
Pathophysiology
Most sternal fractures are caused by blunt anterior chest trauma, although stress fractures have been noted in golfers, weight lifters, and other participants in noncontact sports. Insufficiency fractures caused by abnormally decreased bone density or weakened bone can occur spontaneously in patients with osteoporosis or osteopenia (particularly in older persons, especially women), those receiving long-term corticosteroid therapy, and those with severe thoracic kyphosis. Cardiopulmonary resuscitation commonly results in rib and sternal fractures. [1]
Fractures usually occur at the body or the manubrium. In one study of 79 patients with sternal fracture, 13 (16.5%) had a fracture of the manubrium, 10 caused by seat-belt injury. In 3 cases, stabilization was performed, and follow-up showed sufficient consolidation without complications. [2]
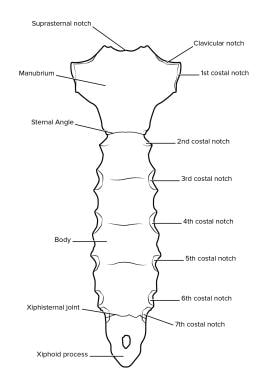
(Surface anatomy of the sternum is shown in the illustration below.)
Epidemiology
Sternal fractures are predominantly associated with deceleration injuries and blunt anterior chest trauma (incidence of 3-6.8% in motor vehicle collisions). Motor vehicle collisions account for 60-90% of sternal fractures. [3]
Many of these injuries occur in older vehicles in which a seat belt is used but no airbag deploys. [4] Those who are unrestrained generally sustain injury from ejection from the vehicle or impact with the steering wheel or dashboard. The occurrence of sternal fracture has tripled with the use of vehicular shoulder restraints, likely secondary to deceleration forces concentrated directly to the sternum; however, the overall severity of the injuries has decreased. [5] Effects of airbags on the incidence of sternal fractures are not fully known, although the literature suggests a decreased incidence when these are deployed.
Direct impact sports, falls, vehicle-to-pedestrian accidents, and assaults account for most of the rest of sternal fractures. Spontaneous fractures and stress fractures are rare.
Sternal fractures are slightly more common in females than in males, possibly because of shoulder restraint positioning; however, the difference is small. Sternal fractures occur more commonly in patients older than 50 years, possibly because of a weaker or inelastic bony thorax. [6] Because of the elasticity of their chest walls, children less commonly have sternal fractures; however, when present, the underlying injuries may be more severe. [7, 8, 9, 10]
Because of the lack of substantial change in size or shape of the sternum between ages 30 and 100 years, the increased incidence of sternal fracture in the elderly may be the result of cortical thickness or bone mineral density changes in the sternum, as opposed to changes in morphology. [4]
Prognosis
The prognosis is excellent for isolated sternal fractures. Most patients recover completely over a period of several weeks. In the absence of other injuries or severe pain, patients with isolated sternal fractures do not need admission to hospital. [11] In rare cases of nonunion and chronic sternal pain, surgical fixation can be considered.
Morbidity/mortality
The mortality rate from isolated sternal fracture is extremely low. Mortality associated with sternal fracture is 0.7%. Death and morbidity are related almost entirely to associated injuries, such as aortic disruption, cardiac contusion, and pulmonary contusion, or to unrelated injuries to the abdomen or head sustained in the accident, with reported mortality of 25-45%. [11]
Complications
Complications may arise from associated injuries. During evaluation of these patients, carefully assess for cardiac, pulmonary, mediastinal, and thoracic spine injuries, as well as associated injuries unrelated to chest trauma. [12]
Chest pain after injury can persist for 8 to 12 weeks. Pain on inspiration can result in atelectasis, pneumonia, and other pulmonary complications. [13]
Elderly patients may experience prolonged recovery because of pain and osteoporotic bone. These patients should join a physical therapy program to regain their strength and muscle mass. [13]
Cardiac contusion is much less common than once thought; its incidence ranges from 6% to 18%, based on severity of trauma.
Traumatic aortic injury occurs in fewer than 2% of sternal fractures, a rate similar to that in patients with blunt chest trauma without sternal fracture.
Nonunion of sternal fractures is very rare. Painful pseudoarthroses occur when a false joint develops secondary to failed union of a fracture and may require delayed surgical repair. Similarly, overlap deformities may require delayed surgical repair.
A posttraumatic mediastinal abscess is very uncommon. Risk factors include the presence of a large hematoma, intravenous drug abuse, and another source of a staphylococcal infection. Treatment is open debridement.
-
Lateral radiograph shows a complete displaced fracture of the sternum (arrow) (same patient as in image above).
-
Illustration shows posterior surface of the sternum.
-
Supine frontal radiograph after significant blunt trauma to the anterior chest wall shows marked mediastinal widening. (Also see next image.)
Tables

What would you like to print?
- Vertebral Fractures and Myeloma: Link Is Questionable
- Christmas: A Time for Love and... Penile Fractures
- Hip Fractures in Patients With Dementia: To Operate or Not?
-
 American Geriatrics Society (AGS) 2025 Annual Scientific Meeting
American Geriatrics Society (AGS) 2025 Annual Scientific Meeting
- Transcatheter Aortic Valve Replacement Beyond Severe Aortic Stenosis
-
Apr 25, 2025 This Week in Cardiology Podcast




