Background
Breast masses are broadly classified as benign or malignant. Common causes of benign breast lesions include fibrocystic disease, fibroadenoma, intraductal papilloma, and abscess. Malignant breast disease encompasses many histologic types that include, but are not limited to, in situ ductal or lobular carcinoma, infiltrating ductal or lobular carcinoma, and inflammatory carcinoma. The main concern of many women presenting with a breast mass is the likelihood of cancer. Reassuringly, most breast masses are benign.
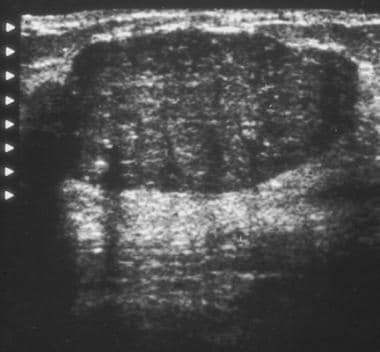 Ultrasonogram demonstrates a hypoechoic mass with smooth, partially lobulated margins typical of a fibroadenoma.
Ultrasonogram demonstrates a hypoechoic mass with smooth, partially lobulated margins typical of a fibroadenoma.
See Breast Lumps in Young Women: Diagnostic Approaches, a Critical Images slideshow, to help identify and manage palpable breast lumps in young women.
Breast infections are divided into lactational and non-lactational infections and puerperal versus nonpuerperal, depending on their association with pregnancy. The process may be confined to the skin overlying the breast, or it may result from an underlying lesion (eg, sebaceous cyst), as in hidradenitis suppurativa. [1, 2, 3, 4]
Pathophysiology
The mammary glands arise from a caudal section of the ectodermal tissue known as the “milk lines,” which extend along the anterior surface of the developing fetus from the axilla to the groin. During puberty, pituitary and ovarian hormonal influences stimulate female breast enlargement, primarily owing to accumulation of adipocytes. Each breast contains approximately 15-25 glandular units known as breast lobules, which are demarcated by Cooper ligaments. Each lobule is composed of a tubuloalveolar gland and adipose tissue. Each lobule drains into the lactiferous duct, which subsequently empties onto the surface of the nipple. Multiple lactiferous ducts converge to form one ampulla, which traverses the nipple to open at the apex. [5]
Below the nipple surface, lactiferous ducts form large dilations called lactiferous sinuses, which act as milk reservoirs during lactation. [6] When the lactiferous duct lining undergoes epidermalization, keratin production may cause plugging of the duct, resulting in abscess formation. [7, 8] This may explain the high recurrence rate (an estimated 39%-50%) of breast abscesses in patients treated with standard incision and drainage, as this technique does not address the basic mechanism by which breast abscesses are thought to occur.
Postpartum mastitis is a localized cellulitis caused by bacterial invasion through an irritated or fissured nipple. It typically occurs after the second postpartum week and may be precipitated by milk stasis. [9] There is usually a history of a cracked nipple or skin abrasion or failure to clean nipples after breastfeeding. [10] Sleeping position may also affect the progression of mastitis to breast abscess. [10] Staphylococcus aureus is the most common organism responsible, but Staphylococcus epidermidis and streptococci are occasionally isolated. Drainage of milk from the affected segment should be encouraged and is best achieved by continued breastfeeding or use of a breast pump. [3, 8, 4]
Nonlactating infections may be divided into central (periareolar) and peripheral breast lesions. Periareolar infections consist of active inflammation around nondilated subareolar breast ducts—a condition termed periductal mastitis. Peripheral nonlactating breast abscesses are less common than periareolar abscesses and are often associated with an underlying condition such as diabetes, rheumatoid arthritis, steroid treatment, granulomatous lobular mastitis, trauma, and smoking. [1, 11, 12] Primary skin infections of the breast (cellulitis or abscess) most commonly affect the skin of the lower half of the breast and often recur in women who are overweight, have large breasts, or have poor personal hygiene. [3]
Breast masses can involve any of the tissues that make up the breast, including overlying skin, ducts, lobules, and connective tissues. Fibrocystic disease, the most common breast mass in women, is found in 60%-90% of breasts during routine autopsy. Fibroadenoma, the most common benign tumor, typically affects women aged 30 years or younger and accounts for 91% of all solid breast masses in females younger than 19 years. [5] Infiltrating ductal carcinoma is the most common malignant tumor; however, inflammatory carcinoma is the most aggressive and carries the worst prognosis. Mammary Paget disease, or adenocarcinoma of the nipple epidermis, is relatively rare but may be misdiagnosed as a benign dermatosis if care is not taken. [13, 14]
Epidemiology
Frequency
Statistics provided refer to populations in the United States.
After skin cancer, breast cancer is the most commonly diagnosed cancer in women, accounting for roughly 1 in 4 cancers diagnosed and affecting 12.4% of women during their lifetime. [15]
Breast infections occur in as many as 10%-33% of lactating women. [16, 17]
Lactational mastitis is seen in approximately 2%-3% of lactating women, [6, 18, 4] and breast abscess may develop in 5%-11% of women with mastitis. [18, 4]
Mortality/Morbidity
Breast mass
Morbidity and mortality depends on etiology (benign vs malignant) and stage of malignant lesions.
Approximately 2.1%-3.6% of women die of breast cancer. In 2009, approximately 40,170 women were expected to die from breast cancer, [15] remaining stable at 40,610 in 2017, just behind lung and colon cancer.
Despite significant differences in sociodemographic and clinical characteristics, overall and disease-free survival rates are similar for men and women with breast cancer. [19, 20]
Associated morbidity may include scarring, disfigurement, lymphedema, and psychologic stress.
Breast abscess
Recurrent or chronic infections, pain, and scarring are causes of morbidity.
Mastitis is usually seen in lactating women, but the presence in a nonlactating woman should spur evaluation for an inflammatory carcinoma, newly onset diabetes, infection withMycobacterium tuberculosis, and other idiopathic causes. [3, 12]
Abscess formation complicates postpartum mastitis in fewer than 10% of cases.
Neonatal mastitis usually occurs in term or near-term infants, is twice as common in females, and progresses to development of a breast abscess in approximately 50% of cases. [21, 22, 5]
Development of mastitis has been correlated with an increased risk of developing breast cancer. [23, 24]
Race
While white women have a higher incidence of breast cancer than African American women after age 40 years, African American women have a higher incidence of early breast cancer (before age 40 years) and are more likely to die of breast cancer at every age. [25]
African-American women have been variably reported to have an increased incidence of developing a primary breast abscess. [26, 27]
Sex
Approximately 99% of breast cancers are found in women.
Up to 1% of breast cancers occur in men, but numbers have been increasing. [19, 28] Men with changes in breast size should undergo as aggressive of a diagnostic workup as women. [21, 22, 29, 30] Because of the high rate of hormone estrogen receptor positivity in male patients, hormonal therapy is a treatment mainstay for many men.
Since the indications and outcomes of biopsies in trans women have been observed to be similar to those in cis women, it seems reasonable to follow breast care guidelines as developed for cis women. [31]
Age
Lumps or breast masses are the most frequent breast pathology in adolescence, but malignancy is extremely rare in this age group. [32] Fibroadenoma, a benign condition, is the most common cause of breast mass in women younger than 35 years. [5]
In 2017, women aged 40 years or older accounted for nearly 96% of new breast cancer diagnoses and 98% of breast cancer deaths.
The median age at breast cancer diagnosis is 62 years.
Breast infections most commonly affect women aged 18-50 years. [3]
Nonpuerperal breast masses encompass a wider range of ages, from the late second to eighth decade of life. Peak incidence is often in the fourth decade of life. Ninety-five percent of these infections occur in women. [8]
Puerperal breast abscesses and mastitis are commonly found in women of childbearing age (mean age of 32 years). [1]
Non-neonatal pediatric breast abscess bacteriology is similar to other skin abscesses. [33]
Access to care
Women who reside in rural settings may be more likely to present with a more advanced cancer stage than women in urban settings. This may partly result from the availability of and access to effective screening tools and primary care. [34]
Prognosis
Breast mass: Prognosis varies from excellent in patients with a fibroadenoma to poor in those with inflammatory breast cancer. Influencing factors include tumor size, histology, nodal involvement, distant metastases, and comorbid conditions.
Breast abscess: Unfortunately, the recurrence rate of breast abscess is high (39%-50%) when treated with standard incision and drainage, and studies have shown even higher recurrence rates in women undergoing fine-needle aspiration. [35] Nonpuerperal abscesses recur more frequently, especially when associated with non-staphylococcal species (>50% recurrence rate). [8] Studies of patients with fistulectomy show lower recurrence rates.
Mastitis: Most patients experience resolution within 2 to 3 weeks. All patients with symptoms that have not resolved within 5 weeks should be evaluated for resistant infection or malignancy.
Patient Education
Educate women who are lactating on nipple hygiene because cracking and abrasions of the skin increase risk of infection.
For excellent patient education resources, visit eMedicineHealth's Women's Health Center and Cancer Center. Also, see eMedicineHealth's patient education articles Breast Infection, Breast Lumps and Pain, Breast Self-Exam, and Breast Cancer.
-
Ultrasonogram demonstrates a hypoechoic mass with smooth, partially lobulated margins typical of a fibroadenoma.
-
Craniocaudal mammograms obtained 1 year apart demonstrate a newly developing mass in the outer part of the breast.
-
Spot compression mammogram of the outer part of the breast demonstrates a new mass as smooth, margined, and oval. The findings are consistent with a fibroadenoma, a cyst, or a malignancy. In this patient, the diagnosis was a rapidly growing fibroadenoma.
-
Eggshell or rim calcifications (arrows) have walls thinner than those of lucent-centered calcifications.
-
This mass with associated large, coarse calcifications (arrows) is a degenerating fibroadenoma.
-
Breast cancer, ultrasonography. Mediolateral oblique digital mammogram of the right breast in a 66-year-old woman with a new, opaque, irregular mass approximately 1 cm in diameter. The mass has spiculated margins in the middle third of the right breast at the 10-o'clock position. Image demonstrates both the spiculated mass (black arrow) and separate anterior focal asymmetry (white arrow).
-
Breast cancer, ultrasonography. Antiradial sonogram of the spiculated mass (shown in the image above) demonstrates a hypoechoic mass with angular margins (black arrows). Cursors on the margins of the mass were used to electronically measure its dimensions of the mass, which was 0.9 X 0.8 cm.
-
Breast cyst. A) A simple, fairly round breast cyst with hypo or anechoic contents and well-defined borders; B) Posterior acoustic enhancement is seen as well as edge shadows (arrows).
-
Breast adenoma. A) A breast adenoma is oval with well-defined borders. It may be hypoechoic and some internal echogenicity may be seen. It is wider than tall and posterior acoustic enhancement is NOT seen, helping distinguish from a cyst or other fluid collection. B) An arrow indicates the adenoma.
-
Breast hematoma. A) A breast hematoma is seen as a round echogenic collection with surrounding tissue edema. A hematoma may be hypoechoic, mixed, or fairly echogenic depending on the stage of the hematoma. B) The hematoma is outlined and tissue edema noted.
-
Loculated breast abscess. A) A large loculated abscess is seen containing hypoechoic fluid and some internal echoes. Posterior acoustic enhancement is seen. Care must be taken to image at an adequate depth to visualize posterior borders of breast lesions. B) The abscess is outlined in yellow and the posterior acoustic enhancement is noted.
-
Loculated breast abscess, curvilinear. A) This is the same abscess seen in the above image and is imaged with a curvilinear transducer to better appreciate the extent of the abscess. It is important to image the abscess completely for width and depth. B) The abscess is outlined in yellow and the ribs and posterior acoustic enhancement are noted.
-
Purulent breast abscess. A) A purulent breast abscess is seen. The fluid is echogenic, but can be recognized as a disruption of the surrounding tissue and posterior acoustic enhancement. B) The abscess is outlined in yellow and the posterior acoustic enhancement is noted.
-
Complex breast abscess. In this clip, the features of a loculated breast abscess containing echogenic purulent material are noted. Example of imaging with a linear high-frequency transducer.
-
Loculated breast abscess, curvilinear. In this clip, a large, loculated breast abscess and its features are noted. Example of imaging with a lower-frequency curvilinear transducer to better appreciate the extent of this large abscess.
Tables

What would you like to print?
- Are Interval Breast Cancer Diagnoses Increasing?
- ACOG Updates Breast Cancer Screening Guidelines
- Should Genetic Testing Be Routine for Breast Cancer?
-
 Can the Use of ADCs in Breast Cancer Teach Us About Resistance Mechanisms and Sequencing in Endometrial Cancer?
Can the Use of ADCs in Breast Cancer Teach Us About Resistance Mechanisms and Sequencing in Endometrial Cancer?
-
ESMO Breast Cancer 2025
-
ADC Therapies for Endocrine-Resistant HR+ Metastatic Breast Cancer





