mandibular body, condyle, and angle occur with nearly equal frequency, followed by fractures of the ramus and coronoid process. [5] Generally, motor vehicle accidents result in fractures of the condylar and symphysis regions because the force is directed against the chin, whereas injuries from boxing are more likely to be located in the mandibular angle, as the result of a right-handed punch. Over 50% of mandible fractures are multiple; the presence of one mandibular fracture mandates evaluation for additional fractures, perhaps contralateral to the affected side. [5]
Sport-Specific Biomechanics
In general, facial fractures in athletic activities result from direct trauma over a small surface area. Sports that present a higher risk are those that involve small objects that are propelled at high velocity, such as baseball, softball, hockey, lacrosse, jai alai, and racquetball. Athletes who participate in sports with high levels of physical contact and collision are at risk as well; these sports include football, basketball, rugby, hockey, martial arts, and boxing.
Many of these sports have safety measures to limit the incidence of facial injuries, and attention should be paid to the rules of use. Racquetball players should always play with goggles to limit orbital blow-out injuries. In hockey, face guards with helmets are required in lower levels of play but not at the professional level. High school football players should all have mouthpieces fitted for them, and mouthpieces should be worn in place before every play.
An athlete's vision should be checked as part of a preparticipation physical examination yearly. Visual risk factors include a corrected visual acuity of 20/40 or less or spectacle correction greater than 6 diopters (D). These athletes need an ophthalmologist's evaluation before competing in sports.
A one-eyed athlete is defined as one with a visual acuity in one eye of 20/200 or less. These athletes may be able to participate with proper protection, and an ophthalmologist's evaluation is essential.
-
The bony walls of the orbit.
-
Le Fort fractures.
-
Mandibular fractures.
