Practice Essentials
Hyperkalemia is defined as a serum potassium concentration greater than approximately 5.0-5.5 mEq/L in adults; the range in infants and children is age-dependent. Levels higher than 7 mEq/L can lead to significant hemodynamic and neurologic consequences; levels exceeding 8.5 mEq/L can cause respiratory paralysis or cardiac arrest and can quickly be fatal. [1] See the image below.
Signs and symptoms
Many individuals with hyperkalemia are asymptomatic. When present, symptoms are nonspecific and predominantly related to muscular or cardiac function. Weakness and fatigue are the most common complaints. Occasionally, patients may report the following:
-
Frank muscle paralysis
-
Dyspnea
-
Palpitations
-
Chest pain
-
Nausea or vomiting
-
Paresthesias
In general, the results of the physical examination alone do not alert the physician to the diagnosis of hyperkalemia, except when severe bradycardia is present or muscle tenderness accompanies muscle weakness, suggesting rhabdomyolysis. Examination findings in patients with hyperkalemia include the following:
-
Vital signs usually normal, except occasionally in bradycardia due to heart block or tachypnea due to respiratory muscle weakness
-
Muscle weakness and flaccid paralysis
-
Depressed or absent deep tendon reflexes
When hyperkalemia is discovered, investigate potential pathophysiologic mechanisms. Hyperkalemia can result from any of the following, which often occur in combination:
-
Excessive intake
-
Decreased excretion
-
A shift of potassium from the intracellular to the extracellular space
See Presentation for more detail.
Diagnosis
In a patient who does not have a predisposition to hyperkalemia, repeat the blood test before taking any actions to bring down the potassium level, unless ECG changes are present. Other tests include the following:
-
ECG
-
Urine potassium, sodium, and osmolality
-
Complete blood count (CBC)
-
Metabolic profile
If the BUN and serum creatinine levels suggest kidney insufficiency, using the MDRD or CKD-EPI equation to determine the estimated glomerular filtration rate (eGFR) is recommended. [2] Chronic kidney disease alone generally will not cause hyperkalemia until the eGFR is less than 20-25 mL/min.
Depending on the clinical findings and the results of the above laboratory work, the following may be indicated:
-
Glucose level - In patients with known or suspected diabetes mellitus
-
Digoxin level - If the patient is on a digitalis medication
-
Arterial or venous blood gas - If acidosis is suspected
-
Urinalysis - If signs of kidney insufficiency without an already known cause are present (to look for evidence of glomerulonephritis)
-
Serum cortisol and aldosterone levels - To check for mineralocorticoid deficiency when other causes are eliminated
-
Serum uric acid and phosphorus tests - For tumor lysis syndrome
-
Serum creatinine phosphokinase (CPK) and calcium measurements - For rhabdomyolysis
-
Urine myoglobin test - For crush injury or rhabdomyolysis; suspect if urinalysis reveals blood in the urine but no red blood cells are seen on urine microscopy
Electrocardiogram
-
Vital for assessing the physiologic significance of the hyperkalemia
-
ECG findings generally correlate with the potassium level, but potentially life-threatening arrhythmias can occur without warning at almost any level of hyperkalemia
-
In patients with organic heart disease and an abnormal baseline ECG, bradycardia may be the only new ECG abnormality
-
ECG changes have a sequential progression, which roughly correlate with the potassium level, but with the caveats mentioned above [3]
Early ECG changes of hyperkalemia, typically seen at a serum potassium level of 5.5-6.5 mEq/L, include the following:
-
Tall, peaked T waves with a narrow base, best seen in precordial leads [4]
-
Shortened QT interval
-
ST-segment depression
At a serum potassium level of 6.5-8.0 mEq/L, the ECG typically shows the following:
-
Peaked T waves
-
Prolonged PR interval
-
Decreased or disappearing P wave
-
Widening of the QRS
-
Amplified R wave
At a serum potassium level higher than 8.0 mEq/L, the ECG shows the following:
-
Absence of P waves
-
Progressive QRS widening
-
Intraventricular/fascicular/bundle branch blocks
The progressively widened QRS eventually merges with the T wave, forming a sine wave pattern. Ventricular fibrillation or asystole follows.
See Workup for more detail.
Management
The aggressiveness of therapy is directly related to the rapidity with which hyperkalemia has developed, the absolute level of hyperkalemia, and the evidence of toxicity. The faster the rise of potassium, the higher the level, and the stronger the evidence of cardiotoxicity, the more aggressive therapy should be.
If the patient has only a moderate elevation in potassium level and no ECG abnormalities, treatment is as follows:
-
Increase potassium excretion using a cation exchange resin or diuretics
-
Correct the source of excess potassium (eg, increased intake or inhibited excretion)
In patients with severe hyperkalemia, treatment is as follows:
-
IV calcium to ameliorate cardiac toxicity, if present
-
Identify and remove sources of potassium intake
-
IV glucose and insulin infusion to enhance potassium uptake by cells
-
Correct severe metabolic acidosis with sodium bicarbonate
-
Consider beta-adrenergic agonist therapy (eg, nebulized albuterol, 10 mg, administered by a respiratory therapist); preferred over alkali therapy in patients with kidney failure
-
Increase potassium excretion by administering diuretics or gastrointestinal cation-exchange medications
-
Emergency dialysis for patients with potentially lethal hyperkalemia that is unresponsive to more conservative measures or with complete renal failure
Medications for increasing potassium excretion include the following:
-
IV saline and a loop diuretic (eg, furosemide), in patients with normal kidney function
-
An aldosterone analogue, such as 9-alpha fluorohydrocortisone acetate (Florinef), in patients with hyporeninemia or hypoaldosteronism or solid organ transplant patients with chronic hyperkalemia from calcineurin inhibitor use
-
Potassiuim binders include cation exchange resins such as sodium polystyrene sulfonate (SPS; Kayexalate), patiromer, or sodium zirconium cyclosilicate (Lokelma); an SPS retention enema may be used for hyperkalemic emergencies, oral products have slower onset of action, but may be considered for patients with advanced kidney failure who are not yet on dialysis or are transplant candidates
Surgery
Surgery is typically unnecessary, but the following scenarios may involve surgical intervention:
-
Patients with metabolic acidosis and consequent hyperkalemia due to ischemic gut: Exploration required
-
Patients with hyperkalemia due to rhabdomyolysis: Surgical decompression of swollen ischemic muscle compartments may be needed
-
Patients without end-stage renal disease who require hemodialysis for control of hyperkalemia: Placement of a hemodialysis catheter for emergent dialysis needed [5]
See Treatment and Medication for more detail.
Background
Hyperkalemia is defined as a serum potassium concentration higher than the upper limit of the normal range; the range in infants and children is age-dependent, whereas the range for adults is approximately 3.5-5.5 mEq/L. The upper limit may be considerably higher in young or premature infants, as high as 6.5 mEq/L. [6] Degrees of hyperkalemia are generally defined as follows (however, note that not all sources agree on these levels) [7] :
-
5.5-6.0 mEq/L – Mild
-
6.1-7.0 mEq/L – Moderate
-
≥7.0 mEq/L – Severe
Levels higher than 7 mEq/L can lead to significant hemodynamic and neurologic consequences. Levels exceeding 8.5 mEq/L can cause respiratory paralysis or cardiac arrest and can quickly be fatal.
Because of a paucity of distinctive signs and symptoms, hyperkalemia can be difficult to diagnose. Indeed, it is frequently discovered as an incidental laboratory finding. The physician must be quick to consider hyperkalemia in patients who are at risk for this disease process. (See Etiology.) However, any single laboratory study demonstrating hyperkalemia must be repeated to confirm the diagnosis, especially if the patient has no changes on electrocardiography (ECG).
Because hyperkalemia can lead to sudden death from cardiac arrhythmias, any suggestion of hyperkalemia requires an immediate ECG to ascertain whether ECG signs of electrolyte imbalance are present. Continuous ECG monitoring is essential if hyperkalemia is confirmed. Other testing is directed toward uncovering the condition or conditions that led to the hyperkalemia (see Workup).
The aggressiveness of therapy for hyperkalemia is directly related to the rapidity with which the condition has developed, the absolute level of serum potassium, and the evidence of toxicity. The faster the rise of the potassium level, the higher it has reached, and the greater the evidence of cardiotoxicity, the more aggressive therapy should be.
In severe cases, treatment focuses on immediate stabilization of the myocardial cell membrane, rapid shifting of potassium to the intracellular space, and total body potassium elimination. In addition, all sources of exogenous potassium should be immediately discontinued. (See Treatment.)
Pathophysiology
Potassium is the primary intracellular cation; 95-98% of the total body potassium is found in the intracellular space, primarily in muscle. Total body potassium stores amount to approximately 50 mEq/kg (3500 mEq in a 70-kg person).
Normal homeostatic mechanisms precisely maintain the serum potassium level within a narrow range (3.5-5.0 mEq/L). The primary mechanisms for maintaining this balance are the buffering of extracellular potassium against a large intracellular potassium pool (via the sodium-potassium pump), which provides minute-to-minute control, and urinary excretion of potassium, which determines total body potassium balance.
Potassium is obtained through the diet. Common potassium-rich foods include meats, beans, tomatoes, potatoes, and fruits such as bananas. Gastrointestinal (GI) absorption is complete, resulting in daily excess intake of about 1 mEq/kg (60-100 mEq).
Under normal conditions, approximately 90% of potassium excretion occurs in the urine, with less than 10% excreted through sweat or stool. Within the kidneys, potassium excretion occurs mostly in the principal cells of the cortical collecting duct (CCD). Urinary potassium excretion depends on adequate luminal sodium delivery to the distal convoluted tubule (DCT) and the CCD, as well as the effect of aldosterone and other adrenal corticosteroids with mineralocorticoid activity.
Renal factors in potassium homeostasis
Sodium reabsorption through epithelial sodium channels (ENaC) located on the apical membrane of cortical collecting tubule cells is driven by aldosterone and generates a negative electrical potential in the tubular lumen, driving the secretion of potassium at this site through the renal outer medullary potassium (ROMK) channels. Aldosterone also regulates sodium transport in the thick ascending limb of the loop of Henle, the DCT, and the connecting tubule.
A family of signaling molecules, the WNK (with no K [lysine]) kinases, plays a critical role in the regulation of sodium and potassium transport in the distal nephron. [8] The WNK kinases are suspected of playing a role in the pathogenesis of several forms of hypertension. [5, 9]
WNK1 and WNK4 regulate the expression and function of the NaCl cotransporter and ROMK in the distal tubule. Increased WNK4 activity results in decreased NaCl cotransporter expression, permitting greater delivery of sodium to the cortical collecting tubule, thus facilitating potassium secretion. Conversely, lesser WNK4 activity results in increased NaCl cotransporter expression, diminishing distal sodium delivery, thus limiting cortical collecting tubule potassium secretion. [10, 11]
Renal potassium excretion is increased by the following:
-
Aldosterone
-
WNK1 and WNK4
-
High sodium delivery to the distal tubule (eg, diuretics)
-
High urine flow (eg, osmotic diuresis)
-
High serum potassium level
-
Delivery of negatively charged ions to the distal tubule (eg, bicarbonate)
Renal potassium excretion is decreased by the following:
-
Absence, or very low levels, of aldosterone
-
WNK1 and WNK4 mutations
-
Low sodium delivery to the distal tubule
-
Low urine flow
-
Low serum potassium level
Kidneys adapt to acute and chronic alterations in potassium intake. When potassium intake is chronically high, potassium excretion also is increased. Even in the absence of potassium intake, however, obligatory renal losses amount to 10-15 mEq/day. Thus, chronic losses occur in the absence of any ingested potassium.
In chronic kidney disease, renal adaptive mechanisms allow the kidneys to maintain potassium homeostasis until the glomerular filtration rate (GFR) decreases to less than 15-20 mL/min. Additionally, in the presence of kidney failure, the proportion of potassium excreted through the gut is thought to increase, though evidence for this compensatory mechanism has been elusive.
The colon is the major site of gut regulation of potassium excretion. Therefore, potassium levels can remain relatively normal under stable conditions, even with advanced renal insufficiency. However, as renal function worsens, the kidneys may not be capable of handling an acute potassium load. An excess of only 100-200 mEq will increase the serum potassium concentration by about 1 mEq/L. [12]
Potassium distribution and serum potassium levels
Potassium is predominantly an intracellular cation; thus, serum potassium levels do not always accurately reflect total body potassium stores. Serum potassium levels are determined by the shift of potassium between intracellular and extracellular fluid compartments, as well as by total-body potassium homeostasis.
Several factors regulate the distribution of potassium between the intracellular and extracellular spaces, including glucoregulatory hormones, adrenergic stimuli, and pH. Insulin enhances potassium entry into cells, whereas glucagon impairs it. Beta-adrenergic agonists enhance potassium entry into cells, whereas beta-blockers and alpha-adrenergic agonists inhibit it.
Alkalosis enhances potassium entry into cells. Acidosis causes a shift of potassium from intracellular space into extracellular space. Inorganic or mineral acid acidoses are more likely to cause a shift of potassium out of the cells than organic acidosis is.
In addition, an acute increase in osmolality, such as may result from hyperglycemia, causes potassium to exit from cells. Acute cell-tissue breakdown (eg, hemolysis or rhabdomyolysis) releases potassium into the extracellular space.
The 2 sets of regulatory factors—those that regulate total-body homeostasis and those that regulate distribution of potassium between intracellular and extracellular spaces—meld to create smooth control of potassium levels throughout the day. Thus, serum concentrations can remain stable even in the face of acute intake or loss of potassium.
For example, although a high-potassium meal might contain enough potassium to raise the serum potassium acutely to lethal levels if the potassium remained in the extracellular space, Na+ -K+ -ATPase rapidly takes up the potassium into cells, thus preventing the development of hyperkalemia. Adrenergic stimulation and insulin are important in maintaining the activity of Na+ -K+ -ATPase. The excess potassium then can be excreted by the kidneys, allowing serum potassium levels to return to normal.
Recent studies point toward a gastrointestinal-renal signal that is aldosterone-independent and causes enhanced renal potassium excretion after a meal. The mechanisms have not been fully determined. [13]
This integrated regulatory process is manifested in the diurnal rhythm for renal potassium excretion. The highest excretion occurs at midday, approximately 18 hours after peak potassium ingestion at the evening meal. [14]
Pathogenetic mechanisms
Hyperkalemia can result from any of the following:
-
Excessive intake of potassium
-
Decreased excretion of potassium
-
A shift of potassium from the intracellular to the extracellular space
In many cases a combination of these factors is involved. For example, a person with a GFR of less than 45 mL/min who consistently eats large amounts of high-potassium foods and is taking a medication that blocks the rennin-angiotensin-aldosterone system is at very high risk for hyperkalemia due to limitations in renal excretion of potassium in the face of high intake.
A person with diabetes mellitus who has hyporeninemic hypoaldosteronism associated with diabetic nephropathy is at high risk for hyperkalemia due to a diminished ability to shift potassium into the intracellular space (insulin deficiency) and impaired renal excretion (aldosterone deficiency). A third circumstance is acute kidney injury from rhabdomyolysis or tumor lysis syndrome, in which hyperkalemia results from impaired renal excretion in addition to the release of large amounts of potassium from intracellular to extracellular fluid compartments.
Excessive intake
Excessive potassium intake alone is a very uncommon cause of hyperkalemia in anyone with an estimated GFR higher than 60 mL/min. The mechanisms for shifting potassium intracellularly and for renal excretion allow a person with normal potassium homeostatic mechanisms to ingest very high quantities of potassium. Even parenteral administration of as much as 60 mEq/hr for several hours creates only a minimal increase in serum potassium concentration in healthy individuals.
The most common source of increased potassium intake is intravenous (IV) or oral potassium supplementation. Packed red blood cells (PRBCs) may also carry high concentrations of potassium that can lead to hyperkalemia during PRBC transfusion. [15]
Decreased excretion
Decreased excretion of potassium, especially when coupled with excessive intake, is the most common cause of hyperkalemia. The most common causes of decreased renal potassium excretion include the following:
-
Kidney failure (most common) [16]
-
Reduced aldosterone production
-
Primary adrenal disease (eg, Addison disease or salt-wasting forms of congenital adrenal hyperplasia)
-
Hyporeninemic hypoaldosteronism or renal tubular disease (pseudohypoaldosteronism I [23] or II)
Shift from intracellular to extracellular space
A number of factors can influence the shift of potassium from the intracellular to the extracellular space (see table below). By itself, this mechanism is a relatively uncommon cause of hyperkalemia, but it can exacerbate hyperkalemia produced by high intake or impaired renal excretion of potassium. A common scenario is that insulin deficiency or acute acidosis produces mild-to-moderate impairment of intracellular shifting of potassium.
Table. Selected Factors Affecting Plasma Potassium (Open Table in a new window)
Factor |
Effect on Plasma K+ |
Mechanism |
Aldosterone |
Decrease |
Increases sodium resorption, and increases K+ excretion |
Insulin |
Decrease |
Stimulates K+ entry into cells by increasing sodium efflux (energy-dependent process) |
Beta-adrenergic agents |
Decrease |
Increases skeletal muscle uptake of K+ |
Alpha-adrenergic agents |
Increase |
Impairs cellular K+ uptake |
Acidosis (decreased pH) |
Increase |
Impairs cellular K+ uptake |
Alkalosis (increased pH) |
Decrease |
Enhances cellular K+ uptake |
Cell damage |
Increase |
Intracellular K+ release |
Succinylcholine |
Increase |
Cell membrane depolarization |
Clinical situations in which this mechanism is the major cause of hyperkalemia include the following:
-
Hyperosmolality
-
Tissue breakdown (eg, rhabdomyolysis, tumor lysis syndrome, or massive hemolysis)
-
Propofol (“propofol infusion syndrome”) [24]
-
Toxins (digitalis intoxication or fluoride intoxication)
-
Beta-adrenergic blockade
-
Strenuous or prolonged exercise
-
Malignant hyperthermia
-
Hyperkalemic periodic paralysis
Hyperkalemia may also be caused by IV administration of epsilon aminocaproic acid (EACA), a synthetic amino acid. EACA has been found to cause hyperkalemia in studies conducted in dogs. The mechanism of action is presumed to be a structural similarity between EACA and arginine and lysine. These latter amino acids enter the muscle cell in exchange for potassium, thereby leading to an increase in extracellular potassium. [28, 29]
Cardiac and skeletal muscle effects
High levels of potassium cause abnormal heart and skeletal muscle function by lowering cell-resting action potential and preventing repolarization, leading to muscle paralysis. Classic ECG findings begin with tenting of the T wave, followed by lengthening and eventual disappearance of the P wave and widening of the QRS complex. [30] However, varying degrees of heart block are also common.
Just before the heart stops, the QRS and T wave merge to form a sinusoidal wave.
Etiology
Hyperkalemia can result from increased potassium intake, decreased potassium excretion, or a shift of potassium from the intracellular to the extracellular space. The most common causes involve decreased excretion. Alone, excessive intake or an extracellular shift is distinctly uncommon. Often, several disorders are present simultaneously.
Increased potassium intake
Alone, increased intake of potassium is a rare cause of hyperkalemia, because the mechanisms for renal excretion and intracellular disposition are very efficient. In general, a relatively high potassium intake contributes to hyperkalemia in individuals who have impaired renal excretion or intracellular-to-extracellular shift.
Increased intake may result from the following:
-
High-potassium, low-sodium diets
-
Ingestion of potassium supplements – Ingested amounts would have to be massive to be the sole cause of hyperkalemia, but even relatively small amounts can produce hyperkalemia in a patient with impaired renal excretion
-
High concentrations of potassium in IV fluid preparations (eg, total parenteral nutrition formulas)
-
Dietary salt substitutes – Several “no-salt” or “low-salt” substitutes contain about 10-12 mEq of potassium per gram and can be dangerous, especially with diminished kidney function
-
Penicillin G potassium therapy
-
Packed red blood cell transfusion (risk peaks at 2-3 weeks of cell storage)
-
Cardioplegia solutions – These contain 20-30 mmol/L of potassium chloride
Decreased potassium excretion
Almost all patients who present with persistent hyperkalemia have impaired renal excretion of potassium. Mild degrees of renal failure generally do not result in resting hyperkalemia, because of compensation by adaptive mechanisms in the kidneys and GI tract. However, once the GFR falls below 15-20 mL/min, significant hyperkalemia can occur, even in the absence of an abnormally large potassium load. The simple lack of nephron mass prevents normal potassium homeostasis.
Other mechanisms, such as drug effects or renal tubular acidosis, can decrease renal potassium excretion and cause hyperkalemia even in individuals with normal or only mildly decreased kidney function. Two other causes of decreased excretion of potassium are reduced distal sodium delivery and reduced tubular fluid flow rate.
Medications that can decrease potassium excretion include the following:
-
Potassium-sparing diuretics (eg, spironolactone, triamterene, amiloride)
-
NSAIDs
-
ACE inhibitors
-
Angiotensin-receptor blockers (ARBs)
-
Cyclosporine or tacrolimus
-
Pentamidine
-
Trimethoprim-sulfamethoxazole
-
Mineralocorticoid receptor antagonists (MRAs)
-
Heparin
-
Ketoconazole
-
Metyrapone
-
Herbs
In a study of 396 consecutive patients with heart failure who were taking renin-angiotensin-aldosterone system inhibitors (RAASi), 26% developed hyperkalemia of 5.5 mmol/L or greater and 12% developed hyperkalemia of 6.0 mmol/L or greater, over mean follow-up of 6.9 years. Independent risk factors for hyperkalemia included diabetes mellitus (odds ratio [OR] = 1.80, 95% CI = 1.03-3.19) and elevated baseline creatinine (OR = 2.37, 95% CI = 2.37-3.85). [31]
Initial analysis of data on 9222 outpatients in a European heart failure registry showed that hyperkalemia was independently associated with higher mortality. After adjusting for RAASi discontinuation, however, hyperkalemia was no longer associated with mortality, suggesting that hyperkalemia may be a risk marker for RAASi discontinuation rather than a risk factor for worse outcomes. [32]
Disorders that can cause type IV renal tubular acidosis, resulting in hyperkalemia, include the following:
-
Diabetes mellitus
-
Sickle cell disease or trait
-
Lower urinary tract obstruction
-
Adrenal insufficiency
-
Primary Addison syndrome due to autoimmune disease, tuberculosis, or infarct
-
Enzyme deficiencies
-
Genetic disorders (see below)
Shift of potassium into extracellular space
Like increased intake, this is rarely the sole cause of hyperkalemia, because the mechanisms for renal excretion are very efficient. However, the inability to transport potassium intracellularly exacerbates hyperkalemia in individuals who have impaired renal excretion.
Factors that can shift potassium into the extracellular space include the following:
-
Metabolic acidosis
-
Acute tubular necrosis
-
Electrical burns
-
Thermal burns
-
Cell depolarization
-
Head trauma
-
Digitalis toxicity
-
Fluoride toxicity [35]
-
Cyclosporine [36]
-
Methotrexate [37]
-
Propofol infusion syndrome
-
Rhabdomyolysis
-
Tumor lysis syndrome
-
Succinylcholine [26]
Hypertonicity may lead to hyperkalemia by the following 2 mechanisms:
-
Loss of intracellular water, resulting in an increased intracellular potassium concentration, favoring a gradient for potassium to move out of the cells
-
As water exits the cells, “solvent drag,” which sweeps potassium along
The most common cause of hyperosmolality is hyperglycemia in uncontrolled diabetes mellitus. Other conditions with hypertonicity are hypernatremia, hypertonic mannitol, and high-osmolarity contrast media..
Aldosterone deficiency is somewhat controversial as a cause of hyperkalemia. There is some evidence that long-term aldosterone deficiency impairs cell potassium uptake.
Toad venom, which is used in traditional Chinese medicine and in folk medicine in southeastern Asia, contains cardiac glycosides whose structure and biochemical activity are similar to those of digitalis. These cause hyperkalemia by binding to the alpha subunit of Na+ -K+ -ATPase and thus inhibiting reuptake of potassium from the extracellular space. [38]
Toad venom is prepared from dried secretions, typically from the Asiatic toad (Bufo gargarizans). In addition being an ingredient in Chinese medications (eg, Chan Su, Lu-Shen Wan), toad venom has also turned up in purported aphrodisiacs. Digoxin Fab fragments have been used to treat toad venom poisoning. [39]
Genetic disorders
Genetic disorders that can result in hyperkalemia include the following:
-
Glomerulopathy with fibronectin deposits (GFND)
-
Congenital hypoaldosteronism
-
Pseudohypoaldosteronism
-
Disorders of chloride homeostasis
-
Nephronophthisis
-
Hyperkalemic periodic paralysis (HYPP)
Glomerulopathy with fibronectin deposits
GFND is a genetically heterogeneous autosomal dominant disorder which manifests as proteinuria, hypertension, type IV renal tubular acidosis. It eventually leads to end-stage renal failure, in the second to fifth decade of life. Type 1 GFND maps to chromosome 1q32, but the gene is unknown at this time. Type 2 GFND is caused by mutations in the FN1 gene located on chromosome 2q34.
Disorders of steroid metabolism and mineralocorticoid receptors
21-hydroxylase deficiency in its classic form and aldosterone synthase deficiency result in hyperkalemia due to low aldosterone levels. 11-Beta hydroxylase deficiency, 3-beta hydroxysteroid dehydrogenase deficiency, and 17 alpha-hydroxylase/17,20-lyase deficiency are generally not characterized by the development of hyperkalemia.
Congenital hypoaldosteronism
Congenital hypoaldosteronism is caused by mutations in the CYP11B2 gene, which encodes the type II corticosterone methyloxidase enzyme. It is inherited in an autosomal recessive manner. Patients with this disorder have decreased aldosterone and salt wasting. They will have an increased serum ratio of 18-hydroxycorticosterone to aldosterone.
Pseudohypoaldosteronism
Type I pseudohypoaldosteronism (PHAI) can be caused by an inactivating mutation of 1 of 3 encoding subunits of the epithelial sodium channel (SCNN1A, SCNN1G, or SCNN1B). PHAI is inherited in an autosomal recessive manner. These mutations result in impaired potassium secretion due to impaired sodium reabsorption in the distal tubule. [41]
PHAI tends to be most severe in the neonatal period, causing renal salt wasting and respiratory tract infections. Sweat, stool, and saliva have high sodium concentrations. Sometimes this disorder can be mistaken for cystic fibrosis.
Another form of PHAI is caused by mutations in the NR3C2 gene and is inherited in an autosomal dominant manner. Patients with this disorder may present in the neonatal period with renal salt wasting and hyperkalemic acidosis similar to those seen in the autosomal recessive form. Patients with this form of PHAI generally improve with age and are typically asymptomatic in adulthood. [42]
Gordon syndrome, or pseudohypoaldosteronism type II (PHAII), characterized by hyperkalemia and hypertension, is caused by mutations in several genes. The following 5 loci are known to be associated with PHAII:
-
PHA2A has been mapped to chromosome 1q31-q42, but no gene is known at the present time
-
PHA2B is caused by mutations in the WNK4 gene on chromosome 17q21
-
PHA2C is caused by mutations in the WNK1 gene on chromosome 12p13
-
PHA2D is caused by mutations in the KLHL3 gene on chromosome5q31
-
PHA2E is caused by mutations in the CUL3 gene on chromosome 2q36
The genes causing this disorder code for protein kinases that are localized to the distal tubule and that regulate ion transport in this nephron segment. WNK4 appears to have several roles in regulating sodium, potassium, and chloride transport through transcellular and paracellular pathways. [43] Interestingly, PHAII from mutations in WNK1 is significantly less severe than PHAII from mutations in WNK4 or KLHL3, whereas PHAII from mutations in CUL3 is more severe. [44] All forms of PHII generally respond to treatment with thiazide diuretics.
Disorders of chloride homeostasis
Disorders of chloride homeostasis can also result in hyperkalemia. Isolated hyperchlorhidrosis is caused by mutations in the CA12 gene, and is inherited in an autosomal recessive manner. This disorder can cause excessive salt wasting in sweat, which can result in severe hyponatremic dehydration and hyperkalemia. [45]
Nephronophthisis
Nephronophthisis is characterized by enlargement of the kidneys, inflammatory portal fibrosis of the liver, and variable development of end-stage renal disease (ESRD). Patients with the infantile form of this disease generally reach ESRD before the age of 2 years. Patients with the juvenile form reach ESRD at a median age of 13 years. Patients with other forms of the disease have variable natural history.
Ultimately, this disorder causes a progressive interstitial fibrosis and tubulopathy. Routine laboratory evaluation will show increased creatinine and potassium.
Hyperkalemic periodic paralysis
HYPP is caused by mutations in the SCN4A gene and is inherited in an autosomal dominant manner. During attacks (which can be precipitated by administration of potassium), individuals with HYPP have flaccid generalized weakness and increased serum potassium levels. In addition, patients with HYPP can also have myotonia, which is not typically a feature of hypokalemic periodic paralysis (HOKPP). A number of similar disorders involving myotonia or muscular weakness are allelic to HYPP. [46]
Diabetes mellitus
Patients with diabetes constitute a unique high-risk group for hyperkalemia, in that they develop defects in all aspects of potassium metabolism. [17, 18] The typical healthy diabetic diet often is high in potassium and low in sodium. Diabetic persons frequently have underlying kidneyl disease and often develop hyporeninemic hypoaldosteronism (ie, decreased aldosterone secondary to suppressed renin levels), impairing renal excretion of potassium. [21, 22]
Many patients with diabetes are placed on ACE inhibitor or ARB therapy for treatment of hypertension or diabetic nephropathy, exacerbating the defect in potassium excretion. Finally, persons with diabetes have insulin deficiency or resistance to insulin action, limiting their ability to shift potassium intracellularly.
Epidemiology
United States statistics
Hyperkalemia, defined as a serum potassium concentration greater than 5.0–5.3 mEq/L, is rare in a general population of healthy individuals. A meta-analysis found a hyperkalemia prevalence of 6.3% among adults across 542 observational studies with varying diagnostic thresholds. The prevalence by hyperkalemia thresholds were 8% for > 5 mEq/L, 5.9% for ≥5.5 mEq/L and 1% for ≥6.0 mEq/L. Rates of hyperkalemia were highest in patients with end-stage kidney disease (21.5%), kidney transplants (21.8%), or acute kidney injury (24.3%). [47]
In hospitalized patients, the incidence of hyperkalemia has ranged from 1% to 10%, depending on how the condition is defined. In hospitalized patients, drugs are implicated in the development of hyperkalemia in as many as 75% of cases. Decreased kidney function, [16] genitourinary disease, cancer, severe diabetes, and polypharmacy may also predispose to hyperkalemia.
The incidence of hyperkalemia in the pediatric population is unknown, though the prevalence of hyperkalemia in extremely low birth weight premature infants can exceed 50%. [48] Hyperkalemia in pediatric patients is most commonly associated with kidney insufficiency, acidosis, and diseases that involve defects in mineralocorticoid, aldosterone, and insulin function. [23]
Military recruits, individuals with sickle cell traits, and people who abuse drugs are at risk for hyperkalemia because of acute rhabdomyolysis. These cases disproportionately occur in males, probably reflecting the higher muscle mass of males, though an underlying hormonal predisposition cannot be absolutely excluded.
Patients with diabetes mellitus are at increased risk for hyperkalemia. In one review of an unselected group of diabetes clinic patients, 15% (270 of 1764) had a serum potassium level higher than 5 mEq/L; however, fewer than 4% had levels higher than 5.4 mEq/L. [49] Clinical risk factors significant in predicting the occurrence of hyperkalemia included kidney insufficiency, duration of diabetes mellitus, age, glycosylated hemoglobin levels, and retinopathy—but not the serum glucose level or the drugs used for diabetes treatment.
Use of ACE inhibitors as a risk factor for hyperkalemia is a significant concern, particularly because the indications for these agents in high-risk populations are broad. In a 1998 study, 11% of patients at a Veterans Affairs general medicine outpatient clinic had hyperkalemia; risk factors included elevated blood urea nitrogen (BUN) and serum creatinine, severe diabetes mellitus, heart failure, peripheral vascular disease, and the use of a long-acting drug. Hyperkalemia occurred in less than 6% of patients with normal kidney function. [50]
As cardiovascular therapy has evolved, the growing population of patients with chronic heart failure also has come to constitute a high-risk group. The factors promoting the development of hyperkalemia in these patients include underlying kidney insufficiency due to poor cardiac output and reduced renal blood flow, as well as the high prevalence of diabetes mellitus in patients with heart failure and the growing use of ACE inhibitors, ARBs, aldosterone inhibitors (eg, spironolactone), and direct renin inhibitors (eg, aliskiren), alone and in combination. [21, 22, 51, 52, 53]
Initial studies examining the risk of hyperkalemia in patients with heart failure who were treated with aldosterone inhibitors revealed only a minor increase in hyperkalemia. However, later studies showed that as the treatment became more widespread, morbidity and mortality from hyperkalemia increased. [54]
International statistics
Hyperkalemia has been reported in less than 5% of the general population worldwide. Hospitalized patients in countries as diverse as England, Australia, and Israel experience hyperkalemia approximately 10% of the time. No racial differences in the incidence of hyperkalemia appear to exist.
As in the United States, risk factors include advanced age, significant prematurity, and the presence of kidney failure, diabetes mellitus, and heart failure. Additionally, one series documented an increased incidence of hyperkalemia with cancer and GI disease. [55] Polypharmacy, particularly the use of potassium supplements and potassium-sparing diuretics, in patients with underlying kidney insufficiency contributed to hyperkalemia in almost 50% of the cases.
Age-related demographics
Several series document the increasing tendency for hyperkalemia in patients at the extremes of life—that is, small premature infants and elderly people. Kidney insufficiency plays a significant role in both groups.
Studies in small premature infants indicate that the incidence of hyperkalemia is increased in infants with a lower GFR, as estimated on the basis of endogenous creatinine clearance. In these cases, hyperkalemia often occurs within the first 48 hours of life. Even full-term infants may have transient hyperkalemia and hyponatremia due to decreased responsiveness to aldosterone (PHAI). [23]
Several factors contribute to the increased propensity for elderly people to become hyperkalemic. Kidney function tends to deteriorate with age, even in relatively healthy individuals. The GFR decreases by approximately 1 mL/min each year in people older than 30 years. Renal blood flow also decreases. Oral intake declines, resulting in decreased urine flow rates. Plasma renin activity and aldosterone levels also tend to decrease with age, reducing the ability of the distal nephron to secrete potassium.
Elderly patients are more likely to be taking medications that could interfere with potassium secretion, such as NSAIDs, ACE inhibitors, and potassium-sparing diuretics. Elderly individuals who are bedridden often are placed on subcutaneous heparin, which can decrease aldosterone production.
Sex-related demographics
Men are significantly more prone to hyperkalemia than women are. This difference has been noted in several series and stands in contrast to the increased incidence of hypokalemia in women. The reasons for this discrepancy are unknown. However, neuromuscular disorders, including myotonic and muscular dystrophies and related disorders that can predispose patients to hyperkalemia with succinylcholine administration, are more prevalent in males. [56]
Prognosis
For patients with a defined and transient cause of hyperkalemia, the prognosis is excellent. With correction of the underlying causative condition, full resolution can be expected. However, patients who have ongoing risk factors for hyperkalemia are likely to experience recurrent episodes.
Sudden and rapid onset of hyperkalemia can be fatal. With slow or chronic increase in potassium levels, adaptation occurs via renal excretion, with fractional potassium excretion increasing by as much as 5-10 times the reference range.
Complications of hyperkalemia range from mild ECG changes to cardiac arrest. Weakness is common as well. The primary cause of morbidity and mortality is potassium’s effect on cardiac function. [57] The mortality can be as high as 67% if severe hyperkalemia is not treated rapidly. [54] Although a normal ECG does not rule out hyperkalemia, it is associated with a significantly lower risk for cardiac complications such as symptomatic bradycardia, ventricular dysrhythmia, cardiac arrest, or death. [58]
In hospitalized patients, hyperkalemia is an independent risk factor for death. In one series, 406 (1.4%) of 29,063 patients who were hospitalized developed hyperkalemia; 58 (14.3%) of the 406 died, with the risk increasing as the potassium level increased. [55]
Whereas 28% of patients with a serum potassium level above 7 mEq/L died, only 9% of those with a potassium level below 6.5 mEq/L died. [55] In 7 of the 58 deaths, the cause of death was directly attributable to hyperkalemia. Most cases resulting in death were complicated by renal failure. It is noteworthy that all of the patients who died of hyperkalemia had normal potassium levels within the 36 hours preceding death.
Interestingly, in a large study of individuals living in the community, serum potassium levels greater than 5.0 mEq/L correlated with increased mortality, although the mechanisms were not clear. [59]
-
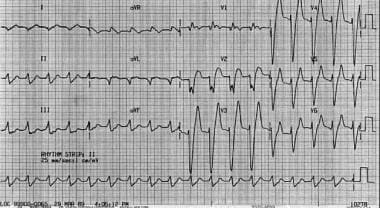
Widened QRS complexes in patient whose serum potassium level was 7.8 mEq/L.
-
ECG of patient with pretreatment potassium level of 7.8 mEq/L and widened QRS complexes after receiving 1 ampule of calcium chloride. Note narrowing of QRS complexes and reduction of T waves.
-
Hyperkalemia diagnosis and treatment flow chart.
-
Widened QRS complexes in hyperkalemia.
Tables
Factor |
Effect on Plasma K+ |
Mechanism |
Aldosterone |
Decrease |
Increases sodium resorption, and increases K+ excretion |
Insulin |
Decrease |
Stimulates K+ entry into cells by increasing sodium efflux (energy-dependent process) |
Beta-adrenergic agents |
Decrease |
Increases skeletal muscle uptake of K+ |
Alpha-adrenergic agents |
Increase |
Impairs cellular K+ uptake |
Acidosis (decreased pH) |
Increase |
Impairs cellular K+ uptake |
Alkalosis (increased pH) |
Decrease |
Enhances cellular K+ uptake |
Cell damage |
Increase |
Intracellular K+ release |
Succinylcholine |
Increase |
Cell membrane depolarization |
