Practice Essentials
Paronychia is a soft tissue infection around a fingernail or toenail that begins as cellulitis but that may progress to a definite abscess. [1] The 2 types of paronychia are as follows [2] :
-
Acute paronychia - Painful and purulent condition; most frequently caused by staphylococci
-
Chronic paronychia - Usually caused by a fungal infection
The image below depicts paronychia.
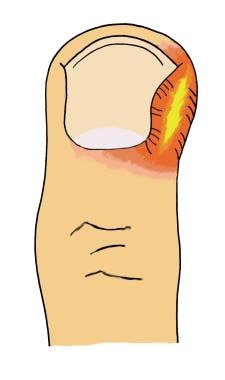
 Classic presentation of paronychia, with erythema and pus surrounding the nail bed. In this case, the paronychia was due to infection after a hangnail was removed.
Classic presentation of paronychia, with erythema and pus surrounding the nail bed. In this case, the paronychia was due to infection after a hangnail was removed.
Signs and symptoms
Physical findings in acute paronychia include the following:
-
The affected area often appears erythematous and swollen
-
In more advanced cases, pus may collect under the skin of the lateral fold
-
If untreated, the infection can extend into the eponychium, in which case it is called eponychia
Further extension of the infection can lead to the involvement of both lateral folds as it tracks under the nail sulcus; this progression is called a runaround infection
Physical findings in chronic paronychia include the following:
-
Swollen, erythematous, and tender nail folds without fluctuance are characteristic of chronic paronychia
-
Eventually, the nail plates become thickened and discolored, with pronounced transverse ridges
-
The cuticles and nail folds may separate from the nail plate, forming a space for the invasion of various microorganisms
See Clinical Presentation for more detail.
Diagnosis
The diagnosis of paronychia is based primarily on patient history and physical examination. Some laboratory studies, however, can be useful. These include the following:
-
Gram staining and/or culture - To help identify a bacterial cause of fluctuant paronychia
-
Potassium hydroxide (KOH) 5% smears - To help diagnose paronychia caused by a candidal infection
-
Tzanck smears - If herpetic whitlow is suspected
-
See Workup for more detail.
Management
Treatment strategies for paronychia include the following:
-
If an abscess has developed, incision and drainage must be performed
See Treatment and Medication for more detail.
Background
Paronychia is a soft tissue infection around a fingernail. More specifically, it is a superficial infection of epithelium lateral to the nail plate that begins as cellulitis but that may progress to a definite abscess. [1] The 2 forms of paronychia, acute and chronic, usually differ in etiology, infectious agent, and treatment and are often considered separate entities. [2]
The acute infection, which is painful and purulent, is most frequently caused by staphylococci, although it commonly has mixed aerobic and anaerobic flora. [7] The patient's condition and discomfort are markedly improved by a simple drainage procedure. Chronic paronychial infections are usually fungal, rather than bacterial, in nature (see the images below).
Classic presentation of paronychia, with erythema and pus surrounding the nail bed. In this case, the paronychia was due to infection after a hangnail was removed.
 In this case of paronychia, no pus or fluctuance is involved in the nail bed itself.
In this case of paronychia, no pus or fluctuance is involved in the nail bed itself.
Epidemiology
Paronychia is the most common hand infection in the United States, representing 35% of these disorders. [3] The infection is more common in women than in men, with a female-to-male ratio of 3:1.
Quality of life
A study by Belyayeva et al indicated that certain nail disorders, including paronychia, can have a particularly high impact on quality of life. Using responses to a questionnaire from 1063 patients with disorders of the fingernails and/or toenails, the investigators found that the effect on quality of life was greatest in patients with nail problems resulting from trauma, infections (including onychomycosis and paronychia), structural abnormalities, and inflammatory diseases (including psoriasis). Quality of life was particularly reduced in women, patients aged 60-79 years, and persons with multiple nail involvement. [8]
According to the report, the results suggest that quality of life is influenced more by the effect of a nail disease on the appearance of the nail than it is by the actual severity of the disease.
Anatomy
The nail organ is an integral component of the digital tip. It is a highly versatile tool that protects the fingertip, contributes to tactile sensation by acting as a counterforce to the fingertip pad, and aids in peripheral thermoregulation via glomus bodies in the nail bed and matrix. Because of its form and functionality, abnormalities of the nail unit result in functional and cosmetic issues.
The anatomy of the nail complex is shown in the image below. The nail is longitudinally flanked by 2 lateral folds, or perionychium. Proximally, it is covered by the eponychium. Distal to the perionychium, the region immediately beneath the free edge of the nail is the hyponychium. The hyponychium serves as a tough physical barrier that resists bacterial infection.
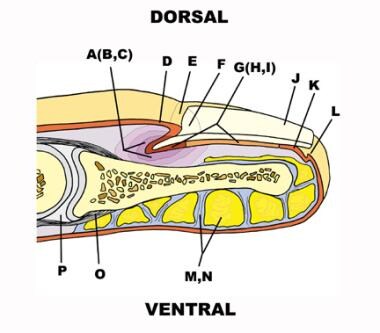 Depicted are the nail fold (A), dorsal roof (B), ventral floor (C), nail wall (D), perionychium (E), lunula (F), nail bed (G), germinal matrix (H), sterile matrix (I), nail plate (J), hyponychium (K), distal groove (L), fascial septa (M), fat pad (N), distal interphalangeal joint (O), and extensor tendon insertion (P).
Depicted are the nail fold (A), dorsal roof (B), ventral floor (C), nail wall (D), perionychium (E), lunula (F), nail bed (G), germinal matrix (H), sterile matrix (I), nail plate (J), hyponychium (K), distal groove (L), fascial septa (M), fat pad (N), distal interphalangeal joint (O), and extensor tendon insertion (P).
Nail plate and bed
The nail, or nail plate, lies immediately on top of the nail bed, which consists of the following 2 portions, which are involved in the production, migration, and maintenance of the nail:
-
Proximal portion - Called the germinal matrix; contains active cells that are responsible for generating new nail; damage to the germinal matrix results in malformed nails
-
Distal portion - Called the sterile matrix; adds thickness, bulk, and strength to the nail
The white, crescent-shaped opacity at the proximal end of the nail is the lunula, which is the visible portion of the germinal matrix. The whiteness of the lunula is due to the poor vascularity of the germinal matrix.
Nail fold
The nail arises from a mild proximal depression called the nail fold. The nail divides the nail fold into 2 components: the dorsal roof and the ventral floor, both of which contain germinal matrices. The skin overlying the nail fold is called the nail wall.
Vascular system
The nail bed receives its blood supply from the 2 terminal branches of the volar digital artery. A fine network in the proximal nail bed and in the skin proximal to the nail fold of the finger provides venous drainage. Lymphatic drainage follows a course similar to that of the venous network. The lymphatic network is dense in the nail bed, especially in the hyponychium. Innervation is derived from the trifurcation of the dorsal branch of the volar digital nerve. One branch goes to the nail fold, one to the pulp, and one to the distal tip of the finger.
Pathophysiology and Etiology
Paronychia, whether acute or chronic, results from a breakdown of the protective barrier between the nail and the nail fold. The occurrence of cracks, fissures, or trauma allowing organisms to enter the moist nail crevice leads to bacterial or fungal (yeast or mold) colonization of the area. [9] Early in the course of this disease process (< 24 h), cellulitis alone may be present. An abscess can form if the infection does not resolve quickly.
Acute paronychia
Acute paronychia usually results from a traumatic event, however minor, that breaks down the physical barrier between the nail bed and the nail; this disruption allows the infiltration of infectious organisms. (See the image below.)
 Paronychial erythema and edema with associated pustule. This suggests a bacterial etiology.
Paronychial erythema and edema with associated pustule. This suggests a bacterial etiology.
Acute paronychia can result from seemingly innocuous conditions, such as hangnails, or from activities such as nail biting, finger sucking, manicuring, or artificial nail placement. Causative organisms include the following [10] :
-
Staphylococcus aureus - The most common infecting organism
-
Streptococcus species
-
Pseudomonas species
-
Gram-negative bacteria
-
Anaerobic bacteria
-
Fusarium species [11]
Chronic paronychia
Chronic paronychia is caused primarily by the yeast fungus Candida albicans. [12] Other, rare causes of chronic paronychia include the following:
-
Bacterial, mycobacterial, or viral infection
-
Metastatic cancer
-
Subungual melanoma
-
Squamous cell carcinoma
Therefore, benign and malignant neoplasms should always be excluded when chronic paronychia does not respond to conventional treatment.
Chronic paronychia most often occurs in persons whose hands are repeatedly exposed to moist environments or in those who have prolonged and repeated contact with irritants such as mild acids, mild alkalis, or other chemicals. People who are most susceptible include housekeepers, dishwashers, bartenders, florists, bakers, and swimmers. In addition, individuals who are immunocompromised, such as those with human immunodeficiency virus (HIV) infection or those undergoing steroid therapy, are predisposed to paronychia.
Other conditions associated with abnormalities of the nail fold that predispose individuals to chronic paronychia include psoriasis, mucocutaneous candidiasis, and drug toxicity from medications such as retinoids, epidermal growth factor receptor inhibitors (cetuximab) (tyrosine kinase inhibitors [neratinib, afatinib]), [13, 14] and protease inhibitors. [15, 16] Of particular interest is the antiretroviral drug indinavir, which induces retinoidlike effects and remains the most frequent cause of chronic paronychia in patients with HIV disease.
Pemphigus vulgaris
Acute or chronic paronychia may also occur as a manifestation of other diseases, such as pemphigus vulgaris. Although nail involvement in pemphigus vulgaris is rare, it can be severe, involving multiple digits and hemorrhage. [17]
Prognosis
If treated promptly, paronychia usually has a good prognosis, but it potentially can result in a more serious infection, such as septic tenosynovitis, osteomyelitis, [18] or, by spreading to the pulp space of the finger, a felon. Such infections develop more readily in patients who are immunosuppressed or in those whose condition has been mistreated or neglected. Secondary ridging, thickening, and discoloration of the nail can also occur, as may nail loss. Occasionally, patients suffer systemic infection from hematogenous extension. [19]
Patient Education
Instruct individuals to avoid any trauma to the fingernails and to avoid nail biting and finger sucking. Educate patients who work with their hands in a moist environment that such exposure predisposes them to infections. Inform patients that treatment is unlikely to be successful if their exposure to a moist or wet environment is not changed. Explain to patients who are immunocompromised that they must remain vigilant against any minor trauma to the fingertips and nails.
For patient education information, see the Skin Conditions and Beauty Center, as well as Paronychia (Nail Infection) and Nail Psoriasis.
-
Classic presentation of paronychia, with erythema and pus surrounding the nail bed. In this case, the paronychia was due to infection after a hangnail was removed.
-
In this case of paronychia, no pus or fluctuance is involved in the nail bed itself.
-
Typical appearance of paronychia.
-
Depicted are the nail fold (A), dorsal roof (B), ventral floor (C), nail wall (D), perionychium (E), lunula (F), nail bed (G), germinal matrix (H), sterile matrix (I), nail plate (J), hyponychium (K), distal groove (L), fascial septa (M), fat pad (N), distal interphalangeal joint (O), and extensor tendon insertion (P).
-
Simple acute paronychia can be drained by elevating the eponychial fold from the nail with a small blunt instrument such as a metal probe or elevator.
-
Paronychia incision and drainage.
-
Paronychial erythema and edema with associated pustule. This suggests a bacterial etiology.
-
Paronychia, side view.
-
After simple drainage, there is purulent return.
-
Wound opened with a small incision using a No. 11 blade scalpel.
-
The wound can be explored with a blunt probe, clamps, or the blunt end of a cotton swab.
-
Ensure that all loculations are broken up and that as much pus as possible is evacuated.
-
Prior to packing or dressing the wound, irrigate the wound with normal saline under pressure, using a splash guard, eye protection, or both.
-
The wound can be covered with antibiotic ointment or petroleum jelly to prevent bandage adhesion.
