Practice Essentials
Primary mediastinal B-cell lymphoma (PMBCL) is relatively rare B-cell non-Hodgkin lymphoma that comprises 6–12% of all diffuse large B-cell lymphomas (DLBCLs) and 2–4% of all non-Hodgkin lymphomas. PMBCL affects young adults in their third to fourth decade of life and has a slight female predominance. [1] Clinically, PMBCL is characterized by signs and symptoms due to local compression by a rapidly growing mass in the anterior mediastinum; these include superior vena cava syndrome, cough, dyspnea, hoarseness, and dysphagia. B symptoms (fever, weight loss, night sweats) may also be present. [2]
PMBCL was initially recognized in the Revised European-American Classification of Lymphoid Neoplasms (REAL) as a subtype of DLBCL that involves the mediastinum. However, PMBCL became a fully recognized separate entity in 2001 when the World Health organization (WHO) identified that PMBCL represents a distinct clinicopathologic disease and should be classified as such.
Gene expression studies have confirmed that PMBCL is molecularly different from DLBCL and that it may resemble Hodgkin lymphoma. [3, 4, 5] Because of its skewed age distribution, PMBCL accounts for a much higher proportion of lymphomas in patients who have undergone autologous hematopoietic stem cell transplantation (auto-HSCT). Importantly, the majority of patients are cured with modern intensive combination chemoimmunotherapy that is often followed by either involved-field radiation or auto-HSCT.
Pathology and Etiology
The tumor cells resemble immunoblasts or centroblasts, and, in many cases, sclerosis and fibrosis can be identified. Flow cytometry studies identify a unique immunophenotype profile for primary mediastinal B-cell lymphoma (PMBCL). Malignant cells express B-cell antigens (CD20, CD19, CD22, and CD79a), and, in some patients, weak CD30 expression is noted. The weak CD30 expression can aid in differentiating PMBCL from anaplastic large cell lymphoma and classic Hodgkin lymphoma. This is critical, as Reed-Sternberg–like cells can be present in patients with PMBCL. Additionally, the malignant cells also lack CD15 expression but have frequent positivity of the transcriptional regulators BCL6, PAX5, and BOB1.
PMBCL is hypothesized to originate from the germinal or postgerminal centers; however, surface immunoglobulin expression is frequently absent.
Several studies have explored the underlying genetic and molecular features that lead to the evolution of primary mediastinal B-cell lymphoma (PMBCL). Gene expression profiling has clearly demonstrated that this disease entity is different from diffuse large B-cell lymphoma (DLBCL) and has identified several deregulated pathways involved in the pathogenesis of PMBCL. Steidl and Gascoyne eloquently summarized the recurrent gene alterations involved in the pathogenesis of PMBCL. [10]
Gene expression profiling has demonstrated overexpression of genes encoding the NF-kappa-B pathway, suggesting its involvement in the pathogenesis of PMBCL. Further, inhibiting I-kappa-B, which activates NF-kappa-B signaling, was shown to induce cell kill in vitro in PMBCL cell-lines.
Chromosomal gains and amplifications of the REL gene locus on band 2p16.1 have been found in 50% of cases. [10, 11, 12] Other chromosomal aberrations that affect NF-kappa-B pathways include BCL-10 (1p22) and MALT-1 (18q21).
Song et al identified a tumor suppressor gene that encodes the A-20 protein, which acts as an inhibitor to the NF-kappa-B pathway downstream from the tumor necrosis factor (TNF) receptor. [13] Mutations in that gene have been found in over 30% of PMBCL cases, but it has also been described in other lymphoid malignancies. [14, 15] Another mutated tumor suppressor gene is SOCS1 (suppressor of cytokine signaling). SOCS1 usually acts as an inhibitor to the JAK-STAT6 pathway, preventing continued activation and proliferation. [16] In fact, Mottok et al suggested that SOCS1 deletion mutations were present in 45% of 20 studied patients. [17]
More recent studies have also shown a role of immune deregulation in PMBCL pathogenesis. Specifically, the reduced expression of major histocompatibility II complex genes led to decreased infiltrating cytotoxic T-cells, and some investigators have suggested this can lead to inferior outcomes, arguing that more studies exploring the role of immune escape in PMBCL are warranted. Another mechanism by which PMBCL cells escape immune surveillance has been by overexpressing certain surface molecules such as PD-1 ligands and receptors, which, in turn, leads to inactivating infiltrating effector T cells. [18]
Clinical Presentation
History
Primary mediastinal B-cell lymphoma (PMBCL) patients usually present with a bulky anterior mediastinal mass in their third or fourth decade in life. Superior vena cava (SVC) syndrome is common, and, in some reports, 50-80% of patients can have some form of SVC compromise. Phrenic nerve palsy, dysphagia, hoarseness, and breast swelling (in women) can occur. Shortness of breath can be due to pleural effusion, massive mediastinal mass, pericardial effusion, or airway compression. Systemic symptoms (fever, weight loss, night sweats) occur in 30-47% of patients.
Most patients have localized symptoms that depend on the bulk and extent of the disease; however, if recurrence develops, a hematogenous pattern of spread to parenchymal organs, such as the liver, kidneys, or brain, is common. Signs and symptoms in recurrent disease vary according to the organ involved.
Physical examination
Physical examination may reveal the following:
-
SVC syndrome, with congestion of face and upper extremities and occasional airway compromise
-
Palpable mass in the supraclavicular area
-
Dullness at the lung bases
-
Respiratory distress, especially with direct extension to the lungs
-
Peripheral adenopathy (unusual except in the supraclavicular area)
Performance status should be noted because this is an important prognostic indicator. [19]
Additional findings
Laboratory studies are not diagnostic of PMBL, but over 70% of patients can have elevated lactate dehydrogenase (LDH) levels. By definition, patients do not have bone marrow involvement, and 75-80% of patients are usually staged as having stage I or II disease. Most patients present with bulky disease defined as a mass greater than 10 cm in largest diameter.
Differential Diagnosis
The differential diagnosis of primary mediastinal B-cell lymphoma (PMBCL) includes the following:
Diagnostic considerations
Differentiating PMBCL from other malignancies that involve the mediastinum is extremely important because the diagnosis affects management and outcome. [20] Similarly important is differentiating PMBCL from systemic diffuse large B-cell lymphoma (DLBCL) with mediastinal involvement. This latter entity often affects older patients and usually has involvement of distant lymph nodes (away from the mediastinum) and for some, bone marrow is affected with disease.
Distinguishing Hodgkin lymphoma from PMBCL can be challenging. Both diseases can affect younger adults and both entities can be similar histologically. Flow cytometry studies can be helpful, as many patients with classic Hodgkin lymphoma have neoplastic cells that express CD15 and CD30, while they lack expression of B-cell markers. As mentioned above, PMBCL patients express B-cell markers and have weak CD30 expression.
Despite significant advances, cases continue to be difficult to diagnose. Some patients have features similar to classic Hodgkin lymphoma (CHL) and PMBCL at the same time. These patients are diagnosed with mediastinal gray zone lymphoma (MGZL), which is described as B-cell lymphoma with features intermediate between DLBCL and CHL. Prognosis is worse than that of both CHL and PMBCL. Management of these patients is not well defined, but National Comprehensive Cancer Network (NCCN) guidelines recommend treatment with aggressive DLBCL regimens. [21] Adding rituximab to chemotherapy regimens may be considered, if the tumor cells are CD20 positive. [21, 22]
Workup
Laboratory studies
Perform a complete blood cell count with differential and platelets. Perform an electrolyte panel and liver function tests.
Elevation in the serum lactate dehydrogenase (LDH) or beta-2 microglobulin level value is an adverse prognostic feature and usually is seen in the majority of patients.
The markers alpha-fetoprotein and beta-human chorionic gonadotropin (beta-hCG) are often highly elevated in patients with mediastinal germ cell tumors, constituting an important differential diagnosis in males.
Imaging studies
Obtain a chest radiograph (posteroanterior, lateral). A mass larger than one third the diameter of the thorax is considered bulky and indicates a poor prognosis. This might have therapeutic implications later in treatment if radiotherapy is being considered.
Obtain CT scans (chest, abdomen, pelvis). Extension to the pleura, pericardium, and even the chest wall is common. Invasion of the liver, kidneys, and peripheral lymph nodes is more common at the time of recurrence. On occasion, obtaining a CT scan of the neck and soft tissues might be warranted.
Positron emission tomography (PET) scans are considered standard of care procedure before initiating therapy. PET scans are expected to become negative upon completion of successful treatment. Additional diagnostic or treatment considerations (as discussed below) are suggested if the PET scans remain positive after completion of therapy. Treatment decisions based solely on PET scan results are not encouraged, and patients might need to undergo additional diagnostic procedures to confirm whether the PET scan findings are truly positive.
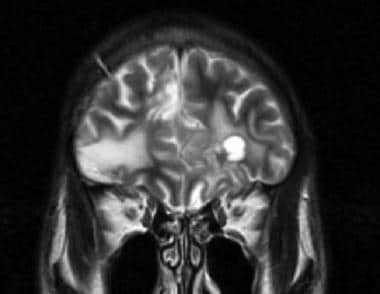
Consider other imaging studies if they are clinically indicated (eg, head CT scan or MRI, if the patient has neurologic problems; see image below). Consider performing a multiple-gated acquisition (MUGA) scan to assess cardiac function before anthracycline-based chemotherapy.
Diagnostic procedures
Adequate diagnostic biopsy is needed and may require surgery to obtain a sufficient sample for accurate diagnosis. Not uncommon, biopsies can initially be nondiagnostic owing to extensive fibrosis and necrosis, and additional studies might be needed. Most commonly, patients either undergo mediastinoscopy or thoracoscopy depending on the location and feasibility. [23]
Ancillary studies, which include immunohistochemistry, immunophenotyping (flow cytometry), and gene rearrangement studies, are often necessary to establish the diagnosis.
Bone marrow aspirate and biopsy are necessary for staging. A unilateral sample is sufficient if the biopsy specimen is larger than 2 cm. By definition, the bone marrow is not usually involved. Patients with marrow involvement might have systemic diffuse large B-cell lymphoma (DLBCL) with secondary mediastinal disease, as opposed to primary mediastinal B-cell lymphoma (PMBCL).
Other tests should be performed if clinically indicated (eg, thoracentesis for pleural effusion, lumbar puncture for neurologic symptoms).
Treatment & Management
For patients with primary mediastinal B-cell lymphoma (PMBCL) who present with superior vena cava (SVC) syndrome, establishing the diagnosis in a timely and efficient manner is critical. Radiation therapy (RT) can alter the pathologic findings and would impair accurate diagnosis; thus, it should be avoided except in extreme circumstances. Patients who are relatively stable should undergo emergent diagnostic evaluation (as summarized above) followed by treatment initiation. [24]
Chemoimmunotherapy
Currently, the most commonly used regimens for PMBCL are as follows [21, 2, 25, 26, 27] :
-
Dose-adjusted EPOCH plus rituximab (DA-EPOCH-R) - Etoposide, prednisone, vincristine (Oncovin), cyclophosphamide, doxorubicin (hydroxydaunorubicin), rituximab; six cycles
-
R-CHOP - Rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone; four or six cycles
After four cycles, R-CHOP may be followed by consolidation with three cycles of ICE (ifosfamide, carboplatin, etoposide) with or without rituximab. After six cycles, R-CHOP may be followed by involved-site radiation therapy (ISRT). [21]
Because PMBCL is rare, few prospective clinical trials have been conducted; consequently, there is no consensus on the optimal chemoimmunotherapy regimen or the use of radiotherapy. [21, 25, 28, 29, 27, 26] A retrospective study by Morgenstern et al in 56 patients with newly-diagnosed PMBCL found that DA-EPOCH-R and R-CHOP/R-ICE provided similar progression-free survival (PFS), overall survival (OS), and complete response (CR) rates; however, R-CHOP/R-ICE was associated with lower toxicity and significantly shorter hospitalization time. [28] A retrospective study by Elhagracy et al in 41 patients found similarly high OS and CR rates with DA-EPOCH-R; these authors prefer R-CHOP to DA-EPOCH-R for low-risk patients with nonbulky disease. [30]
PMBCL is sensitive to radiation therapy (RT), and consolidative RT after chemotherapy can convert patients from a partial response (PR) to CR. However, retrospective studies of RT in PMBCL have yielded conflicting results with regard to benefit. [31] In addition, RT poses risks of long-term adverse effects, such as breast cancer and cardiovascular disease. [26, 32] This is of particular concern because many patients with PMBCL are relatively young, and it may represent a relative disadvantage of R-CHOP, which is often used in conjunction with RT, whereas DA-EPOCH-R is typically administered without RT. [33]
Patients should be evaluated clinically and radiographically to assure continued response. Interim positron emission tomography (PET) scan evaluation is discussed separately below.
Growth factors (filgrastim or peg-filgrastim) may be used, depending on the patient's age and comorbidities. Given the relatively younger age at PMBCL presentation, the authors advocate against the routine use of growth factors as primary prophylaxis. Secondary prophylaxis, however, is recommended to ensure adequate dose density and intensity.
Although a multi-center retrospective analysis found no statistically significant difference in outcome between children and adults with PMBCL treated with DA-EPOCH-R, [34] a phase II trial in children and adolescents with PMBCL found that DA-EPOCH-R did not improve event-free survival compared with a historical controls. [35] A French study of patients younger than 18 years with PMBCL reported 100% 5-year OS in those treated with the risk-based Lymphome Malin de Burkitt (LMB) chemotherapy regimen plus rituximab. [36]
Consolidation therapy and interim PET scans
Prior to the wide use and adaptability to PET scans, most patients underwent consolidative RT or high-dose chemotherapy and autologous hematopoietic stem cell transplantation (auto-HSCT) after completion of systemic therapy. While this approach continues to be commonly used, it has become increasingly controversial, especially in patients who attain complete PET scan negativity upon completion of systemic chemoimmunotherapy.
Several reports have suggested inferior survival in patients with DLBCL who have residual PET scan positivity at the end of chemotherapy and other studies have shown that a positive interim PET scan (after 2-4 cycles of therapy) predicts higher risk of subsequent relapse. [37, 38, 39] However, treatment decisions in patients who remain PET positive after completion of systemic therapy should never be based solely on the PET scan interpretation. In a phase II study by Moskowitz et al in 98 patients with DLBCL, 30% of whom had PMBCL, the majority of patients who remained PET positive had no residual disease when diagnostic biopsies were performed. [40]
Whether RT should be delivered to all patients with PMBCL regardless of PET scan results or whether this approach should be individualized based on PET and/or other clinical or prognostic features remain unknown.
Savage et al reported on the British Columbia experience. [41] CHOP-R followed by consolidative RT was the adapted approach to all PMBCL patients diagnosed and treated from 2001–2005. After 2005, PET scanning was used to guide RT following 6 cycles of CHOP-R. To that end, if the PET scan was negative, patients were observed and if the PET scan was positive, consolidative RT was given. In total, 176 patients were identified: 96 received CHOP-R and 80 received CHOP. For the CHOP-R treated patients, 46 were treated in the “RT era” with 80% receiving RT; 50 were treated in the “PET era”; 38% received RT. Comparing between eras, no overall survival was suggested by adding RT. Further, when PET-positive patients received RT consolidation, no significant difference in outcome was observed between PET-positive and PET-negative patients, suggesting that some patients can avoid undergoing RT when PET is used to guide therapy.
In an attempt to eliminate RT, Dunleavy et al recently reported a phase II trial on 51 patients who were treated with DA-EPOCH-R and showed excellent results. With a median follow-up of 5 years, event-free survival was 93% and overall survival was 97%. For patients who had a PET on this study, the negative predictive value was 100%, while the positive predictive value was 17%. This finding is in line with the data from Moskowitz et al (see above), for which patients have false-positive PET scans after completion of therapy, and underscores the importance of not making therapeutic decisions based on PET findings only. In all, only 2 patients (4%) underwent RT when DA-EPOCH-R was used.
The use of consolidative auto-HSCT in patients with PMBCL stems from the effectiveness of this approach in patients with relapsed DLBCL. [42] Residual disease radiographically was hypothesized to represent persistent lymphoma and patients underwent the aggressive salvage therapy as PET scans were not available then. With the advent of PET and continued standardization of its interpretation, The European Society for Medical Oncology (ESMO) guidelines recommend against routine use of auto-HSCT as a primary consolidative approach. [43] Whether patients who have residual disease that is established histologically should undergo RT or auto-HSCT is unknown. Enrolling these patients in clinical trials is an option, if available. Outside of clinical trials, the decision needs to be individualized and would factor prognostic features, morbid conditions, and patients' wishes.
Relapsed/refractory disease
While PMBCL is often cured with standard first-line therapies, approximately 200 patients per year in the United States are diagnosed with relapsed/refractory PMBCL, which has a poor prognosis with a two-year survival of 15%. [44] Due to its rarity, no standard of care has been identified and relapsed/refractory disease is generally treated following protocols for other DLBCL subtypes. [21]
Patients with relapsed disease often have systemic involvement and many also have extranodal disease. These patients are recommended to undergo salvage systemic chemotherapy followed by stem cell collection and subsequent transplantation. Rituximab, ifosfamide, carboplatin, and etoposide (RICE) is a common salvage approach, although other regimens are acceptable. Patients who demonstrate chemosensitive disease (improvement radiographically and on PET) are taken to transplantation. Patients who have refractory disease should be offered participation in a clinical trial, although some can be considered for allogeneic bone marrow transplantation.
PMBCL frequently involves programmed death 1 (PD-1) ligand overexpression, potentially making PMBCL susceptible to PD-1 blockade. Pembrolizumab, a humanized anti–PD-1 monoclonal antibody blocking interaction of PD-1 with its ligands, PD-L1 and PD-L2, demonstrated a high response rate, durable activity, and a manageable safety profile in patients with relapsed/refractory PMBCL, in the phase IB KEYNOTE-013 and phase II KEYNOTE-170 trials. [44] The phase II CheckMate 436 study reported that the combination of the PD-1 immune checkpoint inhibitor nivolumab the and anti-CD30 antibody–drug conjugate brentuximab vedotin has high antitumor activity and a manageable safety profile in relapsed/refractory PMBCL. [45]
Involvement of the JAK/STAT signaling pathway in some cases of PMBCL has provided another optoin for targeted therapy. Preliminary evidence suggests a possible role for the JAK2 inhibitor ruxolitinib and the JAK2/FLT3 inhibitor pacritinib. [27]
The US Food and Drug Administration (FDA) has approved axicabtagene ciloleucel (Yescarta) for treatment of adult patients with certain types of large B-cell lymphoma, including PMBCL, who have not responded to or who have relapsed after at least two other kinds of treatment. [46] Axicabtagene ciloleucel is a chimeric antigen receptor (CAR) T-cell therapy. In the ongoing ZUMA-1 trial of axicabtagene ciloleucel in patients with DLBCL, PMBCL, or transformed follicular lymphoma, response to date has proved durable, median OS is greater than 2 years, and the long-term adverse effects have been manageable. [47]
Treatment in pregnancy
Some patients are young women who may be pregnant at the time of diagnosis. The management of malignancy during pregnancy raises specific and complex issues. Concern for the patient's health needs to be balanced with the potential teratogenicity of the chemotherapy and the radiation administered for diagnostic examinations or as part of treatment. [48, 49]
Termination of pregnancy is often recommended if the diagnosis is made in the first trimester. However, this is not acceptable to all patients. In cases in which pregnancy is continued, the administration of chemotherapy drugs without undue teratogenicity is often possible. Staging and restaging examinations are minimized. Radiography is avoided, and MRI or ultrasonography procedures are used instead.
The administration of corticosteroids may exacerbate problems such as preeclampsia or glucose intolerance. Close collaboration with an obstetrician is required.
Follow-up
The vast majority of patients can be successfully treated in an outpatient setting for front-line care.
After completion of treatment, patients are usually seen in the outpatient clinic at regular intervals of 2-3 months for the first year. Subsequently, patients are seen every 3-4 months until 5 years. The authors recommend seeing patients annually after that indefinitely. Routine surveillance CT scans and/or PET scans are not recommended after establishing complete remission. The authors consider performing CT scans in some cases if the patients request it, especially if they have high likelihood of relapse.
Complications
The chemotherapeutic drugs used for the management of lymphoma have numerous adverse effects. Nausea and vomiting are common but can be avoided with the use of appropriate antiemetics. Hair loss occurs in most patients but is completely reversible after the completion of treatment.
Mild peripheral neuropathy due to chemotherapy is common. Patients experience numbness in fingertips and toes. Motor neuropathy is unusual.
Myelosuppression (bone marrow suppression) and moderate pancytopenia occur after every treatment cycle. Blood counts typically reach their nadir approximately 10 days after the completion of a treatment cycle. Fatigue is common.
Neutropenic fever and infection are common complications of chemotherapy and require immediate treatment. Approximately 10-20% of patients develop excessive neutropenia or an infectious complication. Primary prophylaxis with antibiotics is not recommended, although it is used for some patients. The use of growth factors is discussed above.
Cardiac toxicity due to chemotherapy is unusual but can occur. Cardiac toxicity from anthracyclines is dose dependent and rare in the typical young patient with PMBCL. Serial monitoring with echocardiograms or multiple-gated acquisition (MUGA) scans may be necessary in individual cases. Typically, patients undergo a MUGA scan to evaluate the left ventricular ejection fraction prior to the initiation of chemotherapy. A MUGA scan is performed in most centers only if clinical concerns arise about cardiomyopathy. Patients should not receive more than 400 mg/m2 of doxorubicin in their lifetime. The incidence of cardiomyopathy if this dose is exceeded is 7-8%. The use of cardioprotectant agents may allow the administration of higher doses of anthracyclines, but these cardioprotectant agents might affect the efficacy of chemotherapy. Therefore, cardioprotectant agents are not routinely recommended.
Rituximab is generally safe. It can cause fever and chills, particularly during the first administration. Rare cases of anaphylactic reactions have been reported. Cases of hepatitis B virus (HBV) reactivation that have resulted in fulminant hepatitis and death have been reported. Persons at high risk of HBV infection should be screened before the initiation of rituximab. Carriers of HBV should be closely monitored for clinical and laboratory signs of active HBV infection and hepatitis during and up to several months after rituximab therapy. All patients should have their hepatitis titers checked before rituximab initiation.
Acute adverse effects of radiation are usually limited and include erythema of the skin and, sometimes, radiation pneumonitis.
Late adverse effects related to treatment include decreased fertility, a slightly increased incidence of secondary cancers in radiation fields (especially breast cancer among women treated during adolescence), and a slightly increased risk for secondary leukemia, especially among patients treated with combined-modality therapy (ie, chemotherapy and radiation).
In addition, coronary artery disease may be more common and may have an earlier onset if substantial areas of the heart are exposed to radiation. Smoking and alcohol abuse should be avoided because of their association with cancer and heart disease.
Guidelines Summary
In 2016, the European Society for Medical Oncology (ESMO) released guidelines for the management of PMBCL. [43] The National Comprehensive Cancer Network (NCCN) 2022 guidelines for the treatment of B-cell lymphomas include recommendations for diagnosis and management of PMBCL. [21]
ESMO guidelines require FDG-PET/CT scan to assess disease extent and to obtain better definition of the residual mediastinal masses at the completion of treatment. [43] NCCN guidelines require clinical pathologic correlation to establish a diagnosis of PMBCL. [21]
Treatment
NCCN guidelines recommend the following as first-line treatment regimens [21] :
-
DA-EPOCH-R
-
R-CHOP- Six cycles, followed by ISRT (preferred) or observation
-
R-CHOP/ICE - Four cycles of R-CHOP, followed by consolidation with three cycles of ICE with or without rituximab
ESMO guidelines recommend rituximab in combination with any of the following regimens [43] :
-
CHOP
-
VACOP-B: Etoposide, doxorubicin, cyclophosphamide, vincristine, prednisolone, bleomycin
-
MACOP-B: Methotrexate, doxorubicin, cyclophosphamide, vincristine, prednisolone, bleomycin
-
DA-EPOCH
ESMO also recommends consolidative mediastinal RT (doses in the range 30–36 Gy, in 1.5–2.0 Gy fractions) in patients treated with standard-dose chemoimmunotherapy but could be omitted in patients with a complete metabolic response only after DA-EPOCH-R.
Autologous stem cell transplantation (HDCT/ASCT) is not recommended in patients who achieved complete remission even in initially poor-risk patients who attain an adequate response to initial therapy. [43]
Post-treatment evaluation
Due to the high frequency of false-positive scans, ESMO recommends further investigaton of a positive PET scan before modifying planned therapy. A post-treatment PET/CT response evaluation should not be carried out until at least 5–6 weeks from the last infusion of chemotherapy to minimise the incidence of false-positive scans. Serial scanning may be required to fully evaluate areas of residual post-treatment PET tracer uptake, with many patients manifesting gradual resolution. [43]
The NCCN notes that PET/CT scan is essential posttreatment. Biopsy of a PET/CT scan–positive mass is recommended if additional systemic treatment is being considered [21]
Treatment of relapsed/refractory PMBCL
For treatment of relapse/refractory disease, NCCN guidelines recommends administering pembrolizumab or nivolumab ± brentuximab vedotin or following the guidelines for DLBCL. [21]
ESMO recommends salvage treatment strategies similar to nodal DLBCLs. If radiation has not been a component of initial therapy, RT should be incorporated into the salvage treatment for patients with relapsed disease, ideally post-transplant if significant mediastinal or lung volumes are involved. [43]
-
Example of mediastinal lymphoma at diagnosis. A large tumor mass is present in the anterior mediastinum, and an associated pleural effusion can also be seen.
-
Isolated CNS relapse of primary mediastinal B-cell lymphoma.
Tables

What would you like to print?
- Non-Hodgkin Lymphoma (NHL)
- Thoracic Non-Hodgkin Lymphoma Imaging
- Follicular Lymphoma (Non-Hodgkin Lymphoma) Staging
- Follicular Lymphoma (Non-Hodgkin Lymphoma) Treatment Protocols
- Diffuse Large B-Cell Lymphoma (Non-Hodgkin Lymphoma) Staging
- Diffuse Large B-Cell Lymphoma (Non-Hodgkin Lymphoma) Treatment Protocols
- New Drug Combo Boosts PFS in Hodgkin Lymphoma
- Doxorubicin Increases Breast Cancer Risk in Women With Hodgkin Lymphoma
- Expanded Indications for Hodgkin and CLL Drugs in Europe
-
 Key Data in Non-Hodgkin Lymphoma From EHA 2023
Key Data in Non-Hodgkin Lymphoma From EHA 2023
-
Non-Hodgkin Lymphoma Highlights From SOHO 2023
-
Don't Miss the Dx: A 61-Year-Old Man With Left Flank Pain, Fever, Night Sweats, and Malaise



 Brain Lesions: Summaries of 12 Cases
Brain Lesions: Summaries of 12 Cases