Practice Essentials
Urinary incontinence is an underdiagnosed and underreported problem that increases with age, affecting 38-55% of women older than 60 years [1] and 50-84% of the elderly in long-term care facilities. [2] At any age, urinary incontinence is more than twice as common in females than in males. [3]
Signs and symptoms
Types of urinary incontinence
-
Urge: Involuntary leakage accompanied by or immediately preceded by urgency (often referred to as an overactive bladder)
-
Mixed: A combination of stress and urge incontinence, marked by involuntary leakage associated with urgency and also with exertion, effort, sneezing, or coughing
-
Functional: The inability to hold urine due to reasons other than neuro-urologic and lower urinary tract dysfunction (eg, delirium, psychiatric disorders, urinary infection, impaired mobility)
See Presentation for more detail.
Diagnosis
Patients with urinary incontinence should undergo a basic evaluation that includes a history, physical examination, and urinalysis. In selected patients, the following may also be needed:
-
Voiding diary
-
Cotton swab test (optional)
-
Cough stress test
-
Measurement of postvoid residual (PVR) urine volume
-
Cystoscopy
-
Urodynamic studies (see the image below)
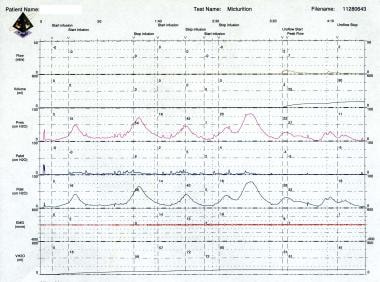 Urinary incontinence. Urodynamic study revealing detrusor instability in a 75-year-old man with urge incontinence. Note the presence of multiple uninhibited detrusor contractions (phasic contractions) that is generating 40- to 75-cm H2O pressure during the filling cystometrogram (CMG). He also has small bladder capacity (81 mL), which is indicative of poorly compliant bladder.
Urinary incontinence. Urodynamic study revealing detrusor instability in a 75-year-old man with urge incontinence. Note the presence of multiple uninhibited detrusor contractions (phasic contractions) that is generating 40- to 75-cm H2O pressure during the filling cystometrogram (CMG). He also has small bladder capacity (81 mL), which is indicative of poorly compliant bladder.
Videourodynamic studies are reserved to evaluate complex cases of stress urinary incontinence. Videourodynamic studies combine the radiographic findings of a voiding cystourethrogram and multichannel urodynamics. Go to Urodynamic Studies for Urinary Incontinence for more information on this topic.
The following points regarding the clinical presentation should be sought when obtaining the history:
-
Severity and quantity of urine lost and frequency of incontinence episodes
-
Duration of the complaint and whether problems have been worsening
-
Triggering factors or events (eg, cough, sneeze, lifting, bending, feeling of urgency, sound of running water, sexual activity/orgasm)
-
Constant versus intermittent urine loss
-
Associated frequency, urgency, dysuria, pain with a full bladder
-
History of urinary tract infections (UTIs)
-
Concomitant fecal incontinence or pelvic organ prolapse
-
Coexistent complicating or exacerbating medical problems
-
Obstetrical history, including difficult deliveries, grand multiparity, forceps use, obstetrical lacerations, and large babies
-
History of pelvic surgery, especially prior incontinence procedures, hysterectomy, or pelvic floor reconstructive procedures
-
Other urologic procedures
-
Spinal and central nervous system surgery
-
Lifestyle issues, such as smoking, alcohol or caffeine abuse, and occupational and recreational factors causing severe or repetitive increases in intra-abdominal pressure
-
Medications
Relevant complicating or exacerbating medical problems may include the following:
-
Chronic cough
-
Chronic obstructive pulmonary disease (COPD)
-
Congestive heart failure
-
Diabetes mellitus
-
Obesity
-
Connective tissue disorders
-
Postmenopausal hypoestrogenism
-
CNS or spinal cord disorders
-
Chronic UTIs
-
Urinary tract stones
-
Benign prostatic hyperplasia
-
Cancer of pelvic organs
Medications that may be associated with urinary incontinence include the following:
-
Cholinergic or anticholinergic drugs
-
Alpha-blockers
-
Over-the-counter allergy medications
-
Estrogen replacement
-
Beta-mimetics
-
Sedatives
-
Muscle relaxants
-
Diuretics
-
Angiotensin-converting enzyme (ACE) inhibitors
See Workup for more detail.
Management
Successful treatment of urinary incontinence must be tailored to the specific type of incontinence and its cause. The usual approaches are as follows:
-
Stress incontinence: Pelvic floor physiotherapy, anti-incontinence devices, and surgery
-
Urge incontinence: Changes in diet, behavioral modification, pelvic-floor exercises, medications, and/or therapies such as onabotulinum toxin injections and neuromodulation therapies.
-
Mixed incontinence: Pelvic floor physical therapy, anticholinergic drugs, and surgery
-
Overflow incontinence: Catheterization regimen or diversion
-
Functional incontinence: Treatment of the underlying cause
Absorbent products may be used temporarily until a definitive treatment has a chance to work, in patients awaiting surgery, or long-term under the following circumstances:
-
Persistent incontinence despite all appropriate treatments
-
Inability to participate in behavioral programs, due to illness or disability
-
Presence of an incontinence disorder that cannot be helped by medications
-
Presence of an incontinence disorder that cannot be corrected by surgery
In stress and urge urinary incontinence, the following medications may provide some benefit:
-
Anticholinergic agents
-
Antispasmodic drugs
-
Beta-adrenergic agonists
-
Tricyclic antidepressants
-
Estrogen
-
Botulinum toxin
Surgical care for stress incontinence involves procedures that increase urethral outlet resistance, including the following:
-
Bladder neck suspension
-
Periurethral bulking therapy
-
Midurethral slings
-
Artificial urinary sphincter
The transobturator male sling may be of particular benefit to men who experience stress incontinence after prostatectomy. [6] Transobturator vaginal tape (TVT-O) is widely used for stress incontinence in women [7] . Please realize this is not available, there are other commercial options.
Surgical care for urge incontinence involves procedures that improve bladder overactivity or bladder capacity, including the following:
-
Sacral nerve modulation
-
Tibial nerve stimulation
-
Injection of neurotoxins such as botulinum toxin
-
Bladder augmentation
See Treatment and Medication for more detail.
For patient education information, see Urinary Incontinence, Bladder Control Problems, and Understanding Bladder Control Medications, .
Background
Urinary incontinence is defined by the International Continence Society as the involuntary loss of urine that represents a hygienic or social problem to the individual. [8] Urinary incontinence can be thought of as a symptom as reported by the patient, as a sign that is demonstrable on examination, and as a disorder.
Urinary incontinence should not be thought of as a disease, because no specific etiology exists; most individual cases are likely multifactorial in nature. The etiologies of urinary incontinence are diverse and, in many cases, incompletely understood.
Types of urinary incontinence
Four types of urinary incontinence are defined in the Clinical Practice Guideline issued by the Agency for Health Care Policy and Research: stress, urge, mixed, and overflow. Some authors include functional incontinence as a fifth type of incontinence. [9, 10, 5]
Stress incontinence is characterized by urine leakage associated with increased abdominal pressure from laughing, sneezing, coughing, climbing stairs, or other physical stressors on the abdominal cavity and, thus, the bladder. [4, 5] Urge urinary incontinence is involuntary leakage accompanied by or immediately preceded by urgency. Mixed urinary incontinence is a combination of stress and urge incontinence; it is marked by involuntary leakage associated with urgency and also with exertion, effort, sneezing or coughing.
Functional incontinence is the inability to hold urine due to reasons other than neuro-urologic and lower urinary tract dysfunction.
Other terms describing urinary incontinence are as follows:
-
Enuresis - Involuntary loss of urine
-
Nocturnal enuresis - Loss of urine occurring during sleep
-
Continuous urinary incontinence - Continuous leakage
Successful treatment of urinary incontinence must be tailored to the specific type of incontinence and its cause (see Treatment). The usual approaches are as follows:
-
Stress incontinence - Pelvic floor physiotherapy, anti-incontinence devices, and surgery
-
Urge incontinence - Changes in diet, behavioral modification, pelvic-floor exercises, and/or medications and new forms of procedural intervention
-
Mixed incontinence - Pelvic floor physical therapy, anticholinergic or beta-3 agonists drugs, and surgery
-
Overflow incontinence - Catheterization regimen or diversion
-
Functional incontinence - Treatment of the underlying cause
Historical context
Urinary incontinence in women is not a recent medical and social phenomenon, but the relative importance attributed to urinary incontinence as a medical problem is increasing. Several factors responsible for the increased attention to incontinence can be cited.
First, women are more willing to talk openly about this disorder. Women are realizing that, in most cases, urinary incontinence is a treatable condition. Consequently, less embarrassment and fewer social stigmas are associated with the diagnosis.
Second, as the population ages, incontinence becomes a more frequent concern. Urinary incontinence often is the chief reason for institutionalization of elderly people.
Third, interest in urinary incontinence disorders within the medical community is surging. This increased interest is arising among basic scientists, clinical researchers, and clinicians. The subspecialties of urogynecology and female urology are emerging, and structured fellowships are in the credentialing process. A Female Pelvic Medicine and Reconstructive Surgery fellowship is now accredited as a subspecialty by the American Board of Obstetrics and Gynecology (ABOG) and the American Board of Urology (ABU).
As a direct result of this increased interest, the public is becoming more aware of the problem and more active and educated about incontinence. Patient advocacy groups provide patients access to information, incontinence products, and physicians who have interest or special expertise in these disorders. In the last decade, funding opportunities for incontinence research have increased vastly. Subspecialty professional organizations and journals are now active.
Important contributions to the understanding of the structure and functioning of the lower urinary tract include an improved understanding of the anatomy and dynamic functioning of the pelvic floor and its contribution to continence. In addition, much study has been conducted to bolster the understanding of the neurophysiology of the bladder, urethra, and pelvic floor. Finally, interest in the diagnosis and treatment of incontinence is ongoing.
An estimated 50-70% of women with urinary incontinence fail to seek medical evaluation and treatment because of social stigma. Only 5% of individuals who are incontinent and 2% of nursing home residents who are incontinent receive appropriate medical evaluation and treatment. Patients who are incontinent often cope with this condition for 6-9 years before seeking medical therapy.
In a 1997 survey of primary care physicians, about 40% reported that they sometimes, rarely, or never ask patients about incontinence. More than 40% of internists and family practitioners routinely recommended absorbent pads to their patients as a solution to incontinence disorders. [11] Continued education of the public and medical professionals is needed to improve the care rendered to individuals with urinary incontinence.
In 1989, the National Institutes of Health Consensus Development Conference estimated the annual cost of urinary incontinence in the United States to be $12.4 billion. Some experts believe that this is a conservative estimate. True costs can be difficult to estimate because many individuals do not come to the attention of medical specialists.
A 2009 survey of women in a managed care population found that the prevalence of undiagnosed urinary incontinence was 53% in the preceding year. [12] Some individuals pay out of pocket for adult incontinence undergarments, absorbable pads, skin care products, deodorants, and increased laundry expenses.
The psychosocial costs and morbidities are even more difficult to quantify. Embarrassment and depression are common. The affected individual may experience a decrease in social interactions, excursions out of the home, and sexual activity.
The psychosocial impact on at-home caregivers, spouses, or family members rarely is considered. Kelleher et al developed a questionnaire to assess the quality of life of women with incontinence. [13] This questionnaire has proven to be easy to use, valid, and reliable. This tool may be a valuable adjunct to pretherapy and posttherapy assessment, as well as valuable in comparing the quality of life impact of different urodynamic diagnoses.
Several other questionnaires are available for urge incontinence, stress incontinence, and quality of life. Many have been validated in many languages, presurgery and postsurgery. The questionnaires most often used are the Urinary Distress Inventory (UDI)–6, Incontinence Quality of Life (IQoL) Questionnaire, Incontinence Impact Questionnaire (IIQ)–7, UDI, Overactive Bladder Symptom and Health-Related Questionnaire (OAB-Q), and King’s Health Questionnaire KHQ). [14]
Anatomy
For understanding urinary incontinence, the relevant anatomy of the lower urinary tract comprises the urethra and bladder. Go to Urinary Incontinence Relevant Anatomy for more information on this topic.
Pathophysiology
Micturition requires coordination of several physiological processes. Somatic and autonomic nerves carry bladder volume input to the spinal cord, and motor output innervating the detrusor, sphincter, and bladder musculature is adjusted accordingly. The cerebral cortex exerts a predominantly inhibitory influence, whereas the brainstem facilitates urination by coordinating urethral sphincter relaxation and detrusor muscle contraction.
As the bladder fills, sympathetic tone contributes to closure of the bladder neck and relaxation of the dome of the bladder and inhibits parasympathetic tone. At the same time, somatic innervation maintains tone in the pelvic floor musculature as well as the striated periurethral muscles.
When urination occurs, sympathetic and somatic tones in the bladder and periurethral muscles diminish, resulting in decreased urethral resistance. Cholinergic parasympathetic tone increases, resulting in bladder contraction. Urine flow results when bladder pressure exceeds urethral resistance. Normal bladder capacity is 300-500 mL, and the first urge to void generally occurs between bladder volumes of 150 and 300 mL.
Incontinence occurs when micturition physiology, functional toileting ability, or both have been disrupted. [10] The underlying pathology varies among the different types of incontinence (ie, stress, urge, mixed, reflex, overflow, and functional incontinence).
Stress incontinence pathophysiology
During episodes of stress incontinence, an increase in intra-abdominal pressure (eg, from laughing, sneezing, coughing, climbing stairs) raises pressure within the bladder to the point where it exceeds the urethra’s resistance to urinary flow. [4, 5] Leakage ceases when bladder pressure again falls below urethral pressure.
The major cause of stress incontinence is urethral hypermobility due to impaired support from pelvic floor. A less common cause is an intrinsic sphincter deficiency, usually secondary to pelvic surgeries. In either case, urethral sphincter function is impaired, resulting in urine loss at lower than usual abdominal pressures.
In women with stress urinary incontinence, either or both mechanisms may be present, although some authors hold that stress incontinence does not develop in patients with poor pelvic support unless intrinsic sphincter deficiency is also present. Intrinsic sphincter deficiency, resulting from loss of function of both the internal and the external sphincter mechanism, is the only cause of stress incontinence in males.
Urethral hypermobility
Urethral hypermobility is related to impaired neuromuscular functioning of the pelvic floor coupled with injury, both remote and ongoing, to the connective tissue supports of the urethra and bladder neck. When this occurs, the proximal urethra and the bladder neck descend to rotate away and out of the pelvis at times of increased intra-abdominal pressure.
Because the bladder neck and proximal urethra move out of the pelvis, more pressure is transmitted to the bladder. During this process, the posterior wall of the urethra shears off the anterior urethral wall to open the bladder neck when intrinsic sphincter deficiency is present.
In women without urethral hypermobility, the urethra is stabilized during stress by three interrelated mechanisms. One mechanism is reflex, or voluntary, closure of the pelvic floor. Contraction of the levator ani complex elevates the proximal urethra and bladder neck, tightens intact connective tissue supports, and elevates the perineal body, which may serve as a urethral backstop.
The second mechanism involves intact connective tissue support to the bladder neck and urethra. The pubocervicovesical or anterior endopelvic connective tissue in the area of the bladder neck is attached to the back of the pubic bone, the arcus tendineus fascia pelvis, and the perineal membrane. The pubourethral ligaments also suspend the middle portion of the urethra to the back of the pubic bone.
These connective-tissue components form the passive supports to the urethra and bladder neck. During times of increased intra-abdominal pressure, if these supports are intact, they augment the supportive effect of muscular closure of the pelvic floor.
The third mechanism involves 2 bundles of striated muscle, the urethrovaginal sphincter and the compressor urethrae, found at the distal aspect of the striated urethral sphincter. These muscles may aid in compressing the urethra shut during stress maneuvers. These muscles do not surround the urethra, as the striated sphincter does, but lie along the lateral and ventral aspects.
The exact function and importance of these muscles are controversial. Some authors suggest that the urethrovaginal sphincter and the compressor urethrae may provide compression and increased pressure in the distal urethra during times of stress.
Damage to the nerves, muscle, and connective tissue of the pelvic floor is important in the genesis of stress incontinence. Injury during childbirth probably is the most important mechanism. Aging, hypoestrogenism, chronic connective tissue strain due to primary loss of muscular support, activities or medical conditions resulting in long-term repetitive increases in intra-abdominal pressure, and other factors can contribute.
During childbirth, 3 types of lesions can occur: levator ani muscle tears, connective tissue breaks, and pudendal/pelvic nerve denervation. Any of these injuries can occur in isolation but 2 or more in combination are more likely to occur. The long-term result may be the loss of active and passive urethral support and loss of intrinsic urethral tone.
The loss of urethral and bladder neck support may impair urethral closure mechanisms during times of increased intra-abdominal pressure. This phenomenon can be viewed in several ways.
Some hypothesize that under normal circumstances, any increase in intra-abdominal pressure is transmitted equally to the bladder and proximal urethra. This is likely due to the retropubic location of the proximal and mid urethra within the sphere of intra-abdominal pressure. At rest, the urethra has a higher intrinsic pressure than the bladder. This pressure gradient relationship is preserved if acute increases in intra-abdominal pressure are transmitted equally to both organs.
When the urethra is hypermobile, pressure transmission to the walls of the urethra may be diminished as it descends and rotates under the pubic bone. Intraurethral pressure falls below bladder pressure, resulting in urine loss.
A related way of describing the mechanism of hypermobility-related stress incontinence is the hammock theory posited by DeLancey. [15] Normally, an acute increase in intra-abdominal pressure applies a downward force to the urethra. The urethra is then compressed shut against the firm support provided by the anterior vaginal wall and associated endopelvic connective tissue sheath. If the endopelvic connective tissue is detached from its normal lateral fixation points at the arcus tendineus fascia pelvis, optimal urethral compression does not take place.
A simple analogy is that of a garden hose (urethra) running over a pavement surface (anterior endopelvic connective tissue). A force is applied in a downward direction using the foot (increased intra-abdominal pressure). This force compresses the hose shut, occluding flow. If the same hose is run through a soft area of mud (damaged connective tissue), then the downward force does not occlude the hose but, rather, pushes the hose deeper into the mud.
An alternative theory of the mechanism of stress incontinence stems from research involving ultrasound visualization of the bladder neck and proximal urethra during stress maneuvers. This research found that 93% of patients with stress incontinence displayed funneling of the proximal urethra with straining, and half of those individuals also showed funneling at rest. [16] In addition, during stress maneuvers, the urethra did not rotate and descend as a single unit; rather, the posterior urethral wall moved farther than the anterior wall.
Although mobile, the anterior urethral wall has been observed to stop moving, as if tethered, while the posterior wall continued to rotate and descend. Possibly, the pubourethral ligaments arrest rotational movement of the anterior wall but not the posterior wall. The resulting separation of the anterior and posterior urethral walls might open the proximal urethral lumen, thus allowing or contributing to stress incontinence.
Intrinsic sphincter deficiency
Intrinsic sphincter deficiency is a condition in which the urethral sphincter is unable to coapt and generate enough resting urethral closing pressure to retain urine in the bladder. The anatomic support of the urethra may be normal.
Intrinsic sphincter deficiency is due to devascularization and/or denervation of the bladder neck and proximal urethra. The urethral sphincter may become weak after pelvic surgery (eg, failed bladder suspension surgery) because of nearby nerve damage or excessive scarring of the urethra and surrounding tissues. Additional causes of urethral dysfunction include pelvic radiation or neurologic injury, including myelomeningocele.
Women with severe intrinsic sphincter deficiency do not always have the usual urethral hypermobility during a Valsalva maneuver. Paradoxically, the urethra appears well supported. This results in so-called lead pipe urethra, where the urethra remains open at rest. Whenever intra-abdominal pressure exceeds proximal urethral pressure, involuntary urine loss ensues. Because the urethra cannot remain closed, the patient experiences almost continuous urinary incontinence.
Female urethral function is influenced by estrogen. The lack of estrogen at menopause leads to atrophy and replacement of submucosa (ie, vascular plexus) by fibrous tissue. When estrogen is administered to postmenopausal women with atrophic vaginitis, the mucosa regains its turgor, with simultaneous up-regulation of alpha-receptors and angiogenesis of vascular plexus. Lack of estrogen is a risk factor for developing intrinsic sphincter deficiency, but estrogen replacement may reverse its effects. (Although it should be noted estrogen therapy is controversial.)
Occult stress incontinence
Stress incontinence on prolapse reduction (previously termed latent stress incontinence) is a term used to describe stress incontinence observed only after reduction of pelvic prolapse. Some believe that kinking of the urethra caused by the prolapse itself provides for at least part of the continence mechanism. These patients may have a history of stress incontinence that improved and finally resolved as their prolapse worsened.
In diagnosing occult incontinence, the goal is to avoid new-onset incontinence following surgical correction of prolapse. This may be accomplished through the use of an incontinence procedure, such as a colposuspension or sling. The diagnosis can be made by stress testing with the prolapse reduced or by pessary placement and pad testing. No particular method of prolapse reduction has been proved superior.
In a study of continent women with severe pelvic organ prolapse, reduction of the prolapse with a pessary revealed occult incontinence in 58% of cases. [17] These patients were treated with a pubovaginal sling, anterior colporrhaphy, and other appropriate reparative operations. Eighty-six percent of the patients with potential incontinence so treated had no postoperative stress-related urine loss.
The group of patients with no demonstrable occult incontinence underwent anterior colporrhaphy and additional individualized procedures. Incontinence procedures, per se, were not performed in this group. No patients had postoperative stress incontinence. Mean follow-up was 40-50 months.
This study points out that bladder neck procedures need not be performed if potential incontinence has been ruled out, even if bladder neck hypermobility is present. Indeed, incontinence procedures are not without their own morbidities and should not be performed unless necessary.
Urge incontinence pathophysiology
Urge incontinence is involuntary urine loss associated with a feeling of urgency. The corresponding urodynamic term is detrusor overactivity, which is the observation of involuntary detrusor contractions during filling cystometry. [18, 19] These contractions may be voluntary or spontaneous and may or may not cause symptoms of urgency and/or urgency incontinence.
However, a study using a quality of life assessment of women with incontinence showed that women with urge incontinence from detrusor overactivity consistently had a worse quality of life than did women with other urodynamic diagnoses.
Urge incontinence may be a result of detrusor myopathy, neuropathy, or a combination of both. When the identifiable cause is unknown, it is termed idiopathic urge incontinence. When a definable causative neuropathic disorder exists, the coexisting urinary incontinence disorder is termed neurogenic detrusor overactivity. Symptoms of overactive bladder or urge incontinence in the absence of neurologic causes are known simply as detrusor overactivity.
The term overactive bladder describes a syndrome of urinary urgency, usually accompanied by frequency and nocturia, with or without urgency urinary incontinence, in the absence of urinary tract infection or other obvious pathology. Overactive bladder in adults is a disorder of unclear etiology and incompletely understood pathophysiology. For discussion of this topic, see the article Overactive Bladder.
Some researchers believe that detrusor overactivity represents the premature initiation of a normal micturition reflex. In vitro studies of bladder muscle strips from patients with detrusor overactivity have demonstrated an increase in response to electrical stimulation and an increased sensitivity to stimulation with acetylcholine. [20] These findings may indicate a higher sensitivity to efferent neurologic activity or a lower threshold of acetylcholine release needed to initiate a detrusor contraction.
A relative cholinergic denervation may explain some of these findings. This proposed mechanism is most plausible in cases of de novo detrusor overactivity, which follow hysterectomy or other pelvic surgery. The mechanism of denervation in idiopathic detrusor overactivity is less certain. Subtle obstruction and the effects of aging on smooth muscle and the autonomic nervous system are 2 possible contributors.
Another finding described in bladder muscle specimens from patients with detrusor overactivity is local loss of inhibitory medullary neurologic activity. Vasoactive intestinal peptide, a smooth muscle relaxant, is decreased markedly in the bladders of patients with detrusor overactivity. In addition, bladders of individuals with detrusor overactivity have been found deficient in smooth muscle–relaxing prostaglandins.
Mills and colleagues conducted a comparison study of bladder muscle strips from patients with severe idiopathic detrusor overactivity and from organ donors with no known urologic problems. [18] The following are some of the findings:
-
Patchy partial denervation of the detrusor with areas of normal innervation and areas of reduced innervation by fibers staining for acetylcholinesterase
-
A reduced force of contraction in response to electrical field stimulation: This finding is in contrast to a previous study showing an increased sensitivity to electrical field stimulation, but the authors believe that the muscle strips may have had increased sensitivity to direct electrical stimulation (non–nerve mediated).
-
Supersensitivity to potassium
-
Increased electrical coupling of cells via cell-to-cell junctions
-
Variability in the activity of muscle strips from the same bladder
The authors believe that the primary abnormality in detrusor overactivity is at the detrusor muscle level with an increased capacity for spontaneous myogenic contractile activity and spread of electrical activity from cell to cell, resulting in tetanic contractions. Epidemiological studies have shown an association between detrusor overactivity and irritable bowel syndrome. [21] Some authorities have proposed that a syndrome of smooth muscle dysfunction may underlie this association.
Another study demonstrated the presence of an increased ratio of abnormal-to-normal cell junctions in patients with bladder dysfunction. The increased ratio was demonstrated most markedly in patients with detrusor overactivity. To a lesser degree, these changes also were observed in patients with outlet obstruction combined with detrusor overactivity and with idiopathic sensory urgency alone. [22]
These authors concluded that idiopathic sensory urgency might represent a milder or less overt variant of detrusor overactivity. They suggested that, in the future, bladder biopsy with structural evaluation of cell junctions might become a useful clinical tool in the diagnostic evaluation of bladder dysfunction. [22]
One study proposed that urge incontinence, regardless of the triggering mechanism, may share a final common pathway of myogenic dysfunction of the detrusor. [23] Spread of contractile signals via cell-to-cell coupling was proposed as the likely mechanism.
Another possible explanation for detrusor overactivity in a subgroup of patients involves the triggering of the micturition reflex by leakage of urine into a funneled and partially incompetent proximal urethra. This theory is consistent with the findings of detrusor overactivity caused by coughing or changing position.
In males, early obstruction due to benign prostatic hyperplasia (BPH) may result in urge incontinence. [24] The pathophysiology of BPH is poorly understood. Relative obstruction develops because of mechanical factors, dynamic factors, and detrusor alterations.
Androgen-induced enlargement of nodules of glandular tissue comprises the mechanical portion of the disorder. The dynamic component is related to increased alpha tone in prostatic and urethral smooth muscle. Detrusor dysfunction may consist of impaired contractility, detrusor overactivity, or both. In severe cases of obstruction, retention and overflow incontinence may develop, and the upper urinary tract can become damaged.
The presence of inflammation in the bladder is believed to result in bladder muscle irritability and urge incontinence in some instances, as depicted in the image below. One study showed that approximately 8% of patients with bacterial urinary tract infections had nonneuropathic bladder instability. If bacterial infection and detrusor overactivity coexist, successful treatment of the infection results in resolution of the detrusor overactivity in about one half of the patients.
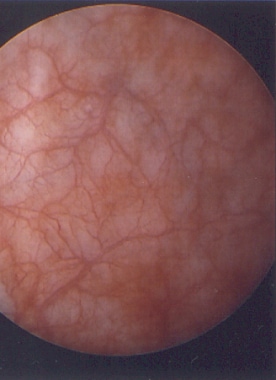 A cystoscopic view of the bladder mucosa reveals shallow ulcerations and petechial hemorrhages, which are findings consistent with interstitial cystitis.
A cystoscopic view of the bladder mucosa reveals shallow ulcerations and petechial hemorrhages, which are findings consistent with interstitial cystitis.
Nonbacterial inflammatory conditions of the bladder, including interstitial cystitis, have been associated with detrusor overactivity. Foreign bodies, including permanent sutures, bladder stones, and neoplasms, also have been linked to bladder irritability and instability.
Mixed incontinence pathophysiology
Mixed incontinence is urinary incontinence resulting from a combination of stress and urge incontinence. [10] Approximately 40-60% of females with incontinence have this combination. Although it is generally defined as detrusor overactivity and impaired urethral function, the actual pathophysiology of mixed urinary incontinence is still being investigated. While generally thought of as separate etiologies for incontinence, some indirect evidence may link these disorders in some instances. In order to effectively treat, it is important for clinicians to determine which subtype of incontinence is more dominant, if relevant.
In mixed incontinence, the bladder outlet is weak and the detrusor is overactive. A classic example of mixed incontinence is a patient with meningomyelocele and an incompetent bladder neck with a hyperreflexic detrusor; however, a combination of urethral hypermobility and detrusor instability is a more common scenario.
Mixed incontinence is a common finding in older patients with urinary incontinence disorders. Often, stress incontinence symptoms precede urge incontinence symptoms in these individuals. Urgency without actual urge-related urine loss also is a common complaint of patients with stress incontinence.
Some patients with stress incontinence have urine leakage into the proximal urethra that may, at first, trigger sensory urgency and/or bladder contractions, which initially are suppressible. Later, in a subgroup of these individuals, myopathic changes may occur in the bladder that make the spread of abnormally generated contractile signals more efficient and more difficult to suppress voluntarily.
Reflex incontinence pathophysiology
Reflex incontinence is due to neurologic impairment of the central nervous system. Common neurologic disorders associated with reflex incontinence include stroke, Parkinson disease, and brain tumors. Reflex incontinence also occurs in patients with spinal cord injuries and multiple sclerosis. Urge incontinence in patients with suprapontine or suprasacral spinal cord lesions, which was formerly known as detrusor hyperreflexia, is currently considered part of neurogenic detrusor overactivity.
Spinal cord injuries interrupt the sacral reflex arc from the suprasacral spinal cord, cerebral cortex, and higher centers. These pathways are crucial for voluntary and involuntary inhibition. In the initial phase of spinal cord injury, the bladder is areflexic and overflow incontinence results. Later, detrusor hyperreflexia usually is found upon urodynamic evaluation.
In multiple sclerosis (MS), demyelinating plaques in the frontal lobe or lateral columns can produce lower urinary tract disorders. Incontinence may be the presenting symptom of MS in about 5% of cases. Approximately 90% of individuals with MS experience urinary tract dysfunction during the course of the disease.
A summary of the published series of urodynamic findings in MS demonstrated that in patients with lower urinary tract dysfunction, the most common urodynamic diagnosis is detrusor hyperreflexia (62%). Detrusor-sphincter dyssynergia (25%) and detrusor hyporeflexia (20%) also are common. Obstructive findings are much more common in males. Of note, the urodynamic diagnosis may change over time as the disease progresses. [25]
Hemorrhage, infarction, or vascular compromise to certain areas of the brain can result in lower urinary tract dysfunction. The frontal lobe, internal capsule, brainstem, and cerebellum commonly are involved sites. Initially, urinary retention due to detrusor areflexia is observed. This may be followed by detrusor hyperreflexia.
Approximately 40-70% of patients with Parkinson disease have lower urinary tract dysfunction. Controversy exists as to whether specific neurologic problems in patients with Parkinson disease lead to bladder dysfunction or if bladder symptoms simply are related to aging. The extrapyramidal system is believed to have an inhibitory effect on the micturition center; theoretically, loss of dopaminergic activity in this area could result in loss of detrusor inhibition.
In patients with dementia, incontinence and urinary tract dysfunction may be due to specific involvement of the areas of the cerebral cortex involved in bladder control. Alternatively, incontinence may be related to global deterioration of memory, intellectual capacity, and behavior. Urodynamically, both detrusor hyperreflexia and areflexia have been found.
CNS neoplasms may result in incontinence. Tumors of the superior medial frontal lobe, spinal cord tumors above the conus medullaris, and cervical spondylosis can cause detrusor hyperreflexia.
Overflow incontinence pathophysiology
The major contributing factor to overflow incontinence is incomplete bladder emptying secondary to impaired detrusor contractility or bladder outlet obstruction. [10] Impaired detrusor contractility is typically neurogenic in nature; causes include diabetes mellitus, lumbosacral nerve disease from tumors, meningomyelocele, MS, prolapsed intravertebral disks, and high spinal cord injuries. Less common causes of overflow incontinence include AIDS, genital herpes affecting the perineal area, and neurosyphilis.
In most cases, both sensory and motor neuropathies are present. The maximal storage capacity of the bladder is reached, oftentimes without the individual realizing that this has occurred. Incontinence occurs off the top of a chronically over-filled bladder. Effective emptying is not possible because of an acontractile detrusor muscle.
Common causes of bladder outlet obstruction in men include benign prostatic hyperplasia (BPH), vesical neck contracture, and urethral strictures. In women, urethral obstruction after anti-incontinence surgery such as a sling or bladder neck suspension can result in iatrogenically induced overflow incontinence. Additionally, prolapse of the anterior vaginal wall can affect bladder emptying.
Functional incontinence
Functional incontinence is seen in patients with normal voiding systems but who have difficulty reaching the toilet because of physical or psychological impediments. In some cases, the cause is transient or reversible. In others, a permanent problem can be identified. The etiology of the incontinence may be iatrogenic, environmental, situational, or disease related. The following common mnemonic, DIAPPERS, is helpful in remembering the functional contributors to incontinence [26] :
-
D - Delirium
-
I - Infection, urinary
-
A - Atrophic urethritis or vaginitis
-
P - Pharmacologic agents
-
P - Psychiatric illness
-
E - Endocrine disorders
-
R - Reduced mobility or dexterity
-
S - Stool impaction
Integral theory
A unifying theory of the etiology of stress incontinence, urge incontinence, voiding dysfunction, and fecal incontinence in women has been proposed. [27] The basis of the theory is that these disorders are the result of overstretching of the vaginal connective tissue and supporting ligaments, which usually occurs during childbirth.
Laxity of the pubourethral ligaments (ie, anterior zone of damage), mid vagina (ie, middle zone), and uterosacral ligaments (ie, posterior zone) make the usual tridirectional support of the vagina ineffective. With the vagina no longer properly tethered to the pelvic girdle, the usual neuromuscular actions that occur during increases in intra-abdominal pressure or pelvic floor relaxation during voiding are not translated as effectively into urethral closure and opening, respectively.
Detrusor overactivity, according to this theory, occurs because of the premature firing of stretch receptors in the bladder base secondary to poor endopelvic connective tissue support to the filling bladder.
The integral theory is attractive from the standpoint of parsimony but is complex. The theory is best appreciated and understood with the help of illustrations and diagrams showing directional force vectors.
Continuous incontinence
This severe type of incontinence is characterized by constant or near constant leakage with no symptoms other than wetness. Generally, this represents a significant breech in the storage capabilities of the bladder or urethra. Urogenital fistulas are a classic example.
A nonfunctioning urethra can result in continuous leakage. Scarring and fibrosis from previous surgery, partial urethral resection for vulvar cancer, and urethral sphincter paralysis due to lower motor neuron disease can cause the urethra to fail.
Pelvic irradiation may not only cause urogenital fistula but in rare cases causes bladder noncompliance that results in continuous incontinence. Congenital malformations of the genitourinary tract, such as bladder exstrophy, [28] epispadias, and ectopic ureters, can result in total incontinence.
Pediatric urinary incontinence
Pediatric incontinence disorders are classified according to cause. Primary incontinence disorders generally are due to congenital structural disorders, including ectopic ureter, exstrophy, epispadias, and patent urachus. Secondary structural causes can result from obstruction from urethral valves, congenital urethral strictures, and large ectopic ureteroceles. In addition, trauma can result in secondary structural incontinence.
Neurogenic lesions make up the next category of pediatric incontinence disorders. These include spinal dysraphism, tethered spinal cord, and spinal cord tumors.
Nonstructural causes account for most cases of pediatric incontinence. [29] Infection and inflammation may be the source. Dysfunctional voiding habits can develop even at a young age. Some children may become so preoccupied with activities that voiding is delayed until capacity is reached and accidents result.
Some believe that certain children develop a pattern of not relaxing the pelvic floor while voiding. In some cases, this can be traced back to an infection or some other noxious stimuli. A vicious cycle of pelvic floor spasm, constipation, and urinary retention can develop.
So-called giggle incontinence has been thought to represent an underlying temporal lobe seizure. Other studies do not support this theory, however.
Vaginal voiding is a pseudoincontinence disorder, which may result from voiding with the legs held too tightly together. The impeded flow of urine may fill the vagina. The vagina empties when the child stands.
Nocturnal enuresis is the most common pediatric incontinence disorder. For discussion of this topic, see Enuresis.
Etiology
Even in an individual patient, urinary incontinence may have multiple etiologies, with varying degrees of contribution to the overall disorder. Structural and functional disorders involving the bladder, urethra, ureters, and surrounding connective tissue can contribute. In addition, a disorder of the spinal cord or central nervous system (CNS) may be the major etiologic factor in some cases. Medical comorbidities also can be important. Finally, some cases of urinary incontinence may be pharmacologically induced. [30]
The most common cause of stress incontinence in women is urethral hypermobility secondary to poor anatomic pelvic support. Women may lose this pelvic support with postmenopausal estrogen loss, childbirth, surgery, or certain disease states that affect tissue strength. A less common cause of stress incontinence is intrinsic sphincter deficiency, which can result from the aging process, pelvic trauma, surgery (eg, hysterectomy, [31] urethropexy, pubovaginal sling), or neurologic dysfunction.
The most common cause of intrinsic sphincter deficiency in men is radical prostatectomy for prostate cancer or transurethral resection of the prostate for benign prostatic hyperplasia. [32] A less common cause of intrinsic sphincter deficiency is trauma to the bladder neck or prostate, resulting from pelvic fracture due to high-impact deceleration injuries.
Contributing factors with aging-related urinary incontinence include a weakening of connective tissue, genitourinary atrophy due to hypoestrogenism, increased incidence of contributing medical disorders, increased nocturnal diuresis, and impairments in mobility and cognitive functioning. [10, 33] Vitamin D deficiency has been identified as a risk factor for urinary incontinence in older adults. [34]
Other factors that may increase the risk of developing incontinence include obesity, straining at stool as a child or young adult, heavy manual labor, chronic obstructive pulmonary disease, and smoking. [35, 36, 37] In many cases of incontinence that are due to detrusor overactivity, the problem is idiopathic in nature.
In a prospective cohort study of 5,391 young women from the Australian Longitudinal Study on Women's Health, depressive symptoms were associated with 37% higher odds of having urinary incontinence after adjustment for sociodemographic factors, body mass index, health behaviors, and reproductive factors. Having physician-diagnosed depression was associated with 42% higher odds. [38]
A review of women with type 1 diabetes mellitus who participated in the Diabetes Control and Complications Trial (DCCT) and its observational follow-up study, the Epidemiology of Diabetes Interventions and Complications (EDIC), found that incident urinary incontinence was associated with higher hemoglobin A1c levels, independent of other recognized risk factors. Thus, improved glycemic control might reduce the risk of urinary incontinence in such patients. [39]
Less frequent causes of urinary incontinence include complications of urologic procedures or pelvic radiation therapy. In the pediatric population, causes include enuresis and congenital abnormalities of the genitourinary system.
Transient causes
Transient urinary incontinence is often seen in both elderly and hospitalized patients. The mnemonic DIAPPERS is a good way to remember most of the reversible causes of incontinence, as follows [26] :
-
D - Delirium or acute confusion
-
I - Infection (symptomatic UTI)
-
A - Atrophic vaginitis or urethritis
-
P - Pharmaceutical agents
-
P - Psychological disorders (depression, behavioral disturbances)
-
E - Excess urine output (due to excess fluid intake, alcoholic or caffeinated beverages, diuretics, peripheral edema, congestive heart failure, or metabolic disorders such as hyperglycemia or hypercalcemia)
-
R - Restricted mobility (limits ability to reach a bathroom in time)
-
S - Stool impaction
In addition to urinary tract infection, conditions such as bladder cancer, bladder stones, and foreign bodies can irritate the bladder, resulting in involuntary bladder contractions and incontinence. Less common infectious causes of overflow incontinence include AIDS, genital herpes affecting the perineal area, and neurosyphilis. Stones or neoplasms may also result in incontinence due to obstruction.
Neurologic causes
Cortical lesions (eg, from strokes, tumors, aneurysms, or hemorrhages) can lead to inappropriate voiding secondary to depressed social awareness, decreased sensation, and/or inappropriate urethral sphincter relaxation. [26] Cerebrovascular disease doubles the risk for urinary incontinence in older women.
Spinal cord lesions can alter sympathetic and parasympathetic tone, resulting in urinary incontinence. Peripheral nerve disease such as diabetic peripheral neuropathy can cause urinary incontinence through a contractile dysfunction of the bladder.
Metastatic carcinoma can cause epidural spinal cord compression. Back pain is the initial symptom in most cases. Almost 20% of cases involve the lumbosacral spine. If the sacral cord is involved, urinary incontinence or retention can be expected. Urinary incontinence symptoms represent an unfavorable prognostic indicator in this patient population. Early diagnosis and treatment of spinal cord compression is extremely important. Paraplegia or quadriplegia can develop within hours or days after the first neurologic deficit appears.
S2-S5 nerve root injury (herniation) can cause bladder dysfunction. Cauda equina syndrome can develop in patients with a large centrally protruding disk. Symptoms include bilateral leg pain and weakness, saddle anesthesia, urinary retention or incontinence, and fecal retention or incontinence. It is important to recognize this syndrome early because there is a high risk for chronic neurologic deficits if treatment is delayed.
Hemi–cauda equina syndrome (from a herniated lumbar disk) can also manifest as urinary incontinence. It presents as unilateral leg pain, unilateral sensory deficit in the S1-S5 dermatomes, and urinary incontinence or urinary retention. These patients require urgent neurosurgical consultation for emergency surgery.
Multiple sclerosis should be considered in any patient without evidence of urinary tract infection who has episodic or rapid onset of urinary symptoms. Urinary incontinence may occur by itself or may be accompanied by other vague neurological symptoms.
Patients with a neurogenic disorder such as myelomeningocele may have an open bladder neck that results in severe intrinsic sphincter deficiency and urinary loss.
Pharmacologic causes
Many medications contribute to urinary incontinence, directly or indirectly. Medications must always be considered as the cause of new-onset urinary incontinence—especially in elderly persons, in whom polypharmacy is often encountered. [40, 26]
Medication may result in incontinence through the following mechanisms:
-
Drugs with anticholinergic properties or side effects (eg, antipsychotics, antidepressants) - Urinary retention and thus overflow incontinence
-
Alpha-adrenergic agonists - Urinary retention and thus overflow urinary incontinence
-
Alpha-antagonist - Urethral relaxation
-
Diuretics – Overwhelming of bladder capacity in elderly persons
-
Calcium channel blockers - Decreased smooth muscle contractility in the bladder, causing urinary retention with overflow incontinence
-
Sedative-hypnotics - Immobility secondary to sedation, leading to functional incontinence
-
Angiotensin-converting enzyme (ACE) inhibitors – Diuretic effect, as well as side effect of cough with relaxation of pelvic floor musculature, can exacerbate incontinence
-
Antiparkinson medications - Urinary urgency and constipation
Epidemiology
The precise prevalence of urinary incontinence is difficult to estimate. Part of the difficulty has been in defining the degree, quantity, and frequency of urine loss necessary to qualify as pathologic, with varying definitions among studies. Consequently, the prevalence of urinary incontinence reported in the literature is varied.
In addition, urinary incontinence is underdiagnosed and underreported. An estimated 50-70% of women with urinary incontinence fail to seek medical evaluation and treatment because of social stigma. Only 5% of incontinent individuals in the community and 2% in nursing homes receive appropriate medical evaluation and treatment. People with incontinence often live with this condition for 6-9 years before seeking medical therapy.
In a Swedish study of 9197 nulliparous women aged 25-64 years, the rate of urinary incontinence increased from 9.7% in the youngest women with a body mass index < 25 kg/m2 to 48.4% among the oldest women with a body mass index ≥35 kg/m2. [41] In a Dutch study of 1257 adults, the prevalence of urinary incontinence was 49.0% in women versus 22.6% in men. In both men and women, the prevalence of urinary incontinence increased with aging. [42, 43]
Urinary incontinence has been estimated to affect 10-13 million people in the United States and 200 million people worldwide. The cost of treating urinary incontinence in United States alone is $16.3 billion, 75% of which is spent on treatment of women. Urinary incontinence can result in prolonged hospital admission, urinary tract infections, contact dermatitis, and falls. Urinary incontinence is a leading cause of admission to a nursing home when families find it too difficult to care for a relative with incontinence.
Sex- and age-related patterns
Age is the single largest risk factor for urinary incontinence, although at any age, urinary incontinence is more than 2 times more common in females than in males. Urinary incontinence affects up to 7% of children older than 5 years, 10-35% of adults, and 50-84% of the elderly persons in long-term care facilities. [2]
In a cross-sectional analysis of women who participated in the 2005-2006 National Health and Nutrition Examination Survey (NHANES), Nygaard et al demonstrated that the prevalence of urinary incontinence increased with age, but reported a lower overall prevalence than other researchers. The prevalence was 6.9% in women aged 20-39 years, 17.2% in those aged 40-59 years, 23.3% in those aged 60-79 years, and 31.7% in women older than 80 years. [44]
An age-related pattern also appears in the predominant type of urinary incontinence experienced. In general, studies have shown that stress urinary incontinence tends to be more common in women younger than 65 years, while urge urinary incontinence and mixed urinary incontinence is more common in women older than 65 years.
Stress incontinence affects 15-60% of women—both young and old individuals. More than 25% of nulliparous young college athletes experience stress incontinence when participating in sports.
Race-related factors
Although data concerning urinary incontinence in people of different races are sparse, reports are emerging that race may play an important role in the prevalence and likelihood of reporting of incontinence. In addition, differences in anatomic morphology of the urinary sphincter mechanism in people of different races may affect the likelihood of developing incontinence.
Fultz et al found that 23.02% of white women reported incontinence, compared with 16.17% of black women. [45] In a study by Anger et al, based on the 1999-2000 NHANES data, the prevalence of urinary incontinence was higher in non-Hispanic white women (41%) than in non-Hispanic black (20%) or Mexican American women (36%). [46] In contrast, Freeman et al found that black women were significantly more likely than white women to report menopausal symptoms (46% vs 30%), urinary incontinence, and vaginal dryness. [47]
Howard et al described functional and morphologic differences in the urethral sphincteric and support system of nulliparous black and white women. Black women demonstrated a 29% higher average urethral closure pressure during a maximum pelvic muscle contraction. Paradoxically, a 36% greater bladder neck hypermobility was present as measured with the cotton-swab test (black women at 49° vs white women at 36°). [42]
Sears et al reported that, among patients with incontinence, urge incontinence was more common in black women (51.5%), whereas stress incontinence was statistically significantly more common in white women (66.2%). [48] Daneshgari et al found that Hispanic women reported stress incontinence and mixed incontinence more often than did non-Hispanic white women. However, the increased prevalence of incontinence in Hispanic women is likely due to higher prevalences of obesity, hysterectomy, and parity than in white women. [49]
Nygaard et al examined the prevalence of symptomatic pelvic floor disorders in women in the United States and found no difference among non-Hispanic whites (16%), Hispanics (15.9%), non-Hispanic blacks (13.8%), and other races (15%). [44] These authors did not differentiate urge from stress incontinence.
Prognosis
The prognosis of a patient with incontinence is excellent with current health care. With improvement in information technology, well-trained medical staff, and advances in modern medical knowledge, patients with incontinence should not experience the morbidity and mortality of the past. Although the ultimate well-being of a patient with urinary incontinence depends on the precipitating condition, urinary incontinence itself is easily treated and prevented by properly trained health care personnel.
In stress incontinence, the improvement rate with alpha-agonists is 19-74%; improvement rates with muscle exercise and surgery, improvement rates are 87% and 88%, respectively. [50] In urge incontinence, the improvement rate is higher with bladder training (75%) than with the use of anticholinergics (44%). Surgical options for urge incontinence are limited and have a high morbidity.
In mixed incontinence, bladder training and pelvic exercises result in higher improvement rate than the use of anticholinergic medications. In overflow incontinence, medications and surgery are very effective in improving symptoms.
Without effective treatment, urinary incontinence can have an unfavorable outcome. Prolonged contact of urine with the unprotected skin causes contact dermatitis and skin breakdown. If left untreated, these skin disorders may lead to pressure sores and ulcers, possibly resulting in secondary infections.
The medical morbidity includes includes the following:
-
Perineal candidal infections
-
Cellulitis
-
Pressure sores
-
Constant skin irritation and moisture
-
Falls and subsequent fractures from slipping on urine
-
Sleep deprivation from nocturia
Psychological morbidity includes the following:
-
Poor self-esteem
-
Social withdrawal
-
Depression
-
Sexual dysfunction from embarrassment
-
Curtailed social and recreational activities
For individuals with a decompensated bladder that does not empty well, the postvoid residual urine can lead to overgrowth of bacteria and subsequent urinary tract infection (UTI). Untreated UTIs may lead to urosepsis and death.
Patients whose urinary incontinence is treated with catheterization also face risks. Both indwelling catheters and intermittent catheterization have a range of potential complications (see Treatment).
Urinary incontinence is a leading cause of admission to a nursing home when families find it too difficult to care for a relative with incontinence.
A study by Foley et al looked at the connection between urinary symptoms, poor quality of life, and physical limitations and falls among elderly individuals. These authors found that urinary incontinence and falling had an impact on quality of life and were, in fact, associated with physical limitations. [51]
Patient Education
For patient education information, see the following:
-
Urinary incontinence. Normal findings on urodynamic study of a 35-year-old white man. During the filling cystometrogram (CMG), there is absence of uninhibited detrusor contractions. Bladder compliance is normal. His maximum bladder capacity is 435 mL. During the pressure-flow study, his maximum flow rate (Qmax) is 25 mL/s and detrusor pressure at maximum flow rate (Pdet Qmax) is 50 cm H2O. The uroflow pattern is without abnormality, producing a bell-shaped curve without any abdominal straining. He voids to completion, and the postvoid residual urine is negligible.
-
Urinary incontinence. Urodynamic study revealing detrusor instability in a 75-year-old man with urge incontinence. Note the presence of multiple uninhibited detrusor contractions (phasic contractions) that is generating 40- to 75-cm H2O pressure during the filling cystometrogram (CMG). He also has small bladder capacity (81 mL), which is indicative of poorly compliant bladder.
-
Urinary incontinence. Urodynamic study revealing detrusor hyperreflexia in a 22-year-old woman with multiple sclerosis. Note the presence of multiple phasic contractions (uninhibited detrusor contractions) generating as much as 100 cm H2O pressure.
-
Urinary incontinence. Urodynamic recording of bladder outlet obstruction due to benign prostatic hyperplasia (BPH) in a 55-year-old man. Note that during a pressure-flow study, his maximum flow rate (Qmax) is only 6 mL/s and detrusor pressure at maximum flow rate (Pdet Qmax) is very high at 101 cm H2O. He also has a small bladder capacity (50 mL) due to chronic bladder outlet obstruction. His flow curve is flat and "bread-loaf" in pattern, which is consistent with infravesical obstruction.
-
Urinary incontinence. Urodynamic study revealing detrusor sphincter dyssynergia in a 35-year-old woman with C5 spinal cord injury. Note the absence of uninhibited detrusor contractions during the filling cystometrogram (CMG). Typically, patients with cervical cord lesions manifest detrusor hyperreflexia. However, this patient is taking Ditropan XL. Thus, phasic contractions are suppressed. During the pressure-flow study, note the increase in amplitude of the electromyogram (EMG) coincident with detrusor contraction and voiding. Her uroflow rate is low (1 mL/s), detrusor pressure is high (42 cm H2O), and the EMG recording is elevated.
-
Urinary incontinence. Video-urodynamic study illustrating type III stress urinary incontinence (intrinsic sphincter deficiency [ISD]) in a 65-year-old woman. Static cystogram reveals obvious contrast leakage via the urethra during Valsalva maneuver. Urodynamic study records abdominal leak point pressure (ALPP) of 55 cm H2O, consistent with ISD.
-
A cystoscopic view of the bladder mucosa reveals shallow ulcerations and petechial hemorrhages, which are findings consistent with interstitial cystitis.
-
A cotton swab angle greater than 30° denotes urethral hypermobility. Figure 1 shows that the cotton swab at rest is zero with respect to the floor. Figure 2 shows that the cotton swab at stress is 45° with respect to the floor.
-
A squirt of urine is observed at the peak of an increase in intra-abdominal pressure in a supine patient
-
This photo illustrates a variety of pelvic organ prolapses, including grade-IV cystocele, uterine descensus, enterocele, and rectocele alone or in combination. In situations where a significant prolapse (eg, uterus, bladder) has occurred, evaluate for possible ureteral obstruction at the level of the pelvic inlet.
