McCormack WM. Infections due to Mycoplasmas. Kasper DL, Braunwald E, Fauci AS, et al, eds. Harrison's Principles of Internal Medicine. New York: McGraw-Hill; 2005. 16th ed.: 1008-11, 159.
Reimann HA. An acute infection of the respiratory tract with atypical pneumonia: a disease entity probably caused by a filtrable virus. JAMA. 1938. 111:2377-84.
Eaton MD, Meiklejohn G, VanHerick W. Studies on the etiology of primary atypical pneumonia: a filterable agent transmissible to cotton rats, hamsters, and chick embryos. J Exp Med. 1944. 79:649-67.
Kamizono S, Ohya H, Higuchi S, Okazaki N, Narita M. Three familial cases of drug-resistant Mycoplasma pneumoniae infection. Eur J Pediatr. 2010 Jun. 169(6):721-6. [QxMD MEDLINE Link].
Isozumi R, Yoshimine H, Morozumi M, Ubukata K, Ariyoshi K. Adult community-acquired pneumonia caused by macrolide resistant Mycoplasma pneumoniae. Respirology. 2009 Nov. 14(8):1206-8. [QxMD MEDLINE Link].
Matsubara K, Morozumi M, Okada T, Matsushima T, Komiyama O, Shoji M, et al. A comparative clinical study of macrolide-sensitive and macrolide-resistant Mycoplasma pneumoniae infections in pediatric patients. J Infect Chemother. 2009 Dec. 15(6):380-3. [QxMD MEDLINE Link].
Lee H, Yun KW, Lee HJ, Choi EH. Antimicrobial therapy of macrolide-resistant Mycoplasma pneumoniae pneumonia in children. Expert Rev Anti Infect Ther. 2017 Dec 11. 1-12. [QxMD MEDLINE Link].
Copete AR, Aguilar YA, Rueda ZV, Vélez LA. Genotyping and macrolide resistance of Mycoplasma pneumoniae identified in children with community-acquired pneumonia in Medellín, Colombia. Int J Infect Dis. 2017 Nov 15. 66:113-120. [QxMD MEDLINE Link].
Blyth CC, Gerber JS. Macrolides in Children With Community-Acquired Pneumonia: Panacea or Placebo?. J Pediatric Infect Dis Soc. 2017 Oct 31. [QxMD MEDLINE Link].
Tashiro M, Fushimi K, Kawano K, Takazono T, Saijo T, Yamamoto K, et al. Comparison of Efficacy of Antimicrobial Agents Among Hospitalized Patients With Mycoplasma pneumoniae Pneumonia in Japan During Large Epidemics of Macrolide-Resistant M. pneumoniae Infections: A Nationwide Observational Study. Clin Infect Dis. 2017 Nov 13. 65 (11):1837-1842. [QxMD MEDLINE Link].
Lee SW, Yang SS, Chang CS, Yeh HJ, Chow WK. Mycoplasma pneumonia-associated acute hepatitis in an adult patient without lung infection. J Chin Med Assoc. 2009 Apr. 72(4):204-6. [QxMD MEDLINE Link].
Quioc JJ, Trabut JB, Drouhin F, Malbrunot C, Vallet-Pichard A, Pol S, et al. Acute cholestatic hepatitis revealing Mycoplasma pneumoniae infection without lung involvement in an adult patient. Eur J Gastroenterol Hepatol. 2009 Feb. 21(2):220-1. [QxMD MEDLINE Link].
Okoli K, Gupta A, Irani F, Kasmani R. Immune thrombocytopenia associated with Mycoplasma pneumoniae infection: a case report and review of literature. Blood Coagul Fibrinolysis. 2009 Oct. 20(7):595-8. [QxMD MEDLINE Link].
Khan FY, A yassin M. Mycoplasma pneumoniae associated with severe autoimmune hemolytic anemia: case report and literature review. Braz J Infect Dis. 2009 Feb. 13(1):77-9. [QxMD MEDLINE Link].
Wetter DA, Camilleri MJ. Clinical, etiologic, and histopathologic features of Stevens-Johnson syndrome during an 8-year period at Mayo Clinic. Mayo Clin Proc. 2010 Feb. 85(2):131-8. [QxMD MEDLINE Link]. [Full Text].
Yachoui R, Kolasinski SL, Feinstein DE. Mycoplasma pneumoniae with atypical stevens-johnson syndrome: a diagnostic challenge. Case Rep Infect Dis. 2013. 2013:457161. [QxMD MEDLINE Link]. [Full Text].
Azumagawa K, Kambara Y, Murata T, Tamai H. Four cases of arthritis associated with Mycoplasma pneumoniae infection. Pediatr Int. 2008 Aug. 50(4):511-3. [QxMD MEDLINE Link].
Csábi G, Komáromy H, Hollódy K. Transverse myelitis as a rare, serious complication of Mycoplasma pneumoniae infection. Pediatr Neurol. 2009 Oct. 41(4):312-3. [QxMD MEDLINE Link].
Narita M. Pathogenesis of neurologic manifestations of Mycoplasma pneumoniae infection. Pediatr Neurol. 2009 Sep. 41(3):159-66. [QxMD MEDLINE Link].
Neumayr L, Lennette E, Kelly D, Earles A, Embury S, Groncy P, et al. Mycoplasma disease and acute chest syndrome in sickle cell disease. Pediatrics. 2003 Jul. 112(1 Pt 1):87-95. [QxMD MEDLINE Link].
Wang K, Gill P, Perera R, Thomson A, Mant D, Harnden A. Clinical symptoms and signs for the diagnosis of Mycoplasma pneumoniae in children and adolescents with community-acquired pneumonia. Cochrane Database Syst Rev. 2012 Oct 17. 10:CD009175. [QxMD MEDLINE Link].
Rahimian M, HosseiniB M. Serological study of Bordetella Pertussis, Mycoplasma Pneumonia and Chlamydia Pneumonia in Iranian hajj pilgrims with prolonged cough illnesses: A follow-up study. Respir Med. 2017 Nov. 132:122-131. [QxMD MEDLINE Link].
Kong K, Ding Y, Wu B, Lu M, Gu H. Clinical Predictors of Wheezing Among Children Infected With Mycoplasma Pneumoniae. Front Pediatr. 2021. 9:693658. [QxMD MEDLINE Link].
Cramer L, Emara DM, Gadre AK. Mycoplasma an unlikely cause of bullous myringitis. Ear Nose Throat J. 2012 Jun. 91 (6):E30-1. [QxMD MEDLINE Link].
Mellick LB, Verma N. The Mycoplasma pneumoniae and bullous myringitis myth. Pediatr Emerg Care. 2010 Dec. 26 (12):966-8. [QxMD MEDLINE Link].
Mellick LB, Verma N. The Mycoplasma pneumoniae and bullous myringitis myth. Pediatr Emerg Care. 2010 Dec. 26(12):966-8. [QxMD MEDLINE Link].
Kotikoski MJ, Kleemola M, Palmu AA. No evidence of Mycoplasma pneumoniae in acute myringitis. Pediatr Infect Dis J. 2004 May. 23(5):465-6. [QxMD MEDLINE Link].
Palmu AA, Kotikoski MJ, Kaijalainen TH, Puhakka HJ. Bacterial etiology of acute myringitis in children less than two years of age. Pediatr Infect Dis J. 2001 Jun. 20(6):607-11. [QxMD MEDLINE Link].
Roberts DB. The etiology of bullous myringitis and the role of mycoplasmas in ear disease: a review. Pediatrics. 1980 Apr. 65(4):761-6. [QxMD MEDLINE Link].
Kim SH, Lee E, Song ES, Lee YY. Clinical Significance of Pleural Effusion in Mycoplasma pneumoniae Pneumonia in Children. Pathogens. 2021 Aug 25. 10 (9):[QxMD MEDLINE Link].
Reittner P, Müller NL, Heyneman L, Johkoh T, Park JS, Lee KS, et al. Mycoplasma pneumoniae pneumonia: radiographic and high-resolution CT features in 28 patients. AJR Am J Roentgenol. 2000 Jan. 174(1):37-41. [QxMD MEDLINE Link].
Ma LD, Chen B, Dong Y, Fan J, Xia L, Wang SZ, et al. Rapid mycoplasma culture for the early diagnosis of Mycoplasma pneumoniae infection. J Clin Lab Anal. 2010. 24(4):224-9. [QxMD MEDLINE Link].
Onari S, Okada T, Okada T, Okano S, Kakuta O, Kutsuma H, et al. Immunochromatography test for rapid diagnosis of Mycoplasma pneumoniae infection. Pediatr Int. 2017 Oct. 59 (10):1123-1125. [QxMD MEDLINE Link].
Song M, Zhang Y, Li S, Zhang C, Tao M, Tang Y, et al. A sensitive and rapid immunoassay for Mycoplasma pneumoniae in children with pneumonia based on single-walled carbon nanotubes. Sci Rep. 2017 Nov 27. 7 (1):16442. [QxMD MEDLINE Link].
Dumke R, Strubel A, Cyncynatus C, Nuyttens H, Herrmann R, Lück C, et al. Optimized serodiagnosis of Mycoplasma pneumoniae infections. Diagn Microbiol Infect Dis. 2012 Jun. 73(2):200-3. [QxMD MEDLINE Link].
Zhao F, Cao B, He LH, et al. Evaluation of a new real-time PCR assay for detection of Mycoplasma pneumoniae in clinical specimens. Biomed Environ Sci. 2012 Feb. 25(1):77-81. [QxMD MEDLINE Link].
Mustafa MI, Al-Marzooq F, How SH, Kuan YC, Ng TH. The use of multiplex real-time PCR improves the detection of the bacterial etiology of community acquired pneumonia. Trop Biomed. 2011 Dec. 28(3):531-44. [QxMD MEDLINE Link].
Di Marco E, Cangemi G, Filippetti M, Melioli G, Biassoni R. Development and clinical validation of a real-time PCR using a uni-molecular Scorpion-based probe for the detection of Mycoplasma pneumoniae in clinical isolates. New Microbiol. 2007 Oct. 30(4):415-21. [QxMD MEDLINE Link].
Gullsby K, Storm M, Bondeson K. Simultaneous detection of Chlamydophila pneumoniae and Mycoplasma pneumoniae by use of molecular beacons in a duplex real-time PCR. J Clin Microbiol. 2008 Feb. 46(2):727-31. [QxMD MEDLINE Link]. [Full Text].
Chen CJ, Hung MC, Kuo KL, Chung JL, Wu KG, Hwang BT, et al. The role of eosinophil cationic protein in patients with Mycoplasma pneumoniae infection. J Chin Med Assoc. 2008 Jan. 71(1):37-9. [QxMD MEDLINE Link].
Llibre JM, Urban A, Garcia E, Carrasco MA, Murcia C. Bronchiolitis obliterans organizing pneumonia associated with acute Mycoplasma pneumoniae infection. Clin Infect Dis. 1997 Dec. 25(6):1340-2. [QxMD MEDLINE Link].
Nagashima M, Higaki T, Satoh H, Nakano T. Cardiac thrombus associated with Mycoplasma pneumoniae infection. Interact Cardiovasc Thorac Surg. 2010 Dec. 11(6):849-51. [QxMD MEDLINE Link].
Li CM, Gu L, Yin SJ, et al. Age-specific Mycoplasma pneumoniae pneumonia-associated myocardial damage in children. J Int Med Res. 2013 Oct. 41(5):1716-23. [QxMD MEDLINE Link].
Daxboeck F. Mycoplasma pneumoniae central nervous system infections. Curr Opin Neurol. 2006 Aug. 19(4):374-8. [QxMD MEDLINE Link].
Smith R, Eviatar L. Neurologic manifestations of Mycoplasma pneumoniae infections: diverse spectrum of diseases. A report of six cases and review of the literature. Clin Pediatr (Phila). 2000 Apr. 39(4):195-201. [QxMD MEDLINE Link].
Koskiniemi M. CNS manifestations associated with Mycoplasma pneumoniae infections: summary of cases at the University of Helsinki and review. Clin Infect Dis. 1993 Aug. 17 Suppl 1:S52-7. [QxMD MEDLINE Link].
Luby JP. Pneumonia caused by Mycoplasma pneumoniae infection. Clin Chest Med. 1991 Jun. 12(2):237-44. [QxMD MEDLINE Link].
Kurata M, Kano Y, Sato Y, Hirahara K, Shiohara T. Synergistic Effects of Mycoplasma pneumoniae Infection and Drug Reaction on the Development of Atypical Stevens-Johnson Syndrome in Adults. Acta Derm Venereol. 2016 Jan. 96 (1):111-3. [QxMD MEDLINE Link]. [Full Text].
Kaler J, Mukhtar O, Khan B, Shrestha B, Kaler R, Ting B, et al. Rhabdomyolysis: An Unusual Presentation of Mycoplasma pneumoniae Infection in an Adult-A Case Report and Literature Review. Case Rep Med. 2018. 2018:6897975. [QxMD MEDLINE Link].
Khan FY, Sayed H. Rhabdomyolysis associated with Mycoplasma pneumoniae pneumonia. Hong Kong Med J. 2012 Jun. 18(3):247-9. [QxMD MEDLINE Link].
Oishi T, Narita M, Ohya H, et al. Rhabdomyolysis associated with antimicrobial drug-resistant Mycoplasma pneumoniae. Emerg Infect Dis. 2012 May. 18(5):849-51. [QxMD MEDLINE Link]. [Full Text].
Moon HJ, Yang JK, In DH, Kwun DH, Jo HH, Chang SH. A Case of a 14-year-old Girl Who Developed Dermatomyositis Associated with Mycoplasma pneumonia Infection. Soonchunhyang Med Sci. December 2015. 21:130-33. [Full Text].
Liu EM, Janigian RH. Mycoplasma pneumoniae: the other masquerader. JAMA Ophthalmol. 2013 Feb. 131(2):251-3. [QxMD MEDLINE Link].
Smith LG. Mycoplasma pneumonia and its complications. Infect Dis Clin North Am. 2010 Mar. 24(1):57-60. [QxMD MEDLINE Link].
Biondi E, McCulloh R, Alverson B, Klein A, Dixon A. Treatment of mycoplasma pneumonia: a systematic review. Pediatrics. 2014 Jun. 133(6):1081-90. [QxMD MEDLINE Link].
Colin AA, Yousef S, Forno E, Korppi M. Treatment of Mycoplasma pneumoniae in pediatric lower respiratory infection. Pediatrics. 2014 Jun. 133(6):1124-5. [QxMD MEDLINE Link].
Cardinale F, Chironna M, Chinellato I, Principi N, Esposito S. Clinical relevance of Mycoplasma pneumoniae macrolide resistance in children. J Clin Microbiol. 2013 Feb. 51(2):723-4. [QxMD MEDLINE Link]. [Full Text].
Kawai Y, Miyashita N, Kubo M, et al. Therapeutic efficacy of macrolides, minocycline, and tosufloxacin against macrolide-resistant Mycoplasma pneumoniae pneumonia in pediatric patients. Antimicrob Agents Chemother. 2013 May. 57(5):2252-8. [QxMD MEDLINE Link]. [Full Text].
Uh Y, Hong JH, Oh KJ, et al. Macrolide resistance of Mycoplasma pneumoniae and its detection rate by real-time PCR in primary and tertiary care hospitals. Ann Lab Med. 2013 Nov. 33(6):410-4. [QxMD MEDLINE Link]. [Full Text].
Centers for Disease Control and Prevention. Mycoplasma pneumoniae Infection Surveillance and Trends. Available at https://www.cdc.gov/mycoplasma/php/surveillance/index.html. February 16, 2024; Accessed: June 22, 2024.
Pereyre S, Goret J, Bébéar C. Mycoplasma pneumoniae: Current Knowledge on Macrolide Resistance and Treatment. Front Microbiol. 2016. 7:974. [QxMD MEDLINE Link].
Todd SR, Dahlgren FS, Traeger MS, Beltrán-Aguilar ED, Marianos DW, Hamilton C, et al. No visible dental staining in children treated with doxycycline for suspected Rocky Mountain Spotted Fever. J Pediatr. 2015 May. 166 (5):1246-51. [QxMD MEDLINE Link]. [Full Text].
Leal SM Jr, Totten AH, Xiao L, Crabb DM, Ratliff A, Duffy LB, et al. Evaluation of Commercial Molecular Diagnostic Methods for Detection and Determination of Macrolide Resistance in Mycoplasma pneumoniae. J Clin Microbiol. 2020 May 26. 58 (6):[QxMD MEDLINE Link].
Zhao H, Yan C, Feng Y, Du B, Feng J, Cui X, et al. Absolute quantification of Mycoplasma pneumoniae in infected patients by droplet digital PCR to track disease severity and treatment efficacy. Front Microbiol. 2023. 14:1177273. [QxMD MEDLINE Link].
Ishiguro N, Sato R, Mori T, Tanaka H, Narita M, Nagano T, et al. Point-of-care molecular diagnosis of Mycoplasma pneumoniae including macrolide sensitivity using quenching probe polymerase chain reaction. PLoS One. 2021. 16 (10):e0258694. [QxMD MEDLINE Link].
Kim CH, Lee J. Mycoplasma pneumoniae Pleural Effusion in Adults. J Clin Med. 2022 Feb 26. 11 (5):[QxMD MEDLINE Link].
[Guideline] Metlay JP, Waterer GW, Long AC, Anzueto A, Brozek J, Crothers K, et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019 Oct 1. 200 (7):e45-e67. [QxMD MEDLINE Link]. [Full Text].
[Guideline] Centers for Disease Control and Prevention. Clinical Care of Mycoplasma pneumoniae Infection. Available at https://www.cdc.gov/mycoplasma/hcp/clinical-care/?CDC_AAref_Val=https://www.cdc.gov/pneumonia/atypical/mycoplasma/hcp/antibiotic-treatment-resistance.html. December 27, 2023; Accessed: June 22, 2024.
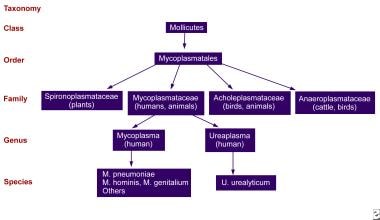 Diagram of the Mollicutes class, to which the Mycoplasma genus belongs.
Diagram of the Mollicutes class, to which the Mycoplasma genus belongs.







