Practice Essentials
Immune thrombocytopenia (ITP) is a syndrome in which platelets become coated with autoantibodies to platelet membrane antigens, resulting in splenic sequestration and phagocytosis by mononuclear macrophages. The resulting shortened life span of platelets in the circulation, together with incomplete compensation by increased platelet production by bone marrow megakaryocytes, results in a decreased number of circulating platelets (thrombocytopenia; see the image below).
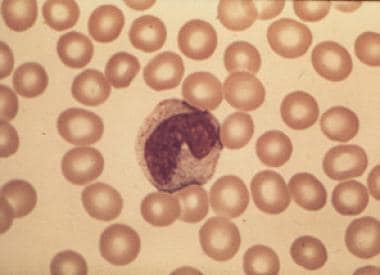 Peripheral blood smear from a patient with immune thrombocytopenia (ITP) shows a decreased number of platelets, a normal-appearing neutrophil, and normal-appearing erythrocytes. ITP is diagnosed by excluding other diseases; therefore, the absence of other findings from the peripheral smear is at least as important as the observed findings. This smear demonstrates the absence of immature leukocytes (as in leukemia) and fragmented erythrocytes (as in thrombotic thrombocytopenic purpura) and no clumps of platelets (as in pseudothrombocytopenia).
Peripheral blood smear from a patient with immune thrombocytopenia (ITP) shows a decreased number of platelets, a normal-appearing neutrophil, and normal-appearing erythrocytes. ITP is diagnosed by excluding other diseases; therefore, the absence of other findings from the peripheral smear is at least as important as the observed findings. This smear demonstrates the absence of immature leukocytes (as in leukemia) and fragmented erythrocytes (as in thrombotic thrombocytopenic purpura) and no clumps of platelets (as in pseudothrombocytopenia).
Signs and Symptoms
ITP manifests as a bleeding tendency, easy bruising (purpura), or extravasation of blood from capillaries into skin and mucous membranes (petechiae). Although most cases of acute ITP, particularly in children, are mild and self-limited, intracranial hemorrhage may occur when the platelet count drops below 10 × 109/L (< 10 × 103/µL); [1] this occurs in 0.5-1% of children, and half of these cases are fatal. [2]
ITP is a primary illness occurring in an otherwise healthy person. Signs of chronic disease, infection, wasting, or poor nutrition indicate that the patient has another illness. Splenomegaly excludes the diagnosis of ITP.
An initial impression of the severity of ITP is formed by examining the skin and mucous membranes, as follows:
-
Widespread petechiae and ecchymoses, oozing from a venipuncture site, gingival bleeding, and hemorrhagic bullae indicate that the patient is at risk for a serious bleeding complication.
-
If the patient's blood pressure was taken recently, petechiae may be observed under and distal to the area where the cuff was placed and inflated.
-
Suction-type electrocardiograph (ECG) leads may induce petechiae.
-
Petechiae over the ankles in ambulatory patients or on the back in bedridden ones suggest mild thrombocytopenia and a relatively low risk for a serious bleeding complication.
Findings suggestive of intracranial hemorrhage include the following:
-
Headache, blurred vision, somnolence, or loss of consciousness
-
Hypertension and bradycardia, which may be signs of increased intracranial pressure
-
On neurologic examination, any asymmetrical finding of recent onset
-
On fundoscopic examination, blurring of the optic disc margins or retinal hemorrhage
See Presentation for more detail.
Diagnosis
On complete blood cell count, isolated thrombocytopenia is the hallmark of ITP. Anemia and/or neutropenia may indicate other diseases. Findings on peripheral blood smear are as follows:
-
The morphology of red blood cells (RBCs) and leukocytes is normal
-
The morphology of platelets is typically normal, with varying numbers of large platelets
-
If most of the platelets are large, approximating the diameter of red blood cells, or if they lack granules or have an abnormal color, consider an inherited platelet disorder
Many children with acute ITP have an increased number of normal or atypical lymphocytes on the peripheral smear, reflecting a recent viral illness. Clumps of platelets on a peripheral smear prepared from ethylenediaminetetraacetic acid (EDTA)–anticoagulated blood are evidence of pseudothrombocytopenia. [3] This diagnosis is established if the platelet count is normal when repeated on a sample from heparin-anticoagulated or citrate-anticoagulated blood.
No single laboratory result or clinical finding establishes a diagnosis of ITP; it is a diagnosis of exclusion. The differential diagnosis includes such other causes of thrombocytopenia as leukemia, myelophthisic marrow infiltration, myelodysplasia, aplastic anemia, and adverse drug reactions. Pseudothrombocytopenia due to platelet clumping is also a diagnostic consideration.
Aspects of bone marrow aspiration and biopsy are as follows:
-
The value of bone marrow evaluation for a diagnosis of ITP is unresolved [4]
-
Biopsy in patients with ITP shows a normal-to-increased number of megakaryocytes in the absence of other significant abnormalities
-
In children, bone marrow examination is not required except in patients with atypical hematologic findings, such as immature cells on the peripheral smear or persistent neutropenia. [5]
-
In adults older than 60 years, biopsy is used to exclude myelodysplastic syndrome or leukemia
-
In adults whose treatment includes corticosteroids, a baseline pretreatment biopsy may prove useful for future reference, as corticosteroids can change marrow morphology
-
Biopsy is performed before splenectomy to evaluate for possible hypoplasia or fibrosis
-
Unresponsiveness to standard treatment after 6 months is an indication for bone marrow aspiration
See Workup for more detail.
Management
ITP has no cure, and relapses may occur years after seemingly successful medical or surgical management. [6] Most children with acute ITP do not require treatment, and the condition resolves spontaneously. [7, 8]
Treatment is as follows:
-
Corticosteroids remain the drugs of choice for the initial management of acute ITP
-
RhIG can induce immune hemolysis (immune hemolytic anemia) in Rh(D)-positive persons and should not be used when the hemoglobin concentration is less than 8 g/dL
-
Platelet transfusions may be required to control clinically significant bleeding but are not recommended for prophylaxis
-
Options in patients with corticosteroid dependence or unresponsiveness include thrombopoietin receptor agonists (TPO-RAs; ie, romiplostim, eltrombopag, avatrombopag), rituximab, or splenectomy
-
TPO-RAs may maintain platelet counts at safe levels in patients with chronic ITP refractory to splenectomy
Pregnant women require special consideration for delivery, as follows [18] :
-
If the platelet count is greater than 50 × 109/L (>50 × 103/µL), the risk of serious hemorrhage is low, but beginning oral prednisone a week before delivery is a reasonable precaution
-
If the platelet count is less than 50 × 109/L (50 × 103/µL) before delivery, treatment with oral prednisone and IVIG is recommended
-
Avoiding the use of IV RhIG in this situation until safety data are available is advisable
-
Rarely, splenectomy may be required to manage acute hemorrhage [19]
See Treatment and Medication for more detail.
For discussion of ITP in pregnancy, see Immune Thrombocytopenia and Pregnancy. For patient education information, see the Thrombocytopenia Directory
Background
Immune thrombocytopenia (ITP) was previously known as idiopathic thrombocytopenic purpura. The term "idiopathic" no longer applies, because the etiology is known: ITP is caused by a dysregulation of the immune system. The term "purpura" has been abandoned because it is misleading: almost one-third of patients with newly diagnosed ITP have no bleeding, despite their low platelet counts. [20]
Pathophysiology
In immune thrombocytopenia (ITP), an abnormal autoantibody, usually immunoglobulin G (IgG) with specificity for one or more platelet membrane glycoproteins, binds to circulating platelet membranes. [21, 22, 23]
Autoantibody-coated platelets induce Fc receptor-mediated phagocytosis by mononuclear macrophages, primarily but not exclusively in the spleen. [24] The spleen is the key organ in the pathophysiology of ITP, not only because platelet autoantibodies are formed in the white pulp, but also because mononuclear macrophages in the red pulp destroy immunoglobulin-coated platelets. [25]
Malik et al have identified cytotoxic CD8+ T cells as an antibody-independent mechanism of platelet destruction in chronic ITP. These researchers demonstrated that adults with chronic ITP have clonal expansion of terminally differentiated effector memory CD8+ T cells (TEMRA), compared with age-matched controls. TEMRAs form aggregates with autologous platelets, release interferon gamma, and trigger platelet activation and apoptosis via the T-cell receptor–mediated release of cytotoxic granules. [26]
If bone marrow megakaryocytes cannot increase production and maintain a normal number of circulating platelets, thrombocytopenia and purpura develop. Impaired thrombopoiesis is attributed to failure of a compensatory increase in thrombopoietin and megakaryocyte apoptosis.
Etiology
In children, most cases of immune thrombocytopenia (ITP) are acute, manifesting a few weeks after a viral illness. In adults, most cases of ITP are chronic, manifesting with an insidious onset, and occur in middle-aged women. These clinical presentations suggest that the triggering events may be different. However, in both children and adults, the cause of thrombocytopenia (destruction of antibody-coated platelets by mononuclear macrophages) appears to be similar.
Autoantibody stimulation
In chronic ITP, for unknown reasons, membrane glycoproteins (GPs) on the surface of platelets become immunogenic, stimulating the production of platelet autoantibodies. In acute ITP, the stimulus for autoantibody production is also unknown; platelet membrane cryptantigens may become exposed by the stress of infection, or pseudoantigens may be formed by the passive adsorption of pathogens on platelet surfaces
Autoantibody specificity
In persons with chronic ITP, approximately 75% of autoantibodies are directed against platelet GPIIb/IIIa or GPIb/IX GP complexes. Presumably, the remaining 25% are directed against other membrane epitopes, including GPV, GPIa/IIa, or GPIV
Role of the spleen
The spleen is the site of autoantibody production (white pulp); it is also the site of phagocytosis of autoantibody-coated platelets (red pulp). The slow passage of platelets through splenic sinusoids with a high local concentration of antibodies and Fc-gamma receptors on splenic macrophages lend to the uniqueness of the spleen as a site of platelet destruction. Low-affinity macrophage receptors, Fc gamma RIIA, and Fc gamma RIIIA bind immune-complexed IgG and are the key mediators of platelet clearance.
Platelet destruction
The mononuclear macrophage system of the spleen is responsible for removing platelets in ITP, as demonstrated by the fact that splenectomy results in prompt restoration of normal platelet counts in most patients with ITP. Platelets are sequestered and destroyed by mononuclear macrophages, which are neither reticular nor endothelial in origin. Therefore, the former designation of reticuloendothelial system is considered imprecise. Immune destruction of immunoglobulin-coated platelets is mediated by macrophage IgG Fc (Fc gamma RI, Fc gamma RII, and Fc gamma RIII) and complement receptors (CR1, CR3).
Epidemiology
United States
The annual incidence of immune thrombocytopenia (ITP) is estimated to be five cases per 100,000 children and two cases per 100,000 adults, [2] but those data are not from large population-based studies. Most cases of acute ITP, particularly in children, are mild and self-limited and may not receive medical attention. Therefore, estimated incidences of ITP are difficult to determine and are likely to understate the full extent of the disease. The age-adjusted prevalence of ITP in Maryland was reported as 9.5 per 100,000 persons by Segal and Powe. [27]
International
A French study reported an incidence of ITP of 2.9 cases per 100,000 person-years, with peaks in children and in those older than 60 years of age and a higher frequency of ITP in males in these subgroups. ITP showed seasonal variation, with a peak in winter and a nadir in summer. Persistence or chronicity occurred in 36% of children compared with 67% of adults. In adults, 18% of ITP cases were secondary, with malignancy the main cause. [28]
Mortality and morbidity
The primary cause of long-term morbidity and mortality in patients with immune thrombocytopenia (ITP) is hemorrhage. [29] Spontaneous or accidental trauma–induced intracranial hemorrhage is the most frequent cause of death in association with ITP. Most cases of intracranial hemorrhage occur in patients whose platelet counts are less than 10 × 109/L (< 10 × 103/µL). [1] This situation occurs in 0.5-1% of cases in children, and half of those are fatal. [2] In one study, 17% of children experienced a major hemorrhage. [30] The estimated frequency of intracranial hemorrhage in adults with ITP is 1.5%. [31]
Treatment-related morbidity may result from the need to maintain the platelet count in a safe range in patients with chronic treatment-resistant ITP. These patients may require a long-term course of corticosteroids, other immunosuppressive medications, or splenectomy, and thus may experience the complications of therapy with corticosteroids or splenectomy.
Sex- and Age-related Demographics
In children, ITP is more common in boys than in girls. [32] In middle-aged adults, women are affected more frequently than men. [2]
Children may develop ITP at any age, but the incidence peaks in children aged 1-6 years. [32] Adults may be affected at any age, but most cases are diagnosed in women aged 30-40 years.
Onset in a patient older than 60 years is uncommon, and a search for other causes of thrombocytopenia is warranted. The most likely causes in these persons are myelodysplastic syndromes, acute leukemia, and marrow infiltration (myelophthisis). Persons with ITP who are 70 years or older are at increased risk for spontaneous bleeding and treatment-related adverse events. [33]
Prognosis
Prognosis varies in children and adults.
Children
More than 80% of children with untreated immune thrombocytopenia (ITP) have a spontaneous recovery with completely normal platelet counts in 2-8 weeks. Fatal bleeding occurs in 0.9% upon initial presentation.
A systematic review and meta-analysis identified the following factors associated with higher risk of ITP in children becoming chronic [34] :
-
Female sex (odds ratio [OR] 1.17)
-
Age ≥11 years at presentation (OR 2.47)
-
No preceding infection or vaccination (OR 3.08)
-
Insidious onset (OR 11.27)
-
Platelet count ≥20 × 109/L at presentation (OR 2.15)
-
Presence of antinuclear antibodies (OR 2.87)
-
Treatment with methylprednisolone plus intravenous immunoglobulin (OR 2.67)
Factors associated with lower likelihood of developing chronic ITP were as follows:
-
Mucosal bleeding at diagnosis (OR 0.39)
-
Treatment with intravenous immunoglobulin alone (OR 0.71)
Adults
Approximately 60-90% of adults with ITP respond with an increased platelet count after treatment with prednisone or prednisone and IV RhIG or IVIG. Of those adults who do not maintain an increased platelet count and who require splenectomy, approximately two thirds have a sustained response and 10-15% have a partial response. [1, 35]
-
Peripheral blood smear from a patient with immune thrombocytopenia (ITP) shows a decreased number of platelets, a normal-appearing neutrophil, and normal-appearing erythrocytes. ITP is diagnosed by excluding other diseases; therefore, the absence of other findings from the peripheral smear is at least as important as the observed findings. This smear demonstrates the absence of immature leukocytes (as in leukemia) and fragmented erythrocytes (as in thrombotic thrombocytopenic purpura) and no clumps of platelets (as in pseudothrombocytopenia).
Tables
Grade |
Bleeding |
Management approach |
|---|---|---|
Grade 1 (minor) |
Minor bleeding, few petechiae (≤100 total) and/or ≤5 small bruises (≤3 cm in diameter), no mucosal bleeding |
Consent for observation |
Grade 2 (mild) |
Mild bleeding, many petechiae (>100 total) and/or >5 large bruises (>3 cm in diameter), no mucosal bleeding |
Consent for observation |
Grade 3 (moderate) |
Moderate bleeding, overt mucosal bleeding, troublesome lifestyle |
Intervention to reach grade 1 or 2 |
Grade 4 (severe) |
Severe bleeding, mucosal bleeding leading to decrease in Hb > 2 g/dL or suspected internal hemorrhage |
Intervention |
