Practice Essentials
More than 600 drugs are known to cause pulmonary toxicity, and illicit drugs are well-known to result in pulmonary toxicities. To minimize the potential morbidity and mortality from drug-induced respiratory diseases, healthcare providers should be familiar with the possible adverse effects of the medications they prescribe. A list of drugs that are reported to cause pulmonary toxicity is available on the continually updated Website PNEUMOTOX online.
Drug-induced pulmonary toxicity is a diagnosis of exclusion. This condition can be suspected if the patient has been exposed to a likely causative drug, develops new signs and symptoms, and has a remittence of these symptoms once the drug is withheld.
Adverse drug reactions can involve the pulmonary parenchyma, pleura, airways, pulmonary vascular system, mediastinum, and neuromuscular system that contribute to respiration. These reactions can manifest acutely, subacutely, or chronically. See the image below.
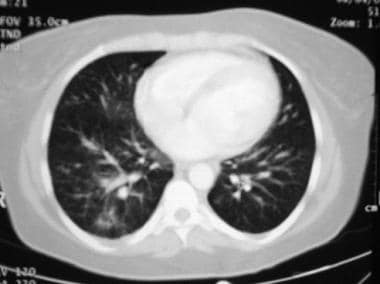 This image is a computed tomography scan of a patient with sarcoidosis. The pattern of multiple nodules seen here can manifest in patients taking medications that can cause granulomatous reactions.
This image is a computed tomography scan of a patient with sarcoidosis. The pattern of multiple nodules seen here can manifest in patients taking medications that can cause granulomatous reactions.
Before starting patients on any medication, educate them about the potential adverse effects of the drug. Patients who develop drug toxicity should be advised to avoid the drug in the future.
Signs and symptoms
Drug-induced lung diseases have no pathognomonic clinical, laboratory, physical, radiographic, or histologic findings. However, Irey defined the following set of criteria for the diagnosis of drug reactions [1] :
-
Correct identification of the drug, its dose, and its duration of administration
-
Exclusion of other primary or secondary lung diseases
-
Temporal eligibility: Appropriate latent period (exposure to toxicity)
-
Recurrence with rechallenge (not commonly performed)
-
Singularity of drug (ie, other drugs the patient is taking)
-
Remission of symptoms with removal of the drug
-
Characteristic pattern of reaction to a specific drug (perhaps previously documented)
-
Quantification of drug levels that confirm abnormal levels (especially for overdoses)
-
Degree of certainty of drug reaction (ie, causative, probable, or possible)
Nonspecific physical examination findings may include crackles in the case of noncardiac pulmonary edema (NCPE), wheezes in the case of bronchospasm, and decreased breath sounds in pleural effusion.
See Presentation for more detail.
Diagnosis
The diagnosis of drug-mediated pulmonary toxicity is usually established based on clinical findings. In general, laboratory analyses are not helpful.
Radiologic patterns observed in drug-induced pulmonary toxicity are highly variable and depend on the type of adverse reaction the patient is experiencing. Most drug-induced pulmonary toxicities involve the parenchyma, thus, interstitial infiltrates may be demonstrated on radiographs. Pleural fluid may be the only finding. However, the radiographs may be normal or minimally abnormal if the airways or pulmonary vasculature are/is affected. High-resolution computed tomography (CT) scanning is more sensitive than chest radiography for defining the radiographic abnormalities. [2]
Pulmonary function testing (PFTs) primarily results in a restrictive lung disease pattern, with decreases in the total lung capacity (TLC). The ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) may be normal or increased, whereas the diffusion capacity of the lung (DLCO) is typically decreased (this measure of lung function is often the first to be diminished).
If the drug-induced pulmonary toxicity causes airway obstruction, then the FEV1/FVC ratio and FEV1 will be reduced. The residual volume to total lung capacity (RV/TLC) ratio may be increased.
In general, bronchoscopy with transbronchial biopsy is not helpful in establishing the diagnosis of drug-induced pulmonary toxicity. Transbronchial biopsy, however, may aid in the diagnosis of pulmonary involvement by other diseases such as sarcoidosis, metastatic cancer, or lymphoma. Bronchoalveolar lavage (BAL) can contribute to the expected clinicopathologic pattern of a given drug-induced lung disease such as identifying eosinophils in a drug-induced eosinophilic pneumonia. BAL also is helpful in the differential diagnosis, primarily by excluding an infective etiology to the pulmonary infiltrates.
Similarly, video-assisted thoracoscopic and open lung biopsies are not typically useful in establishing the diagnosis of drug-induced pulmonary toxicities. These invasive procedures, however, may lead to the diagnosis of other diseases.
See Workup for more detail.
Management
The treatment of drug-induced lung disease consists of immediately discontinuing the offending drug and appropriately managing the pulmonary symptoms. Acute episodes of drug-induced pulmonary disease often remit 24-48 hours after the drug has been discontinued. Chronic syndromes may take a month or longer to resolve.
General supportive measures include the following:
-
Smoking cessation
-
Control of other chronic underlying lung disease
-
Prompt treatment of concomitant respiratory infections
Anecdotal reports indicate that glucocorticoid therapy has been associated with rapid improvement in gas exchange and reversal of radiographic abnormalities in some drug-induced pulmonary toxicities.
See Treatment and Medication for more detail.
Background
More than 600 drugs, as well as illicit drugs, are known to cause pulmonary toxicity. This number is expected continue to increase as new therapeutic agents and illicit drugs are developed and used. Because the medications that cause respiratory diseases are used by a variety of healthcare providers, including generalists, specialists, and subspecialists, virtually no area of medicine is free from encounters of patients experiencing adverse drug reactions.
Recognition of drug-induced lung disease is difficult, because the clinical, radiologic, and histologic findings are nonspecific. Therefore, to minimize the potential morbidity and mortality from drug-induced respiratory diseases, healthcare providers should be familiar with the possible adverse effects of the medications they prescribe. Clinicians can make a correct diagnosis only if they are aware of the drugs that have been identified to cause pulmonary reactions and their specific manifestations. The continually updated Website PNEUMOTOX online provides a list of drugs that are reported to cause pulmonary toxicity. (Also see Medscape's Pill Identifier tool.)
Drug-induced pulmonary toxicity is a diagnosis of exclusion. Other disease processes must be ruled out before establishing this diagnosis. Such diseases processes include respiratory infections; occupational, recreational, and environmental exposures; specific respiratory disorders; and systemic diseases. Drug-induced pulmonary toxicity can be suspected if the patient has been exposed to a likely causative drug, develops new signs and symptoms, and has a remittence of these symptoms once the drug is withheld. Although the best evidence for drug-induced pulmonary toxicity is to rechallenge the patient, this procedure is potentially hazardous and rarely done in human subjects.
Adverse drug reactions can involve the pulmonary parenchyma, pleura, airways, pulmonary vascular system, mediastinum, and neuromuscular system that contribute to respiration. These reactions can manifest acutely, subacutely, or chronically. See the image below.
This image is a computed tomography scan of a patient with sarcoidosis. The pattern of multiple nodules seen here can manifest in patients taking medications that can cause granulomatous reactions.
Pathophysiology
Medications can elicit a wide variety of thoracic tissue effects and responses. The adverse reactions can involve the the pulmonary parenchyma, pleura, airways, pulmonary vascular system, mediastinum, and neuromuscular system. The clinical and histopathologic entities reported as drug-induced pulmonary toxicities are outlined below. These reactions can manifest acutely, subacutely, or chronically. Moreover, in some drug-induced pulmonary toxicities, there is involvement of the parenchyma and the airways or the parenchyma and the pulmonary vasculature.
Adverse reactions involving the pulmonary parenchyma
-
Interstitial pneumonitides: Usual interstitial pneumonitis, nonspecific interstitial pneumonitis, desquamative interstitial pneumonitis, giant cell interstitial pneumonitis, lymphocytic interstitial pneumonitis, respiratory bronchiolitis with interstitial pneumonitis
-
Noncardiac pulmonary edema (NCPE)
-
Cardiac pulmonary edema (from myocardial toxicities)
-
Pulmonary infiltrates and eosinophilia (PIE)
-
Eosinophilic pneumonia
-
Hypersensitivity pneumonitis
-
Cryptogenic organizing pneumonia (COP) (also known as bronchiolitis obliterans-organizing pneumonia [BOOP])
-
Diffuse alveolar damage (DAD)
-
Pulmonary hemorrhage
-
Granulomatous pneumonitis
-
Lipoid pneumonia
-
Pulmonary alveolar proteinosis
-
Eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome)
-
Pulmonary fibrosis
-
Pulmonary nodule(s)
Adverse reactions involving the pleura
-
Pleural effusion
-
Drug-induced lupus with pleural effusion
-
Eosinophilic pleural effusion
-
Pleural thickening or fibrosis
-
Ovarian hyperstimulation syndrome
-
Pneumothorax
Adverse reactions involving the airways
-
Bronchospasm, bronchoconstriction, asthma
-
Bronchiolitis obliterans
-
Cough
-
Dysphonia or hoarseness
-
Calcification of the cartilaginous rings
-
Churg-Strauss syndrome
-
COP (or BOOP)
Adverse reactions involving the pulmonary vasculature
-
Pulmonary hypertension
-
Pulmonary thromboembolic disease
-
Pulmonary veno-occlusive disease
-
Pulmonary hemorrhage
-
Pulmonary vasculitis
-
Churg-Strauss syndrome
-
Diffuse alveolar hemorrhage
-
Hemoptysis
-
Pulmonary hematoma
Adverse reactions involving the mediastinum
-
Pseudosarcoidosis
-
Mediastinal lymphadenopathy
-
Lymphoproliferative disease
-
Mediastinal lipomatosis
Adverse reactions involving neuromuscular dysfunction
-
Respiratory muscle weakness or paralysis
-
Respiratory muscle rigidity
-
Central respiratory depression, apnea
-
NCPE
Mechanisms of pulmonary injury
Pulmonary toxicity secondary to drugs may be due to a variety of mechanisms, such as the following:
-
Oxidant injury
-
Pulmonary vascular damage
-
Deposition of phospholipids within cells
-
Immune system–mediated injury
-
Central nervous system (CNS) depression
-
Direct toxic effect
Oxidant injury
Oxidant-mediated injury plays a significant role in several drug-induced pulmonary diseases. Oxidant molecules (eg, oxygen, hydrogen peroxide, hypochlorous acid) that are formed within phagocytic cells such as monocytes, macrophages, and neutrophils may participate in redox reactions resulting in fatty-acid oxidation that lead to membrane instability and perhaps autologous cytotoxicity.
Normally, antioxidant defense mechanisms (ie, superoxide dismutase, glutathione peroxidase, alpha tocopherol) provide the necessary balance to offset the oxidant effects. The classic examples of drug-mediated oxidant injury are chronic reactions to nitrofurantoin and, possibly, many of the chemotherapeutic drug-induced pulmonary injuries.
Nitrofurantoin may produce pulmonary fibrosis by accelerating the generation of oxygen radicals within lung cells, overwhelming the normal antioxidant protective mechanisms; this, in turn, incites an inflammatory and fibrotic reaction. Similarly, antineoplastic drugs may disturb oxidant/antioxidant system homeostasis, resulting in pulmonary injury.
Pulmonary vascular damage
Drug-induced pulmonary vascular disease manifests clinically as acute pulmonary edema, diffuse interstitial lung disease, pulmonary vascular occlusion, and pulmonary hypertension or hemorrhage. The proposed mechanisms of lung vascular damage include the following:
-
Increased microvascular hydrostatic pressure
-
Increased permeability of the vascular endothelium
-
Vascular occlusion by direct activation of inflammatory and immune mechanisms, or indirectly by stimulating intravascular coagulation (pulmonary thromboembolism)
-
Impaired homeostasis
Deposition of phospholipids within cells
Similar to other amphiphilic compounds, amiodarone can cause an accumulation of phospholipids within lysosomes in the lung cells and other tissues, owing to the inhibition of phospholipase A. Amiodarone has been demonstrated to produce phospholipidosis in alveolar macrophages and in alveolar type 2 cells. Ultrastructural studies show myelinoid inclusion bodies in the affected tissue. The process is reversible with discontinuation of the causative drug.
Immune system–mediated injury
Drugs can act as potential antigens, or haptens, inducing an immune cascade that can lead to the development of immune-mediated lung toxicity. Deposition of antigen-antibody complexes may trigger an inflammatory response, leading to pulmonary edema and interstitial lung disease. Drug-induced systemic lupus erythematosus is an example of immune-mediated lung damage.
CNS depression
The medulla is believed to activate sympathetic components of the autonomic nervous system. An acute neurologic crisis, accompanied by a marked increase in intracranial pressure, may stimulate the hypothalamus and the vasomotor centers of the medulla. This, in turn, initiates a massive autonomic discharge, leading to neurogenic pulmonary edema.
Acute NCPE can occur after administration of a number of drugs. Some examples are as follows:
-
Naloxone
-
Heroin
-
Interleukin 2
-
All-trans -retinoic acid
-
Contrast media
-
Intrathecal methotrexate (MTX)
-
Cytarabine
Direct toxic effect
Chemotherapeutic drugs can cause a direct toxic reaction. The acute pulmonary toxicity of bleomycin has been attributed to DNA strand scission, with resulting chromosomal injury. Animal studies confirm that more chronic bleomycin injury occurs predominantly in the lungs, which have very low levels of bleomycin hydrolase activity.
Type 1 epithelial cells are more vulnerable to bleomycin toxicity. This direct cellular damage can lead to bleomycin-induced pulmonary fibrosis (also called fibrosing alveolitis), which usually develops subacutely, from 1 to 6 months after bleomycin treatment, but it may occur acutely or more than 6 months following the administration of bleomycin.
Risk factors
The likelihood of developing adverse pulmonary effects from drugs remains largely unpredictable and idiosyncratic. A limiting dose has only been identified for a few drugs. Thus, monitoring of patients who receive such drugs is advisable for a small number of these agents (ie, amiodarone, bleomycin), but even this step remains in debate. Some of the known risk factors for these selected drugs include the following:
-
Advanced age
-
Cumulative dose
-
Simultaneous oxygen therapy
-
Combination therapy
-
Radiation therapy
-
Occupational factors
-
Underlying lung disease
-
Genetic factors
Advanced age has been shown to be a risk factor for the development of drug-induced pulmonary disease. Bleomycin can cause significant lung toxicity in patients older than 70 years.
Cytotoxic agents generally exhibit increasing toxicity with increasing dose. This is believed to be a result of drug accumulation in the lungs themselves. The rate of pulmonary toxicity with high-dose (>1500 mg/m2) bis -chloroethylnitrosourea (BCNU) therapy varies from 20% to 50%.
Exposure to high concentrations of oxygen may contribute to or aggravate adult respiratory distress syndrome (ARDS). A high fraction of inspired oxygen generates free oxidant radicals, which can damage endothelial and type 1 pneumocytes. NOTE: Clinicians should be aware of possible drug synergisms, such as a combination of a high fraction of oxygen with bleomycin or amiodarone, which can cause ARDS.
The role of drugs taken concomitantly may be important. Hazardous associations have been reported with the coadministration of cisplatin and bleomycin, which can increase the risk of bleomycin-induced interstitial lung disease. The combination of vinblastine and mitomycin increases the risk of asthma.
Radiation can result in the production of oxidant radicals that lead to pulmonary damage. Radiation therapy in combination with chemotherapy may be synergistic. [3]
Occupational exposure to pulmonary toxins can increase the risk of drug-related adverse effects. Asbestos exposure may potentiate the noxious respiratory effects of ergot drugs and bleomycin. [4, 5]
In general, patients with preexisting lung disease are at an increased risk for drug toxicity. For example, rheumatoid pneumonitis may increase the relative risk of developing respiratory disease from disease-modifying drugs.
Etiology
Drug-induced lung disease can be categorized in terms of major clinical syndromes, as follows:
-
Interstitial pneumonitis
-
Noncardiac pulmonary edema (NCPE) / capillary leak syndrome
-
Hypersensitivity reaction
-
Cryptogenic pulmonary edema (COP) (previously referred to as bronchiolitis obliterans-organizing pneumonia [BOOP])
-
Pulmonary vascular disease
-
Bronchospasm
-
Pleural involvement
-
Mediastinal involvement
Interstitial pneumonitis
Interstitial pneumonitis (ie, inflammation of the lung interstitium, such as the alveolar septa) is the most common manifestation of drug-induced lung disease. A wide array of drugs can cause interstitial pneumonitis. Some of the agents implicated are azathioprine, bleomycin, chlorambucil, MTX, phenytoin, statins, amiodarone, and sulfasalazine. [6, 7]
Time to onset is is unpredictable, from a few days to years into treatment, and may be progressive over a few weeks, with isolated fever followed by the insidious development of respiratory symptoms, or the onset may be abrupt, especially in cases caused by MTX. Signs and symptoms include increasing dyspnea, dry cough, high fevers and, occasionally, a rash. The spectrum of severity ranges from mild symptoms and ill-defined pulmonary opacities to extensive consolidation and respiratory failure.
NCPE / capillary leak syndrome
A variety of drugs can cause NCPE. This is a less common pattern of drug-induced involvement than pneumonitis and fibrosis. Drugs can cause pulmonary edema by two mechanisms. First, some drugs cause injury to the capillary endothelium, leading to leakage of fluid and protein into the lung interstitium. Second, certain drugs depress the central nervous system (CNS), resulting in neurogenic pulmonary edema.
Clinically, acute NCPE (ie, acute pulmonary edema with no evidence for left ventricular dysfunction or overload) manifests as an acute onset of dyspnea with tachypnea, tachycardia, hypoxemia, and diffuse crackles on physical examination. Fluffy infiltrates are present on the chest radiograph.
Drugs that cause NCPE include the following [8] :
-
Heroin
-
Interleukin 2
-
Methotrexate (MTX)
-
Cocaine
-
Tocolytic agents
-
Hydrochlorothiazide
-
Cyclophosphamide
-
Iodinated radiographic contrast agents
Hypersensitivity reaction
Drug hypersensitivity results from interactions between a pharmacologic agent and the patient’s immune system. These reactions are commonly associated with nitrofurantoin, MTX, beta-blockers, and procarbazine. Drug-mediated hypersensitivity reactions manifest as an acute syndrome consisting of dyspnea, fever, and nonproductive cough. Peripheral eosinophilia may be present, and the chest radiograph shows localized or bilateral alveolar infiltrates.
Cryptogenic pulmonary edema
COP is a distinctive pattern of lung response to a few drugs. Histology reveals interstitial inflammation superimposed on the dominant background of alveolar and ductal fibrosis. Drugs that can cause COP include the following:
-
Acebutolol
-
Amiodarone
-
Amphotericin B
-
Bleomycin
-
Carbamazepine
Pulmonary vascular disease
Drugs can affect the pulmonary vascular circulation by causing venous thromboembolism, pulmonary hypertension, vasculitis, or pulmonary veno-occlusive disease. Pulmonary veno-occlusive disease is characterized by chronic congestive changes, mild-to-moderate arterial hypertensive changes, and obstruction of small pulmonary veins. Oral contraceptives, [9] bleomycin, and carmustine (BCNU) have been reported to cause this rare disorder.
Oral contraceptives also cause a 4- to 7-fold increased risk of venous thromboembolism. [10] The mechanism responsible for this effect is not known, but estrogens are well known to increase platelet adhesiveness and decrease venous tone and can cause a procoagulant effect. Other implicated drugs include phenytoin, procainamide, and retinoic acid.
Appetite suppressants (eg, amphetamines, fenfluramine) are associated with an increased risk of pulmonary hypertension. The anorectic agent aminorex was removed from the market for this reason. Clinicians should remain vigilant because most over-the-counter appetite suppressants contain fenfluramine and dexfenfluramine. [11] Prescription medications such as beta-blockers and mitomycin C have also been reported to cause pulmonary hypertension.
Several drugs cause pulmonary vasculitis, including nitrofurantoin, sulfonamides, penicillins, phenytoin, and propylthiouracil. This disorder is likely a form of hypersensitivity pneumonitis.
Drug-induced pulmonary hemorrhage is a rare drug-related complication. Patients usually present with hemoptysis, dyspnea, and hypoxemia. Diffuse alveolar hemorrhage is characterized by bilateral infiltrates in the context of anemia of recent onset and hypoxemia.
Several anticoagulants and cytosine arabinoside can produce diffuse alveolar hemorrhage. [12] Penicillamine, amiodarone, cocaine, hydralazine, mitomycin C, nitrofurantoin, abciximab, MTX, carbamazepine, and moxalactam disodium are recognized as inciting agents. The diagnosis of diffuse alveolar hemorrhage is confirmed by bronchoalveolar lavage (BAL), which shows increased blood staining in sequential aliquots. Treatment is withdrawal of the offending drug and control of the bleeding.
Bronchospasm
Aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs) can induce bronchospasm (8-20% of adults with asthma). In rare cases, this reaction can lead to death in aspirin-sensitive persons with asthma. Asthma and aspirin sensitivity may develop in the months following the initial exposure to aspirin or NSAIDs. The acute asthmatic reaction occurs within 20 minutes to 3 hours after ingestion of the drug.
Patients initially present with an acute episode of vague malaise, sneezing, nasal obstruction, rhinorrhea and, often, a productive cough. These symptoms resolve in a few weeks but may be followed by persistent rhinitis and the development of nasal polyps. Spirometry typically shows a variable obstructive ventilatory defect.
Bronchospasm has also been reported with the use of the following agents:
-
Inhaled pentamidine
-
Amphotericin B
-
Amiodarone
-
Angiotensin-converting enzyme (ACE) inhibitors (ACEIs)
-
Dipyridamole
-
Nitrofurantoin
-
Beta-blockers
-
Penicillamine
Because infection with human immunodeficiency virus (HIV) is now better controlled and patients are treated for many years, further study of antiretroviral therapy (ARVT) and lung function will determine whether bronchospasm reverses after cessation of ARVT. In one study of pulmonary function abnormalities in patients with HIV receiving ARVT, univariate analysis demonstrated that ARVT is a risk factor for airway obstruction unresponsive to bronchodilator treatment, with an odds ratio of 4.71. [13]
Pleural involvement
Pleural effusions can develop in patients undergoing treatment with MTX, nitrofurantoin, amiodarone, procarbazine, carmustine, or cyclophosphamide and dasatinib. Pleural effusions can also occur in drug-induced lupus; medications in this setting include hydralazine, procainamide, phenytoin, nitrofurantoin, and ACEIs. Positive serum testing for antinuclear and histone antibodies aids in the diagnosis of this disorder. Some medications cause eosinophilic pleural effusions.
Bilateral pleural thickening is a distinctive form of late cyclophosphamide toxicity. Pneumothorax can complicate late stages of drug-induced pulmonary changes and has been reported in association with bleomycin, carmustine, and retinoic acid.
Mediastinal involvement
Phenytoin, bleomycin, and carbamazepine can induce enlargement of hilar and mediastinal lymph nodes. In addition, a pseudosarcoidosis syndrome can develop with interferon alfa and beta.
Mediastinal lipomatosis is the accumulation of excess unencapsulated fat within the mediastinum. It may be seen in patients with Cushing disease or those treated with corticosteroid therapy. The usual appearance on the chest radiograph is a smooth widening of the anterior and superior mediastinum without any deformity of the trachea. The fat pads in the costophrenic angles are also often enlarged. The diagnosis is made based on chest computed tomography (CT) scan findings. The treatment is cessation of steroid therapy.
Drug classes
Selected drugs that are important causes of pulmonary toxicity fall into the following classes:
-
Cytotoxic
-
Cardiovascular
-
Anti-inflammatory
-
Antimicrobial
-
Illicit
-
Cancer immunotherapies
-
Miscellaneous
Cytotoxic drugs
Bleomycin
Bleomycin is very useful in the treatment of head and neck carcinomas, germ cell tumors, and lymphoma. However, the rate of bleomycin-induced pulmonary toxicity is approximately 10% (range, 2-40%).
Risk factors for lung toxicity with bleomycin include the following:
-
Old age
-
Cumulative dose greater than 450 total units (10% mortality if >550 total U)
-
Concomitant or prior radiation therapy (Lung injury may not be confined to the radiation port.)
-
Exposure to a high supplemental fraction of inspired oxygen (>0.25-0.3), [14] which can lead to the development of ARDS 18-36 hours after exposure
-
Combination therapy with cyclophosphamide or granulocyte-colony stimulating factor
-
Renal failure [15]
A wide variety of adverse reactions to bleomycin have been reported, including chronic interstitial fibrosis, hypersensitivity-type disease, and COP. Clinically, bleomycin toxicity manifests acutely or subacutely with dyspnea and chest pain. [16] Pneumonitis with pulmonary fibrosis [17] can develop 6-8 weeks after the onset of treatment. [18] Crackles may be present upon chest auscultation; their presence precedes radiographic changes.
Chest radiographs may show reticulation, ground-glass opacity and, occasionally, consolidation with a subpleural and lower lobe predominance. [19, 20] Often, generalized loss of lung volume occurs. [21] Lung toxicity can cause multiple pulmonary nodules, [22] which may mimic metastatic disease [23] but have the histologic characteristic of COP.
Pulmonary function testing (PFT) results typically reveal a restrictive ventilatory defect and a reduced diffusion capacity of the lungs for carbon monoxide (DLCO) that predates the onset of overt toxicity by weeks. The BAL cytologic pattern is neutrophilic. [24] Tissue eosinophilia is uncommon but has been reported in patients with bleomycin-induced lung toxicity. [25]
Management includes withdrawal of the drug. Corticosteroids are generally administered to all patients with clinically significant toxicity; then, they are slowly tapered according to the patient’s clinical response. Clinical improvement typically occurs within weeks, but the condition may take 2 years to completely resolve. The overall mortality rate varies from 10% to 83%.
Mitomycin C
MItomycin C is used in the treatment of breast, gastrointestinal, gynecologic, and lung carcinomas. The rate of pulmonary mitomycin C toxicity is approximately 3-12%. Pulmonary disorders that have been described with mitomycin C toxicity include the following:
-
Acute pneumonitis
-
Hemolytic-uremic–like syndrome with acute lung injury
-
Chronic pneumonitis with the insidious development of diffuse parenchymal lung disease
-
Exudative pleural exudative effusions
A fraction of inspired oxygen value greater than 50% increases the risk for pulmonary mitomycin C toxicity. Coadministration with vinca alkaloids (eg, vinblastine, vincristine) can cause bronchospasm and hypoxia.
Symptoms of pulmonary mitomycin C toxicity typically appear after the third or fourth course of chemotherapy. Chest radiographs may reveal a reticular pattern and opacities. These pulmonary opacities may clear, or they may persist in patients who progress to the development of chronic interstitial lung disease (ILD).
Approximately two thirds of the patients develop chronic respiratory symptoms that respond to corticosteroids. The mortality rate is high (≤50%).
Nitrosourea (BCNU, carmustine)
The rate of pulmonary toxicity with nitrosourea is 20-30%, with a 90% mortality. BCNU readily crosses the blood-brain barrier and is often used in patients with CNS malignancies—This agent causes pulmonary toxicity more often than any other nitrosourea.
BCNU may have synergy with other drugs (eg, cyclophosphamide) and radiation therapy in producing pulmonary toxicity. In addition, the following factors increase the risk of toxicity:
-
Younger age
-
Preexisting lung disease
-
Smoking habit
-
Dose greater than 525 mg/m2 (50% affected at dose >1500 mg/m2)
Symptoms may develop as soon as 1 month after treatment or up to more than 10 years after treatment. [26] Patients presenting with BCNU-induced pulmonary toxicity typically have nonproductive cough and dyspnea associated with reticular nodular interstitial infiltrates on their chest radiographs. [27] PFT results include reduced forced vital capacity (FVC), total lung capacity (TLC), and DLCO values. The reduced DLCO value can occur in patients with normal chest radiographs.
Treatment of BCNU-induced pulmonary toxicity is with corticosteroids. [28] Patients presenting early with acute pulmonary toxicity due to BCNU are more responsive to corticosteroid therapy and have a better prognosis. In contrast, late toxicity is characterized by pulmonary fibrosis and a poor therapeutic response. A long-term complication with BCNU toxicity is the development of upper lobe fibrosis.
Cyclophosphamide
Cyclophosphamide is an alkylating agent used in the treatment of various forms of leukemias and lymphomas, and as a conditioning agent prior to bone marrow or stem cell transplantation. The rate of cyclophosphamide-induced pulmonary toxicity is generally less than 1%.
Risk factors for cyclophosphamide lung toxicity include concomitant radiation therapy, use of other cytotoxic agents known to be associated with lung toxicity (eg, bleomycin), and exposure to high oxygen concentrations.
The two distinct clinical patterns of pulmonary toxicity associated with cyclophosphamide are (1) an acute pneumonitis that occurs early in the course of treatment and (2) a chronic, progressive, fibrotic process that may occur after prolonged therapy. If diagnosed early, the acute form of cyclophosphamide pulmonary toxicity is largely reversible upon removal of the drug and institution of corticosteroid therapy.
Chronic cyclophosphamide pneumonitis takes the form of progressive pulmonary fibrosis with respiratory failure and, occasionally, digital clubbing. Chronic cyclophosphamide pneumonitis is typically irreversible, even with drug withdrawal and the institution of corticosteroid therapy. [29]
Bilateral reticular or nodular diffuse opacities are the hallmark of both early- and late-onset pulmonary toxicity. In the case of early-onset pneumonitis, chest CT scans reveal ground-glass opacities predominantly in the periphery of the upper lungs. The radiographic opacities of late-onset pneumonitis have a more fibrotic appearance on CT scans, involving mostly the mid and upper lung regions. Pneumothorax may develop late in the course of the disease. PFTs typically display a restrictive pattern with a reduced DLCO.
It is important to rule out infection, particularly Pneumocystis jiroveci pneumonia, when evaluating a patient for cyclophosphamide-induced pulmonary toxicity, as both conditions may be present in these patients. In general, treatment of cyclophosphamide-induced pulmonary toxicity is largely supportive, but lung transplantation may be considered.
Busulfan
Busulfan is an alkylating agent used to treat myeloproliferative disorders. Currently, this drug is almost exclusively administered as part of preparative regimens prior to stem cell transplantation. The rate of busulfan lung toxicity is approximately 5%.
Risk factors for toxicity are synergistic pulmonary damage when exposed to oxygen, radiation, or other cytotoxic chemotherapeutic drugs. The time of onset of busulfan lung toxicity ranges from a few months to 10 years. Common clinical manifestations are cough, progressive dyspnea with exertion, fever, weight loss, and brownish pigmentation of the skin.
Chest radiographs may be normal, or they may reveal bibasilar reticular opacities. Busulfan toxicity can cause a radiologic pattern similar to that of alveolar proteinosis. [30] PFT results reveal a restrictive ventilatory defect and a reduced DLCO.
Treatment is withdrawal of the drug and corticosteroid therapy. Anecdotal reports describe responses to corticosteroids, but no controlled studies are available. Generally, the prognosis is poor, with a 50-80% mortality.
Methotrexate
MTX is an antifolate that is part of several antineoplastic chemotherapy regimens. The incidence of MTX pulmonary toxicity is 0.3-12%.
Risk factors for MTX-induced lung toxicity include the following:
-
Age older than 60 years
-
Rheumatoid pleuropulmonary involvement
-
Previous use of disease-modifying antirheumatic drugs
-
Hypoalbuminemia (either before or during therapy)
-
Diabetes mellitus
-
Daily rather than weekly drug administration
-
Preexisting lung disease
-
Abnormal PFT results prior to therapy
-
Decreased elimination of MTX (eg, renal failure)
Symptoms usually develop within weeks of the onset of treatment and include fever, dyspnea, persistent nonproductive cough, and/or rash. Patients may also have fatigue and weight loss. Then, typically, the disease accelerates, producing a brisk development of infiltrative lung disease, resulting in respiratory failure. Severe hypoxemia is consistently present. Mild peripheral eosinophilia is present in 40% of patients.
Nonspecific interstitial pneumonia (NSIP) is the most common manifestation of MTX-induced lung disease. Other histopathologic patterns include BOOP, NCPE, and non-Hodgkin (B-cell) lymphoma. Interestingly the non-Hodgkin lymphoma usually regresses after cessation of MTX therapy.
Chest radiographs reveal ill-defined reticular opacities, ground-glass opacity, or consolidation. [31] A basal prominence is typical. High-resolution CT scanning may demonstrate ground-glass changes as prominent abnormalities.
PFTs in patients who can tolerate the procedure reveal restrictive ventilatory defects with a low diffusing capacity. Hypoxemia may be present on arterial blood gas (ABG) analysis. BAL may be helpful for excluding an infectious etiology such as P jiroveci pneumonia, [32] and in supporting the diagnosis of MTX pneumonitis. Lymphocytic predominance with an increase in the number of helper T lymphocytes and the helper/suppressor T-cell ratio is observed in the BAL fluid of patients with MTX pneumonitis. [33, 34]
The diagnosis of MTX-induced lung toxicity must be made on the basis of the clinical setting, clinical manifestations, radiographic abnormalities, and BAL results. Occasionally, lung histopathology is necessary.
The diagnostic criteria proposed by Searles and McKendry for MTX-induced toxicity consist of major and minor criteria. [35] Major criteria are as follows:
-
Hypersensitivity pneumonitis based on histopathology, without evidence of pathogenic organisms
-
Radiologic evidence of pulmonary interstitial or alveolar infiltrates
-
Blood cultures (if febrile) and initial sputum cultures (if sputum is produced) that are negative for pathogenic organisms
Minor criteria are as follows:
-
Nonproductive cough
-
Shortness of breath for less than 8 weeks
-
Oxygen saturation up to 90% on room air at the time of initial evaluation
-
DLCO up to 70% of predicted
-
Leukocyte count up to 15,000 cells/µL
Definitive diagnosis of MTX pneumonitis can be made if the patient has one or two major criteria in conjunction with three of the five minor criteria.
The management of MTX pneumonitis includes drug discontinuation. If symptoms and radiographic findings persist despite discontinuation of the drug, corticosteroid therapy is recommended. However, no prospective, randomized, placebo-controlled trials have been performed to support the use of corticosteroids in MTX pulmonary toxicity.
Pulmonary abnormalities from MTX, in contrast to those from many other cytotoxic agents, are often reversible; 85% of affected patients fully recover. Fibrosis of the lungs after MTX pneumonitis is unusual. The overall mortality is 15%. Death is caused by rapidly progressive respiratory failure.
Gefitinib
Gefitinib is a selective tyrosine kinase inhibitor (TKI) of the epidermal growth factor receptor (EGFR) used to treat adults with EGFR mutation-positive non-small-cell lung cancer (NSCLC). Clinical trials have reported a broad range of adverse pulmonary events with ILD most commonly reported. Gefitinib-induced ILD is often life-threatening; its mortality is approximately 30-40%. [36]
Clinical manifestations of gefitinib-induced pulmonary toxicity include an unproductive cough, dyspnea, and serious hypoxemia. The appearance of respiratory symptoms within the first 4 weeks of gefitinib treatment can aid in the diagnosis, which is based on clinical symptoms, characteristic findings of a CT scan, nonprogression of the NSCLC, and a curative effect upon cessation of gefitinib. [37]
Treatment of gefitinib-induced ILD is largely supportive, including supplemental oxygen, empirical antibiotics, and mechanical ventilation. Immediate discontinuation of the drug is strongly recommended. Successful therapy with large-dose corticosteroids has been reported, although no controlled trials have been conducted to evaluate their efficacy. [36, 37]
Dasatinib
Dasatinib is a dual Src and BCR-ABL TKI approved for first-line treatment of Philadelphia-positive chronic myelogenous leukemia (CML) and for all phases of Philadelphia-positive CML with resistance or intolerance to prior therapy, including imatinib. A phase II trial of dasatinib in patients with squamous cell lung cancer was halted early due to unaccaptable toxicity, of which the most common was pleural effusion. [38] Pleural effusion has been seen in 16% to 54% of patients treated with dasatinib therapy; it responds to the use of steroids along with discontinuation of the medication. [39]
Pulmonary arterial hypertension (PAH) has also been associated with dasatinib, with a reported incidence of 0.45% to 1.2%. [11] The pathogenesis is unclear and attributed to off-target effects. Improvement is usually observed upon withdrawal of treatment; however, some patients required specific PAH treatment.
Other TKIs
TAS-121 is a novel third-generation EGFR TKI that has been used to treat patients with EFGR-positive NSCLC. ILD was a dose-limiting toxicity in an open-label, nonrandomized multicenter, dose escalation, phase I study of TAS-121 in 134 Japanese patients with EFGR+ NSCLC. [40] (However, the most common adverse drug reactions were dermatologic toxicity [89.6%], decreased platelet count [67.2%], and pyrexia [44%]). [40]
Crizotinib is an anaplastic lymphoma TKI that targets an echinoderm microtubule-associated protein-like-4-anaplastic lymphoma kinase gene fusion, a mutation found in 2-7% of NSCLC cases. [41] Tereso et al reported the case of a Portugese patient who developed drug-induced ILD following treatment for NSCLC with crizotinib. [41]
Cardiovascular drugs
Amiodarone
Amiodarone is an antiarrhythmic agent used in the treatment of many types of tachyarrhythmia. Although no definitive correlation exists between the development of drug toxicity and the duration of therapy or the total accumulative dose, the risk for amiodarone-induced lung disease may be increased if the daily maintenance dose is over 400 mg and the patient is elderly, or if the duration of therapy exceeds 2 months. Recognized risk factors include preexisting lung disease and a history of thoracic or nonthoracic surgery or pulmonary angiography.
Patients who have developed amiodarone-induced lung toxicity usually present with nonspecific symptoms such as cough, dyspnea, fever, and weight loss. These symptoms may be mistaken for, or obscured by, symptoms of overt cardiac failure in a patient who is critically ill.
Radiologically, amiodarone toxicity can manifest as a focal lesion or diffuse interstitial abnormality. Less commonly, ill-defined nodules or masses that occasionally cavitate can be present. [42, 43]
Bronchoscopy with BAL and biopsy helps exclude infection and typically reveals the presence of foamy macrophages with lamellar inclusions (visualized by electron microscopy). These changes within macrophages are indicative of exposure to amiodarone but do not prove that the drug is the cause of the pulmonary process. Similar changes are seen in asymptomatic persons who are receiving the drug.
Amiodarone pulmonary toxicity is a diagnosis of exclusion. Increased lung attenuation on CT scans, increased gallium uptake, and abnormal PFT results are helpful in the diagnosis but are nonspecific. The combination of high-attenuation abnormalities within the lungs and liver or spleen is characteristic of amiodarone toxicity. A positive gallium scan result is seen in almost all patients with amiodarone pneumonitis and can help to differentiate it from pulmonary embolism and congestive heart failure.
Withdrawal of the drug is the cornerstone of treatment for amiodarone-induced lung disease. Glucocorticoids seem to be useful in more severe or persistent cases. Because of amiodarone's long elimination half-life (approximately 45 d), pulmonary toxicity may initially progress despite drug discontinuation and it may recur upon steroid withdrawal. Radiographic resolution generally occurs over 2 months. Sato et al reported successful treatment of one case with polymyxin beta-immobilized fiber column direct hemoperfusion. [44] Use of veno-venous extracorporeal membrane oxygenation (ECMO) to maintain pulmonary function and vital organ perfusion in a patient with severe amiodarone-induced toxicity has been reported. [45]
Approximately 15% of patients taking amiodarone develop postoperative ARDS. Onset of symptoms begin 2 hours to 2 weeks following sugery. A high fraction of inspired oxygen given during the operation and the postoperative period has been postulated to contribute to this complication [46]
ACEIs
Up to 20% of patients develop a dry cough after taking ACEIs. The exact mechanism of ACEI cough is unknown, but it is thought to be linked to the accumulation of substances normally metabolized by ACE. These substances include bradykinin or tachykinins (with the consequent stimulation of vagal afferent nerve fibers) and substance P. [47, 48, 49, 50, 51]
Resolution of ACEI–induced cough usually occurs within 1-4 days but may take weeks to months. Patients can be switched to an angiotensin receptor blocker (ARB), which rarely induces cough. In addition, sulindac has been reported to be of benefit in the management of ACEI–induced cough. Studies have also suggested that intermediate doses of aspirin (500 mg/d), but not low doses (100 mg/d), can suppress ACEI cough. [52, 53, 54]
Although ACEIs are generally safe in most patients with obstructive airways disease, case reports suggest that in a subpopulation of patients, these agents can increase bronchial reactivity, asthma symptoms, or exacerbations.
Another symptom of ACEI therapy is angioneurotic edema (0.68% of patients). [55] It manifests as swelling of the tongue, lips, and mucous membranes within hours or weeks after initiating treatment and can rapidly evolve into respiratory distress. This complication can be treated with a subcutaneous injection of epinephrine every 15-20 minutes, diphenhydramine, and steroid therapy.
Beta-blockers
Beta-blockers can precipitate bronchospasm in patients with asthma or chronic obstructive pulmonary disease (COPD). [56] The benefits of using beta-blockers, as with any other drug, must be weighed on a case-by-case basis against the risk of adverse effects.
In patients with stable COPD or asthma, beta-blockers can be started at low doses, with careful monitoring for adverse effects. Because of its cardioselectivity, atenolol is the drug of choice for an individual with obstructive airways disease who needs a beta-adrenergic antagonist.
Esmolol is the drug of choice in critically ill patients with asthma or COPD who require a beta-blocker (unstable angina), owing to its beta1 selectivity and extremely short half-life (9 min).
Importantly, ophthalmic beta-blockers, such as timolol, which are used in the treatment of glaucoma, have produced a number of deaths secondary to exacerbation of COPD and asthma. [57] Betaxolol ophthalmic may be a safer alternative to timolol.
Anti-inflammatory drugs
Aspirin
Aspirin-induced asthma (AIA) occurs in less than 1% of healthy individuals and in up to 20% of asthmatic individuals. The pathogenesis of AIA is mediated by the production of potent inflammatory and bronchoconstrictor leukotriene (LT) mediators such as LTC4, LTD4, and LTE4 via activation of the 5-lipoxygenase pathway.
In addition to wheezing, reactions are usually accompanied by nasal and ocular symptoms, including congestion, rhinorrhea, and tearing. Facial flushing, angioedema, and gastrointestinal symptoms can also occur. The Samter triad (or aspirin sensitive asthma, aspirin exacerbated respiratory disease [AERD]) is asthma, nasal polyps, and aspirin sensitivity. The treatment of AIA is steroid therapy and discontinuation of aspirin and NSAIDs.
Among elderly patients on long-term aspirin therapy, 10-15% develop NCPE. It usually occurs when the serum salicylate level is greater than 40 mg/dL. Treatment is usually supportive, but some patients require hemodialysis. Long-term salicylate ingestion can manifest as pseudoseptic syndrome (fever, tachycardia, elevated white blood cell count, hypotension, ARDS, and altered mental status). Elevated salicylate levels are helpful in diagnosing this condition.
Gold
Gold-induced drug toxicity is uncommon, occurring in 1% of patients. Toxicity occurs within 2–6 months after therapy is started and is associated with mucocutaneous lesions in 30% of patients. Diffuse alveolar damage (DAD) and NSIP are the most common manifestations of gold-induced lung disease. Note that pleural effusion is not associated with gold toxicity.
Toxicity from gold therapy can also affect other organs, such as the skin (dermatitis), the nerves (peripheral neuropathy), and the kidneys (proteinuria).
Treatment of gold toxicity is withdrawal of the agent and, in severe cases, steroid therapy. The prognosis is good. Most patients improve after discontinuation of the gold therapy.
Penicillamine
Penicillamine is an anti-inflammatory agent mostly used in the treatment of rheumatoid arthritis. It can cause bronchiolitis obliterans, penicillamine-induced systemic lupus erythematosus, pulmonary-renal syndrome, and pneumonitis. Management includes withdrawal of the drug, supportive therapy, and consideration of a trial of corticosteroids. In general, the prognosis is poor.
Antimicrobial drugs
Nitrofurantoin
Nitrofurantoin, an antibacterial agent used primarily for the treatment of urinary tract infections, is one of the most common causes of drug-induced lung disease. Both acute and chronic pulmonary toxicity can occur, but the acute syndrome is much more common.
The mechanism of the acute nitrofurantoin reaction is unknown, and it is not dose dependent. The acute pleuropulmonary reaction begins 2-10 days after the initial drug exposure and is manifested by dyspnea and cough. Fever is present in most cases. Pleurisy occurs in one third of patients.
The chest radiograph shows a pattern of basilar alveolar or interstitial infiltrates, [58] sometimes accompanied by a pleural effusion. Peripheral blood eosinophilia and elevation in the sedimentation rate are seen in one third and nearly one half of the patients, respectively. The prognosis is good, with most patients recovering in 1-4 days after discontinuation of nitrofurantoin therapy.
Chronic toxicity is far less common than the acute reaction and is not associated with systemic symptoms. Chronic pulmonary toxicity typically manifests clinically as an insidious onset dyspnea and cough. Clinically and radiographically, it is indistinguishable from idiopathic pulmonary fibrosis and typically causes no pleural effusion. PFTs demonstrate a restrictive ventilatory defect. If no improvement is noted within 2-3 months after withdrawal of the drug, corticosteroid therapy is indicated.
Sulfasalazine
Sulfasalazine is an antimicrobial drug used for the treatment of inflammatory bowel disease. It can cause eosinophilic pneumonia, desquamative interstitial pneumonitis, NCPE, drug-induced lupus syndrome, and vasculitis, usually after 1-8 months of therapy. More than 50% of patients have peripheral eosinophilia. Management includes removal of the drug and, if necessary, corticosteroid treatment.
Illicit drugs
Cocaine
Cocaine is one of the most frequently used illicit drugs in the United States. Inhalation of cocaine may result in pneumomediastinum and pneumothorax. [7, 59, 60] Smoking of cocaine is associated with the following effects:
-
Acute exacerbations of asthma
-
Bronchiolitis obliterans
-
Cardiogenic pulmonary edema
-
NCPE
-
Interstitial pneumonitis
-
Pulmonary vascular hypertension
-
Pulmonary hemorrhage
-
Talcosis
-
Thermal injury to the airway
-
Pneumothorax
-
Significant impairment of the diffusing capacity of the lungs
Heroin
Heroin can cause acute NCPE, which can occur with the first use of the drug. The exact mechanism of heroin-induced NCPE is unknown, but a postulated mechanism is the direct toxic effect of heroin on the alveolar capillary membrane, which leads to increased permeability, and effects on the central nervous system. This, in turn, leads to a hypoxic effect on the alveolar capillary membrane, resulting in increased capillary permeability.
Other complications of heroin use are septic emboli from infected thrombophlebitis or endocarditis and aspiration pneumonia. Persons with long-term heroin abuse may experience repeated episodes of aspiration pneumonia, leading to bronchiectasis and narcotizing bronchitis. Treatment is supportive.
Naloxone can be used to reverse respiratory depression. Interestingly, several case reports describe acute NCPE related to naloxone, although the mechanism remains unknown. [61]
Cancer immunotherapies
Immune checkpoint inhibitors
Immune checkpoint inhibitors help to prevent self-destructive immune responses. Tumor cells are capable of evading these immune responses via overexpression of the ligands of checkpoint receptors, bringing T cells to a state of nonresponsiveness or exhaustion.
By deactivating the function of checkpoint inhibitors, the body may have increased anti-tumor immunity. However as collateral damage, there could be heightened immune activity against host antigens, leading to possible immune-related toxicities everywhere in the body—including the lungs. [62]
Increasing reports of multiple forms of pulmonary toxicity related to these medications are occuring.
Ipilimumab (CTLA-4) (FDA approved 2011)
There is preliminary evidence of ipilimumab-related pulmonary toxicity. In a study by the University Hospital of Zurich in which serial spirometries and measurements of DLCO in 71 patients with metastatic melanoma before and during treatment of ipilimumab were collected, there was a reduction of at least 10% in FVC and at least 15% in DLCO. [63] In addition, clinically meaningful lung function decline at 3 weeks (9%), 6 weeks (11%), and 9 weeks (24%) was noted. Ipilimubab in combination with nivolumab has also had a reported incidence of anti-programmed death (PD)-1–related pneumonitis. [64]
Pembrolizumab (PD-1) (FDA approved 2014 ) and atezolizumab (programmed death ligand [PDL]-1) (FDA approved 2016)
Three cases of pembrolizumab-induced pneumonitis were reported in 2017. [65] It is proposed that the triggering of pneumonitis may be facilitated by preexisting local inflammation in the lungs.
Atezolizumab-induced pneumonities has been reported in phase II and III trials involving patients with NSCLC, [66] as well as in case reports in those with urethral cancer.
Nivolumab (PD-1) (FDA approved 2014)
Nivolumab has been implicated in pulmonary sarcoid-like granulomatosis D and organizing pneumonitis. [67, 68]
Durvalumab (PDL-1) and avelumab (PDL-1) (FDA approved 2017)
There is limited mention of durvalumab and avelumab specifically associated with checkpoint inhibitor-related pneumonitis in the literature. However, one unique report exists of a patient with cervical cancer treated with durvalumab in combination with cediranib who developed right heart failure and pulmonary hypoxemia from pulmonary tumor thrombotic microangiopathy. [69] Although the report does not make a suggestion of PD-1 and PDL-1 inhibitors causing pulmonary hypertension, these agents may act synergistically with other chemotherapeutic agents (in this case, vascular endothelial growth factor [VEGF] inhibitors) to disrupt angiogenesis and promote abnormal vessel formation.
In general, based on a prior meta-analysis of trials, it appears that the incidence of pneumonitis is greater in patients treated with PD-1 than PD-L1 inhibitors. [70] Furthermore, the analysis concluded there was a higher incidence of all grade pneumonitis in treatment-naive patients exposed to PD-1 inhibitors compared to those previously treated for their disease.
Chimeric antigen receptor (CAR) T cells
Tisagenlecleucel and axicabtagene ciloleucel
CAR-T therapy uses T cells that have been genetically modified to express chimeric antigen receptors, or CAR T cells, targeting the B-cell antigen CD19. The most common acute and serious toxicity of CAR T cells is cytokine release syndrome. In severe cases, this syndrome may lead to capillary leakage, renal and hepatic dysfunction, and cardiopulmonary compromise. [62] There have been no explicit case reports of CAR-T related pulmonary toxicity—however, these novel therapies have only been FDA approved for adult B-cell non-Hodgkin lymphoma or childhood acute lymphoblastic leukemia as of mid 2018. [71]
Miscellaneous drugs
Talc
Talcosis is the development of a foreign body granulomatous reaction and is also termed "intravenous (IV) drug abuser’s lung." It results from IV injection of oral preparations containing particulates of talc. Talc can cause granulomatous pulmonary artery occlusion or granulomatous interstitial fibrosis. Patients present with dyspnea, syncope, or signs of right-sided heart failure.
Chest radiographs may be normal in approximately 50% of cases. They can also demonstrate diffuse micronodular densities mimicking alveolar microlithiasis. Talc can also cause nodular lesions in the upper pulmonary lobes, resembling progressive massive fibrosis or pneumoconiosis.
PFT results may reveal a mixed obstructive and restrictive ventilatory defect with decreased DLCO.
Funduscopic examination is helpful by disclosing typical changes of talcosis. Talc emboli can be identified near the macula within the small vessels in 50% of affected patients.
Tocolytics
Tocolytics (ie, terbutaline, albuterol, ritodrine) are mainly used in the treatment of premature labor. Tocolytics act on the beta-receptors of the vessels and cause peripheral vasodilation. If tocolytics are discontinued abruptly, the vasodilated vessels return to their normal vascular tone; this promotes large increases in intravascular volume, which causes NCPE.
The risk factors for the development of NCPE in this setting include the following:
-
Use of corticosteroids
-
Fluid overload
-
Twin gestation
-
Multiparity
-
Anemia
-
Silent cardiac disease
Tocolytic-induced NCPE is treated with diuretics and supportive therapy. Corticosteroids are not helpful.
Epidemiology
Estimating the exact frequency of drug-induced lung diseases is difficult because of the lack of recognition by clinicians and nonspecific diagnostic test results, and because this is a diagnosis of exclusion. Several studies suggest that drug-induced pulmonary toxicity is underdiagnosed worldwide.
In the United States, more than 2 million cases of adverse drug reactions occur annually, including 100,000 deaths. An estimated 0.3% of hospital deaths in the United States are drug related. [72] As many as 10% of patients who receive chemotherapeutic agents develop an adverse drug reaction in their lungs. [73] These figures, however, probably underestimate the true frequency of the problem.
Racial differences in incidence
Bortezomib, a proteosome inhibitor with good clinical activity in persons with multiple myeloma, can lead to severe pneumonitis in black patients. [74] Additionally, some diseases are more common in certain ethnic groups. For example, sarcoidosis is more common in black persons. The incidence of drug-induced pulmonary toxicity is high in black patients taking medications to treat sarcoidosis (ie, methotrexate toxicity in sarcoid patients).
Sex- and age-related differences in incidence
The person’s sex is not an independent risk factor for the development of drug-induced lung disease. However, certain diseases are more common in females, and females will have more adverse effects relative to males. Similarly, amiodarone lung toxicity is more common in males, but this may be related to the fact that amiodarone is used more often in males, rather than a sex-specific predilection.
In general, both extremes of age (ie, childhood and old age) are associated with an increased risk of drug toxicity. In the case of bleomycin, advanced age is one of the major factors responsible for the development of lung fibrosis.
Prognosis
The prognosis of drug-induced pulmonary toxicity is variable and depends on the specific drug and the underlying clinical, physiologic, and pathologic severity of the lung disease. Complications include the following:
-
Pulmonary fibrosis
-
Respiratory failure requiring mechanical ventilation
-
Pulmonary embolism
-
Pulmonary hypertension
-
Pneumothorax
-
Increased incidence of pneumonia
Failure to recognize a drug-mediated lung disease can lead to significant morbidity and mortality. The following are some examples of drug-associated mortality:
-
Death attributable to amiodarone adult respiratory distress syndrome (ARDS) occurs in 10% of cases. [46]
-
The overall rate of bleomycin pulmonary toxicity is 10%; cases are fatal in 1-2%.
-
Cyclophosphamide-induced pulmonary fibrosis has a mortality rate approaching 50%.
-
Approximately 7% of patients with methotrexate-induced hypersensitivity reactions develop chronic fibrosis, and 8% die of progressive respiratory failure.
-
Cytosine arabinoside, an antimetabolite used to treat acute leukemia, causes noncardiac pulmonary edema (NCPE) in 13-20% of patients; mortality ranges from 2% to 50%.
-
The incidence of symptomatic busulfan-induced pulmonary fibrosis is approximately 4-5%, with mortality ranging from 50% to 80%.
-
Bis -chloroethylnitrosourea (BCNU), or carmustine, causes pulmonary fibrosis, with a near 90% mortality.
-
This image is a standard nonenhanced axial thoracic computed tomography scan. There is left lower lobe consolidation with some loss of volume and an air bronchogram. Transbronchial lung biopsy confirmed the diagnosis of cryptogenic organizing pneumonia (also known as bronchiolitis obliterans-organizing pneumonia [BOOP]).
-
Cryptogenic organizing pneumonia (also called bronchiolitis obliterans-organizing pneumonia [BOOP]) is often patchy and peribronchiolar. The proliferation of granulation tissue within small airways and alveolar ducts is excessive and is associated with chronic inflammation of the surrounding alveoli.
-
This image is a computed tomography scan of a patient with sarcoidosis. The pattern of multiple nodules seen here can manifest in patients taking medications that can cause granulomatous reactions.
-
This histology image from a lung biopsy specimen was obtained from the patient with sarcoidosis discussed in the previous image (see the computed tomography scan illustrating multiple nodules). Multiple areas of noncaseating granulomas are present. Drugs such as methotrexate, nitrofurantoin, procarbazine, and pentazocine can cause granulomatous lung disease.
-
This is a close-up histologic view of a noncaseating granuloma with a giant cell.
-
This histologic section of the lung shows diffuse alveolar damage in a patient with adult respiratory distress syndrome.
-
In usual interstitial pneumonitis or idiopathic pulmonary fibrosis, subpleural and paraseptal inflammation is present, with an appearance of temporal heterogeneity on histologic examination. Patchy scarring of the lung parenchyma and normal, or nearly normal, alveoli interspersed between fibrotic areas are the hallmarks of this disease. In addition, the lung architecture is completely destroyed.
