Practice Essentials
Recognizing patients with severe acute pancreatitis as soon as possible is critical for achieving optimal outcomes. Management depends largely on severity. Medical treatment of mild acute pancreatitis is relatively straightforward. Treatment of severe acute pancreatitis involves intensive care. Surgical intervention (open or minimally invasive) is indicated in selected cases.
Signs and symptoms
Symptoms of acute pancreatitis include the following:
-
Abdominal pain (cardinal symptom): Characteristically dull, boring, and steady; usually sudden in onset and gradually becoming more severe until reaching a constant ache; most often located in the upper abdomen and may radiate directly through to the back
-
Nausea and vomiting, sometimes with anorexia
-
Diarrhea
Patients may have a history of the following:
-
Recent operative or other invasive procedures
-
Family history of hypertriglyceridemia
-
Previous biliary colic and binge alcohol consumption (major causes of acute pancreatitis)
The following physical findings may be noted, varying with the severity of the disease:
-
Fever (76%) and tachycardia (65%); hypotension
-
Abdominal tenderness, muscular guarding (68%), and distention (65%); diminished or absent bowel sounds
-
Jaundice (28%)
-
Dyspnea (10%); tachypnea; basilar rales, especially in the left lung
-
In severe cases, hemodynamic instability (10%) and hematemesis or melena (5%); pale, diaphoretic, and listless appearance
-
Occasionally, extremity muscular spasms secondary to hypocalcemia
The following uncommon physical findings are associated with severe necrotizing pancreatitis:
-
Cullen sign (bluish discoloration around the umbilicus resulting from hemoperitoneum)
-
Grey-Turner sign (reddish-brown discoloration along the flanks resulting from retroperitoneal blood dissecting along tissue planes); more commonly, patients may have a ruddy erythema in the flanks secondary to extravasated pancreatic exudate
-
Erythematous skin nodules, usually no larger than 1 cm and typically located on extensor skin surfaces; polyarthritis
See Presentation for more detail.
Diagnosis
Once a working diagnosis of acute pancreatitis is reached, laboratory tests are obtained to support the clinical impression, such as the following:
-
Serum amylase and lipase
-
Liver-associated enzymes
-
Blood urea nitrogen (BUN), creatinine, and electrolytes
-
Blood glucose
-
Serum cholesterol and triglyceride
-
Complete blood count (CBC) and hematocrit; NLR
-
C-reactive protein (CRP)
-
Arterial blood gas values
-
Serum lactic dehydrogenase (LDH) and bicarbonate
-
Immunoglobulin G4 (IgG4): elevated in autoimmune pancreatitis
Diagnostic imaging is unnecessary in most cases but may be obtained when the diagnosis is in doubt, when pancreatitis is severe, or when a given study might provide specific information required. Modalities employed include the following:
-
Abdominal radiography (limited role): Kidneys-ureters-bladder (KUB) radiography with the patient upright is primarily performed to detect free air in the abdomen
-
Abdominal ultrasonography (most useful initial test in determining the etiology, and is the technique of choice for detecting gallstones)
-
Endoscopic ultrasonography (EUS) (used mainly for detection of microlithiasis and periampullary lesions not easily revealed by other methods)
-
Abdominal computed tomography (CT) scanning (generally not indicated for patients with mild pancreatitis but always indicated for those with severe acute pancreatitis)
-
Endoscopic retrograde cholangiopancreatography (ERCP); to be used with extreme caution in this disease and never as a first-line diagnostic tool [1]
-
Magnetic resonance cholangiopancreatography (MRCP) (not as sensitive as ERCP but safer and noninvasive)
Other diagnostic modalities include the following:
-
CT-guided or EUS-guided aspiration and drainage
-
Genetic testing
Acute pancreatitis is broadly classified as either mild or severe. According to the Atlanta classification, severe acute pancreatitis is signaled by the following [2] :
-
Evidence of organ failure (eg, systolic blood pressure below 90 mm Hg, arterial partial pressure of oxygen [Pa O2] 60 mm Hg or lower, serum creatinine level 2 mg/dL or higher, GI bleeding amounting to 500 mL or more in 24 hours)
-
Local complications (eg, necrosis, abscess, pseudocyst)
-
Ranson score of 3 or higher or APACHE score of 8 or higher
See Workup for more detail.
Management
Medical management of mild acute pancreatitis is relatively straightforward; however, patients with severe acute pancreatitis require intensive care.
Initial supportive care includes the following:
-
Fluid resuscitation [3]
-
Nutritional support
Antibiotic therapy is employed as follows:
-
Antibiotics (usually of the imipenem class) should be used in any case of pancreatitis complicated by infected pancreatic necrosis but should not be given routinely for fever, especially early in the presentation
-
Antibiotic prophylaxis in severe pancreatitis is controversial; routine use of antibiotics as prophylaxis against infection in severe acute pancreatitis is not currently recommended
Surgical intervention (open or minimally invasive) is indicated when an anatomic complication amenable to a mechanical solution is present. Procedures appropriate for specific conditions involving pancreatitis include the following:
-
Gallstone pancreatitis: Cholecystectomy
-
Pancreatic duct disruption: Image-guided percutaneous placement of a drainage tube into the fluid collection [4] ; stent or tube placement via ERCP; in refractory cases, distal pancreatectomy or a Whipple procedure
-
Pseudocysts: None necessary in most cases; for large or symptomatic pseudocysts, percutaneous aspiration, endoscopic transpapillary or transmural techniques, or surgical management
-
Infected pancreatic necrosis: Image-guided aspiration; necrosectomy
-
Pancreatic abscess: Percutaneous catheter drainage and antibiotics; if no response, surgical debridement and drainage
See Treatment and Medication for more detail.
Background
This article focuses on the recognition and management of acute pancreatitis. Pancreatitis is an inflammatory process in which pancreatic enzymes autodigest the gland. The gland sometimes heals without any impairment of function or any morphologic changes; this process is known as acute pancreatitis. Pancreatitis can also recur intermittently, contributing to the functional and morphologic loss of the gland; recurrent attacks are referred to as chronic pancreatitis.
Both forms of pancreatitis may present in the emergency department (ED) with acute clinical findings. Recognizing patients with severe acute pancreatitis as soon as possible is critical for achieving optimal outcomes (see Presentation).
Once a working diagnosis of acute pancreatitis is reached, laboratory tests are obtained to support the clinical impression, to help define the etiology, and to look for complications. Diagnostic imaging is unnecessary in most cases but may be obtained when the diagnosis is in doubt, when severe pancreatitis is present, or when an imaging study might provide specific information needed to answer a clinical question. Image-guided aspiration may be useful. Genetic testing may be considered (see Workup).
Management depends largely on severity. Medical treatment of mild acute pancreatitis is relatively straightforward. Treatment of severe acute pancreatitis involves intensive care; the goals of medical management are to provide aggressive supportive care, to decrease inflammation, to limit infection or superinfection, and to identify and treat complications as appropriate. Surgical intervention (open or minimally invasive) is indicated in selected cases (see Treatment).
Pathophysiology
Normal pancreatic function
The pancreas is a gland located in the upper posterior abdomen. It is responsible for insulin production (endocrine pancreas) and the manufacture and secretion of digestive enzymes (exocrine pancreas) leading to carbohydrate, fat, and protein metabolism. Approximately 80% of the gross weight of the pancreas supports exocrine function, and the remaining 20% is involved with endocrine function. The focus of this article is on the exocrine function of the pancreas.
The pancreas accounts for only 0.1% of total body weight but has 13 times the protein-producing capacity of the liver and the reticuloendothelial system combined, which together make up 4% of total body weight. Digestive enzymes are produced within the pancreatic acinar cells, packaged into storage vesicles called zymogens, and then released via the pancreatic ductal cells into the pancreatic duct, where they are secreted into the small intestine to begin the metabolic process.
In normal pancreatic function, up to 15 different types of digestive enzymes are manufactured in the rough endoplasmic reticulum, targeted in the Golgi apparatus and packaged into zymogens as proenzymes. When a meal is ingested, the vagal nerves, vasoactive intestinal polypeptide (VIP), gastrin-releasing peptide (GRP), secretin, cholecystokinin (CCK), and encephalins stimulate the release of these proenzymes into the pancreatic duct.
The proenzymes travel to the brush border of the duodenum, where trypsinogen, the proenzyme for trypsin, is activated via hydrolysis of an N-terminal hexapeptide fragment by the brush border enzyme enterokinase. Trypsin then facilitates the conversion of the other proenzymes into their active forms.
A feedback mechanism exists to limit pancreatic enzyme activation after appropriate metabolism has occurred. It is hypothesized that elevated levels of trypsin, having become unbound from digesting food, lead to decreased CCK and secretin levels, thus limiting further pancreatic secretion.
Because premature activation of pancreatic enzymes within the pancreas leads to organ injury and pancreatitis, several mechanisms exist to limit this occurrence. First, proteins are translated into the inactive proenzymes. Later, posttranslational modification of the Golgi cells allows their segregation into the unique subcellular zymogen compartments. The proenzymes are packaged in a paracrystalline arrangement with protease inhibitors.
Zymogen granules have an acidic pH and a low calcium concentration, which are factors that guard against premature activation until after secretion has occurred and extracellular factors have triggered the activation cascade. Under various conditions, disruption of these protective mechanisms may occur, resulting in intracellular enzyme activation and pancreatic autodigestion leading to acute pancreatitis.
Pathogenesis of acute pancreatitis
Acute pancreatitis may occur when factors involved in maintaining cellular homeostasis are out of balance. The initiating event may be anything that injures the acinar cell and impairs the secretion of zymogen granules; examples include alcohol use, gallstones, and certain drugs.
At present, it is unclear exactly what pathophysiologic event triggers the onset of acute pancreatitis. It is believed, however, that both extracellular factors (eg, neural and vascular response) and intracellular factors (eg, intracellular digestive enzyme activation, increased calcium signaling, and heat shock protein activation) play a role. In addition, acute pancreatitis can develop when ductal cell injury leads to delayed or absent enzymatic secretion, as seen in patients with the CFTR gene mutation.
Once a cellular injury pattern has been initiated, cellular membrane trafficking becomes chaotic, with the following deleterious effects:
-
Lysosomal and zymogen granule compartments fuse, enabling activation of trypsinogen to trypsin
-
Intracellular trypsin triggers the entire zymogen activation cascade
-
Secretory vesicles are extruded across the basolateral membrane into the interstitium, where molecular fragments act as chemoattractants for inflammatory cells
Activated neutrophils then exacerbate the problem by releasing superoxide (the respiratory burst) or proteolytic enzymes (cathepsins B, D, and G; collagenase; and elastase). Finally, macrophages release cytokines that further mediate local (and, in severe cases, systemic) inflammatory responses. The early mediators defined to date are tumor necrosis factor-alpha (TNF-α), interleukin (IL)-6, and IL-8.
These mediators of inflammation cause an increased pancreatic vascular permeability, leading to hemorrhage, edema, and eventually pancreatic necrosis. As the mediators are excreted into the circulation, systemic complications can arise, such as bacteremia due to gut flora translocation, acute respiratory distress syndrome (ARDS), pleural effusions, gastrointestinal (GI) hemorrhage, and renal failure.
The systemic inflammatory response syndrome (SIRS) can also develop, leading to the development of systemic shock. Eventually, the mediators of inflammation can become so overwhelming that hemodynamic instability and death ensue.
In acute pancreatitis, parenchymal edema and peripancreatic fat necrosis occur first; this is known as acute edematous pancreatitis. When necrosis involves the parenchyma, accompanied by hemorrhage and dysfunction of the gland, the inflammation evolves into hemorrhagic or necrotizing pancreatitis. Pseudocysts and pancreatic abscesses can result from necrotizing pancreatitis because enzymes can be walled off by granulation tissue (pseudocyst formation) or via bacterial seeding of the pancreatic or peripancreatic tissue (pancreatic abscess formation).
Li et al compared two sets of patients with severe acute pancreatitis—one with acute renal failure and the other without it—and determined that a history of renal disease, hypoxemia, and abdominal compartment syndrome were significant risk factors for acute renal failure in patients with severe acute pancreatitis. [5] In addition, patients with acute renal failure were found to have a significantly greater average length of stay in the hospital and in the intensive care unit (ICU), as well as higher rates of pancreatic infection and mortality.
Etiology
Long-standing alcohol consumption and biliary stone disease cause most cases of acute pancreatitis, but numerous other etiologies are known. In 10%-30% of cases, the cause is unknown, though studies have suggested that as many as 70% of cases of idiopathic pancreatitis are secondary to biliary microlithiasis.
Biliary tract disease
One of the most common causes of acute pancreatitis in most developed countries (accounting for approximately 40% of cases) is gallstones passing into the bile duct and temporarily lodging at the sphincter of Oddi. The risk of a stone causing pancreatitis is inversely proportional to its size.
It is thought that acinar cell injury occurs secondary to increasing pancreatic duct pressures caused by obstructive biliary stones at the ampulla of Vater, although this has not been definitively proven in humans. Occult microlithiasis is probably responsible for most cases of idiopathic acute pancreatitis.
Alcohol
Alcohol use is a major cause of acute pancreatitis (accounting for at least 35% of cases [6] ). At the cellular level, ethanol leads to intracellular accumulation of digestive enzymes and their premature activation and release. At the ductal level, it increases the permeability of ductules, allowing enzymes to reach the parenchyma and cause pancreatic damage. Ethanol increases the protein content of pancreatic juice and decreases bicarbonate levels and trypsin inhibitor concentrations. This leads to the formation of protein plugs that block pancreatic outflow.
Most commonly, the disease develops in patients whose alcohol ingestion is habitual over 5-15 years. Alcoholics are usually admitted with an acute exacerbation of chronic pancreatitis. Occasionally, however, pancreatitis can develop in a patient with a weekend binging habit, and several case reports have described a sole large alcohol load precipitating a first attack. Nevertheless, the alcoholic who imbibes routinely remains the rule rather than the exception for the development of pancreatitis.
Currently, there is no universally accepted explanation for why certain alcoholics are more predisposed to developing acute pancreatitis than other alcoholics who ingest similar quantities.
Endoscopic retrograde cholangiopancreatography
Pancreatitis occurring after endoscopic retrograde cholangiopancreatography (ERCP) is probably the third most common type (accounting for approximately 4% of cases). Whereas retrospective surveys indicate that the risk is only 1%, prospective studies have shown the risk to be at least 5%.
The risk of post-ERCP acute pancreatitis is increased if the endoscopist is inexperienced, if the patient is thought to have sphincter of Oddi dysfunction, or if manometry is performed on the sphincter of Oddi. Aggressive preintervention intravenous (IV) hydration has been durably shown to prevent post-ERCP pancreatitis in randomized studies. More recently, rectal indomethacin has been employed; it has been shown to reduce the incidence of post-ERCP pancreatitis and is now widely accepted at most institutions. The literature continues to debate the role of rectal indomethacin. [7]
Trauma
Abdominal trauma (approximately 1.5%) causes an elevation of amylase and lipase levels in 17% of cases and clinical pancreatitis in 5% of cases. Pancreatic injury occurs more often in penetrating injuries (eg, from knives, bullets) than in blunt abdominal trauma (eg, from steering wheels, horses, bicycles). Blunt injury to the abdomen or back may crush the gland across the spine, leading to a ductal injury.
Drugs
Considering the small number of patients who develop pancreatitis compared to the relatively large number who receive potentially toxic drugs, drug-induced pancreatitis is a relatively rare occurrence (accounting for approximately 2% of cases) that is probably related to an unknown predisposition. Fortunately, drug-induced pancreatitis is usually mild.
Drugs definitely associated with acute pancreatitis include the following:
-
Azathioprine
-
Sulfonamides
-
Sulindac
-
Tetracycline
-
Valproic acid,
-
Didanosine
-
Methyldopa
-
Estrogens
-
Furosemide
-
6-Mercaptopurine
-
Pentamidine
-
5-aminosalicylic acid compounds
-
Corticosteroids
-
Octreotide
Drugs probably associated with acute pancreatitis include the following:
-
Chlorothiazide and hydrochlorothiazide
-
Methandrostenolone (methandienone)
-
Metronidazole
-
Nitrofurantoin
-
Phenformin
-
Piroxicam
-
Procainamide
-
Colaspase
-
Chlorthalidone
-
Combination cancer chemotherapy drugs (especially asparaginase)
-
Cimetidine
-
Cisplatin
-
Cytosine arabinoside
-
Diphenoxylate
-
Ethacrynic acid
In addition, there are many drugs that have been reported to cause acute pancreatitis in isolated or sporadic cases.
Less common causes
The following causes each account for less than 1% of cases of pancreatitis.
Infection
Several infectious diseases may cause pancreatitis, especially in children. These cases of acute pancreatitis tend to be milder than cases of acute biliary or alcohol-induced pancreatitis.
Viral causes include mumps virus, coxsackievirus, cytomegalovirus (CMV), hepatitis virus, Epstein-Barr virus (EBV), echovirus, varicella-zoster virus (VZV), measles virus, and rubella virus. Bacterial causes include Mycoplasma pneumoniae, Salmonella, Campylobacter, and Mycobacterium tuberculosis. Worldwide, Ascaris is a recognized cause of pancreatitis resulting from the migration of worms in and out of the duodenal papillae.
Pancreatitis has been associated with AIDS; however, this may be the result of opportunistic infections, neoplasms, lipodystrophy, or drug therapies.
Hereditary pancreatitis
Hereditary pancreatitis is an autosomal dominant gain-of-function disorder related to mutations of the cationic trypsinogen gene (PRSS1), which has an 80% penetrance. Mutations in this gene cause premature activation of trypsinogen to trypsin.
In addition, the CFTR mutation plays a role in predisposing patients to acute pancreatitis by causing abnormalities of ductal secretion. At present, however, the phenotypic variability of patients with the CFTR mutation is not well understood. Certainly, patients homozygous for the CFTR mutation are at risk for pancreatic disease, but it is not yet clear which of the more than 800 mutations carries the most significant risk. In addition, the role of CFTR heterozygotes in pancreatic disease is unknown.
Mutations in the SPINK1 protein, which blocks the active binding site of trypsin, rendering it inactive, also probably play a role in causing a predisposition to acute pancreatitis.
This probably explains the predisposition, rather than the cause, of acute pancreatitis in these patients. If enough mutant enzymes become activated intracellularly, they can overwhelm the first line of defense (ie, pancreatic secretory trypsin inhibitor) and resist backup defenses (ie, proteolytic degradation by mesotrypsin, enzyme Y, and trypsin itself). Activated mutant cationic trypsin can then trigger the entire zymogen activation cascade.
Hypercalcemia
Hypercalcemia from any cause can lead to acute pancreatitis. Causes include hyperparathyroidism, excessive doses of vitamin D, familial hypocalciuric hypercalcemia, and total parenteral nutrition (TPN). Routine use of automated serum chemistries has allowed earlier detection and reduced the frequency of hypercalcemia manifesting as pancreatitis.
Developmental abnormalities of pancreas
The pancreas develops from two buds stemming from the alimentary tract of the developing embryo. There are two developmental abnormalities commonly associated with pancreatitis: pancreas divisum and annular pancreas.
Pancreas divisum is a failure of the dorsal and ventral pancreatic ducts to fuse during embryogenesis. Probably a variant of normal anatomy, it occurs in approximately 5% of the population (see the images below); in most cases, it may actually protect against gallstone pancreatitis. It appears that the presence of a stenotic minor papillae and an atretic duct of Santorini are additional risk factors that together contribute to the development of acute pancreatitis through an obstructive mechanism (although this is controversial).
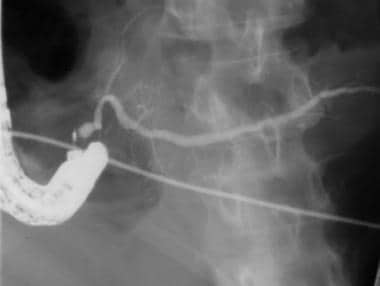 Acute pancreatitis. This image was obtained from a patient with pancreas divisum associated with minor papilla stenosis causing recurrent pancreatitis. Because pancreas divisum is relatively common in the general population, it is best regarded as a variant of normal anatomy and not necessarily as a cause of pancreatitis. In this case, note the bulbous contour of the duct adjacent to the cannula. This appearance has been termed Santorinicele. Dorsal duct outflow obstruction is a probable cause of pancreatitis when Santorinicele is present, and it is associated with a minor papilla that accommodates only a guide wire.
Acute pancreatitis. This image was obtained from a patient with pancreas divisum associated with minor papilla stenosis causing recurrent pancreatitis. Because pancreas divisum is relatively common in the general population, it is best regarded as a variant of normal anatomy and not necessarily as a cause of pancreatitis. In this case, note the bulbous contour of the duct adjacent to the cannula. This appearance has been termed Santorinicele. Dorsal duct outflow obstruction is a probable cause of pancreatitis when Santorinicele is present, and it is associated with a minor papilla that accommodates only a guide wire.
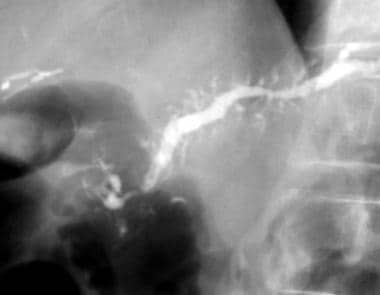 Acute pancreatitis. Recurrent pancreatitis was associated with pancreas divisum in an elderly man. The pancreatogram of the dorsal duct shows distal stenosis with upstream chronic pancreatitis. After the stenosis was dilated and stented, his pain resolved and the patient improved clinically during 1 year of quarterly stent exchanges. Follow-up computed tomography (CT) scans showed resolution of the inflammatory mass. Although ductal biopsies and cytology were repeatedly negative, the patient's pain and pancreatitis returned when the stents were removed. He developed duodenal outflow obstruction and was sent to surgery; during the Whipple procedure, periampullary adenocarcinoma (of minor papilla) was revealed.
Acute pancreatitis. Recurrent pancreatitis was associated with pancreas divisum in an elderly man. The pancreatogram of the dorsal duct shows distal stenosis with upstream chronic pancreatitis. After the stenosis was dilated and stented, his pain resolved and the patient improved clinically during 1 year of quarterly stent exchanges. Follow-up computed tomography (CT) scans showed resolution of the inflammatory mass. Although ductal biopsies and cytology were repeatedly negative, the patient's pain and pancreatitis returned when the stents were removed. He developed duodenal outflow obstruction and was sent to surgery; during the Whipple procedure, periampullary adenocarcinoma (of minor papilla) was revealed.
Annular pancreas is an uncommon congenital anomaly in which a band of pancreatic tissue surrounds the second part of the duodenum. Usually, it does not cause symptoms until later in life. This condition is a rare cause of acute pancreatitis, probably through an obstructive mechanism.
Sphincter of Oddi dysfunction can lead to acute pancreatitis by causing increased pancreatic ductal pressures. However, the mechanism of pancreatitis induced by such dysfunction in patients without elevated sphincter pressures on manometry remains controversial.
Hypertriglyceridemia
Clinically significant pancreatitis usually does not occur until a person’s serum triglyceride level reaches 1000 mg/dL. It is associated with type I and type V hyperlipidemia. Although this view is somewhat controversial, most authorities believe that the association is caused by the underlying derangement in lipid metabolism rather than by pancreatitis causing hyperlipidemia. This type of pancreatitis tends to be more severe than alcohol- or gallstone-induced disease.
Tumors
Obstruction of the pancreatic ductal system by a pancreatic ductal carcinoma, ampullary carcinoma, islet cell tumor, solid pseudotumor of the pancreas, sarcoma, lymphoma, cholangiocarcinoma, or metastatic tumor can cause acute pancreatitis. The chances of pancreatitis occurring when a tumor is present are approximately 14%. Pancreatic cystic neoplasms, such as intraductal papillary-mucinous neoplasm (IPMN), mucinous cystadenoma, or serous cystadenoma, can also cause pancreatitis.
Toxins
Exposure to organophosphate insecticide can cause acute pancreatitis. Scorpion and snake bites may also be causative; in Trinidad, the sting of the scorpion Tityus trinitatis is the most common cause of acute pancreatitis. Hyperstimulation of pancreas exocrine secretion appears to be the mechanism of action in both instances.
Surgical procedures
Acute pancreatitis may occur in the postoperative period of various surgical procedures (eg, abdominal or cardiopulmonary bypass surgery, which may damage the gland by causing ischemia). Postoperative acute pancreatitis is often a difficult diagnosis to confirm, and it has a higher complication rate than pancreatitis associated with other etiologies. The mechanism is unclear.
Vascular abnormalities
Vascular factors, such as ischemia or vasculitis, can play a role in causing acute pancreatitis. Vasculitis can predispose patients to pancreatic ischemia, especially in those with polyarteritis nodosa and systemic lupus erythematosus.
Autoimmune pancreatitis
Autoimmune pancreatitis, a relatively newly described entity, is an extremely rare cause of acute pancreatitis (prevalence, 0.82 per 100,000 individuals). When it does cause acute pancreatitis, it is usually in young people (approximately age 40 years) who may also suffer from other autoimmune diseases. The pathogenesis is unclear, but it is potentially related to immunoglobulin (Ig) G4 autoimmune disease. [8]
Epidemiology
United States statistics
Acute pancreatitis has an approximate incidence of 40-50 cases per year per 100,000 adults. [9] In 2009, approximately 275,000 hospitalizations were attributed to acute pancreatitis. [10] In 2007, approximately 220,000 patients with acute pancreatitis were admitted to non–federally funded hospitals. In 1998, 183,000 patients with acute pancreatitis were admitted. This trend in rising incidence has been recognized over the past several decades. [9, 11, 12, 13]
International statistics
Worldwide, the incidence of acute pancreatitis ranges between 5 and 80 per 100,000 population, with the highest incidence recorded in the United States and Finland. [14] In Luneburg, Germany, the incidence is 17.5 cases per 100,000 people. In Finland, the incidence is 73.4 cases per 100,000 people. Similar incidence rates have been reported in Australia. The incidence of disease outside North America, Europe, and Australia is less well known.
In Europe and other developed nations, such as Hong Kong, more patients tend to have gallstone pancreatitis, whereas in the United States, alcoholic pancreatitis is most common.
Age-related demographics
The median age at onset depends on the etiology. [15] The following are median ages of onset for various etiologies:
-
Alcohol-related - 39 years
-
Biliary tract–related - 69 years
-
Trauma-related - 66 years
-
Drug-induced etiology - 42 years
-
ERCP-related - 58 years
-
AIDS-related - 31 years
-
Vasculitis-related - 36 years
Hospitalization rates increase with age. For people aged 35-75 years, the rate doubles for males and quadruples for females.
Sex-related demographics
Generally, acute pancreatitis affects males more often than females. In males, the etiology is more often related to alcohol; in females, it is more often related to biliary tract disease. Idiopathic pancreatitis has no clear predilection for either sex.
Race-related demographics
The hospitalization rates of patients with acute pancreatitis per 100,000 population are 3 times higher for blacks than whites. These racial differences are more pronounced for males than females. The risk for African Americans aged 35-64 years is 10 times higher than for any other group. African Americans are at a higher risk than whites in that same age group.
The annual incidence of acute pancreatitis in Native Americans is 4 per 100,000 population; in whites, 5.7 per 100,000 population; and in blacks, 20.7 per 100,000 population. [16]
Prognosis
The overall mortality in patients with acute pancreatitis is 10%-15%. Patients with biliary pancreatitis tend to have a higher mortality than patients with alcoholic pancreatitis. This rate has been falling over the last 2 decades as improvements in supportive care have been initiated. Type 2 diabetes mellitus has also been associated with higher severity and mortality in the setting of acute pancreatitis. [17] In patients with severe disease (organ failure), who account for about 20% of presentations, mortality is approximately 30%. [18] This figure has not decreased in the past 10 years. In patients with pancreatic necrosis without organ failure, the mortality approaches zero.
In the first week of illness, most deaths result from multiorgan system failure. In subsequent weeks, infection plays a more significant role, but organ failure still constitutes a major cause of mortality. Acute respiratory distress syndrome (ARDS), acute renal failure, cardiac depression, hemorrhage, and hypotensive shock all may be systemic manifestations of acute pancreatitis in its most severe form.
Identifying patients in the greatest need of aggressive medical treatment by differentiating their disease severity as mild or severe is recommended. In mild disease, the pancreas exhibits interstitial edema, an inflammatory infiltrate without hemorrhage or necrosis, and, usually, minimal or no organ dysfunction. In severe disease, the inflammatory infiltrate is severe, associated with necrosis of the parenchyma, often accompanied by evidence of severe gland dysfunction, and it may be associated with multiorgan system failure.
Different strategies have been used to assess the severity of acute pancreatitis and predict outcome (see Workup and Staging). Several clinical scoring systems (eg, Ranson criteria, Glasgow, Imrie) are available. The APACHE II scoring system, though cumbersome, appears to be the best validated (see the APACHE II Scoring System calculator). Biological markers have also been used for this purpose. Genetic markers are being studied and have not yet come into clinical use.
Peritoneal lavage has a high specificity (93%); however, it has a low sensitivity (54%). Dynamic CT scanning of the abdomen is widely available and useful in predicting the outcome of acute pancreatitis. When the Balthazar criteria (see Workup and Computed Tomography Scanning) are used, sensitivity is 87% and specificity is 88%.
Suppiah et al examined the prognostic value of the neutrophil-lymphocyte ratio (NLR) in 146 consecutive patients with acute pancreatitis. [19] They found that elevation of the NLR during the first 48 hours of hospital admission was significantly associated with severe acute pancreatitis and was an independent negative prognostic indicator. The NLR is calculated from the white cell differential and provides an indication of inflammation.
Khan et al examined the prognostic value of Modified Early Warning Score (MEWS) in identifying severe acute pancreatitis in 200 patients admitted to a single institution. [20] The investigators tracked the highest and mean daily scores. They found that patients with a high MEWS value > 2 on day one or mean value > 1.2 on day two was most accurate in predicting severe acute pancreatitis. The investigators concluded that MEWS is a reliable, safe, and inexpensive score that can be used easily at all levels of health care for prognosticating patients with acute pancreatitis.
In a retrospective study of data from 822 patients hospitalized with acute pancreatitis, Mikolasevic et al found that patients who had nonalcoholic fatty liver at admission (n = 198; 24.1%) had a statistically higher incidence of moderately severe (35.4% vs 14.6%) and severe acute pancreatitis (20.7% vs 9.6%) than those without nonalcoholic fatty liver. [21] Moreover, these patients had higher (1) C-reactive protein levels not only on the day of admission but also at day 3, (2) APACHE II scores at admission, (3) CT scan severity index, and (4) occurrence of organ failure and local complications. Although mortality was also higher in the nonalcoholic fatty liver group compared to the group without this disease, the difference was not statistically significant. [21]
Complications
Acute fluid collections may occur, typically early in the course of acute pancreatitis. These are primarily detected by imaging studies rather than by physical examination. Because they lack a defined wall and usually regress spontaneously, most acute fluid collections require no specific therapy.
An acute pseudocyst is a collection of pancreatic fluid that is walled off by granulation tissue after an episode of acute pancreatitis; it requires 4 or more weeks to develop. Although pseudocysts are sometimes palpable on physical examination, they are usually detected with abdominal ultrasonography or computed tomography (CT).
Intra-abdominal infection is common. Within the first 1-3 weeks, fluid collections or pancreatic necrosis can become infected and jeopardize clinical outcome. From 3 to 6 weeks, pseudocysts may become infected or a pancreatic abscess may develop. A pancreatic abscess is a circumscribed intra-abdominal collection of pus, within or in proximity to the pancreas. It is believed to arise from localized necrosis, with subsequent liquefaction that becomes infected.
The intestinal flora is the predominant source of bacteria causing the infection. The usual suspects are Escherichia coli (26%), Pseudomonas species (16%), Staphylococcus species (15%), Klebsiella species (10%), Proteus species (10%), Streptococcus species (4%), Enterobacter species (3%), and anaerobic organisms (16%). Fungal superinfections may occur weeks or months into the course of severe necrotizing pancreatitis.
Pancreatic necrosis is a nonviable area of pancreatic parenchyma that is often associated with peripancreatic fat necrosis and is principally diagnosed with the aid of dynamic spiral CT scans. Distinguishing between infected and sterile pancreatic necrosis is an ongoing clinical challenge. Sterile pancreatic necrosis is usually treated with aggressive medical management, whereas almost all patients with infected pancreatic necrosis require surgical debridement or percutaneous drainage if they are to survive.
Hemorrhage into the gastrointestinal (GI) tract, retroperitoneum, or the peritoneal cavity is possible because of erosion of large vessels. Intestinal obstruction or necrosis may occur. Common bile duct obstruction may be caused by a pancreatic abscess, pseudocyst, or biliary stone that caused the pancreatitis. An internal pancreatic fistula from pancreatic duct disruption or a leaking pancreatic pseudocyst may occur.
In the weeks (to months) following presentation, the physician’s attention shifts to developing signs of intra-abdominal infection, pancreatic pseudocyst, intra-abdominal hemorrhage, colon perforation, obstruction or fistulization, and multiorgan system failure.
Patient Education
Educate patients about the disease, and advise them to avoid alcohol in binge amounts and to discontinue any risk factor, such as fatty meals and abdominal trauma.
For patient education resources, see the Cholesterol Center, as well as Pancreatitis and Gallstones.
-
Acute pancreatitis. Suspected acute pancreatitis. Etiologic factors and forms of acute pancreatitis. Ranson criteria.
-
Acute pancreatitis. Mild pancreatitis. Favorable prognostic signs for acute pancreatitis. Medical management and studies used for acute pancreatitis.
-
Acute pancreatitis. Prognostic indicators for severe pancreatitis and intensive care unit management.
-
Acute pancreatitis. Diagnosis and treatment of necrotizing pancreatitis.
-
Acute pancreatitis. Treatment of and studies used for pancreatic pseudocysts.
-
Acute pancreatitis. Idiopathic recurrent pancreatitis. Etiologies for acute pancreatitis.
-
Acute pancreatitis. Pancreatic abscess. Definition of an abscess.
-
Acute pancreatitis. A patient with acute gallstone pancreatitis underwent endoscopic retrograde cholangiopancreatography. The cholangiogram showed no stones in the common bile duct and multiple small stones in the gallbladder. The pancreatogram shows narrowing of the pancreatic duct in the area of genu, resulting from extrinsic compression of the ductal system by inflammatory changes in the pancreas.
-
Acute pancreatitis. This image was obtained from a patient with pancreas divisum associated with minor papilla stenosis causing recurrent pancreatitis. Because pancreas divisum is relatively common in the general population, it is best regarded as a variant of normal anatomy and not necessarily as a cause of pancreatitis. In this case, note the bulbous contour of the duct adjacent to the cannula. This appearance has been termed Santorinicele. Dorsal duct outflow obstruction is a probable cause of pancreatitis when Santorinicele is present, and it is associated with a minor papilla that accommodates only a guide wire.
-
Acute pancreatitis. A normal-appearing ventral pancreas is seen in a patient with recurrent acute pancreatitis. Dorsal pancreas (not pictured) showed evidence of chronic pancreatitis.
-
Acute pancreatitis. Endoscopic retrograde cholangiopancreatography excluded suppurative cholangitis and established the presence of anular pancreas divisum. The dorsal pancreatogram showed extravasation into the retroperitoneum, and sphincterotomy was performed on the minor papilla. A pigtail nasopancreatic tube was then inserted into the dorsal duct and out into the retroperitoneal fluid collection. The other end of the tube was attached to bulb suction and monitored every shift.
-
Acute pancreatitis. Although percutaneous drains remove loculated fluid collections elsewhere in the abdomen, a nasopancreatic tube drains the retroperitoneal fluid collection. One week later, the retroperitoneal fluid collection was much smaller (the image is reversed in a horizontal direction). By this time, the patient was off pressors and was ready to be extubated.
-
Acute pancreatitis. Recurrent pancreatitis was associated with pancreas divisum in an elderly man. The pancreatogram of the dorsal duct shows distal stenosis with upstream chronic pancreatitis. After the stenosis was dilated and stented, his pain resolved and the patient improved clinically during 1 year of quarterly stent exchanges. Follow-up computed tomography (CT) scans showed resolution of the inflammatory mass. Although ductal biopsies and cytology were repeatedly negative, the patient's pain and pancreatitis returned when the stents were removed. He developed duodenal outflow obstruction and was sent to surgery; during the Whipple procedure, periampullary adenocarcinoma (of minor papilla) was revealed.
Tables
| Acute pancreatitis (any) or a history of post-ERCP pancreatitis |
| Younger age |
| Female sex |
| Absence of bile duct stones |
| More than 10 attempts to cannulate the papilla of Vater |
| Pancreatic duct cannulation |
| Contrast medium injection of the pancreatic system |
| Pancreatic sphincterotomy |
| Sphincter of Oddi dysfunction |
