Practice Essentials
Myocarditis is an inflammatory disease of the myocardium with a wide range of clinical presentations, from subtle to devastating.
The image below depicts numerous lymphocytes with associated myocyte damage.
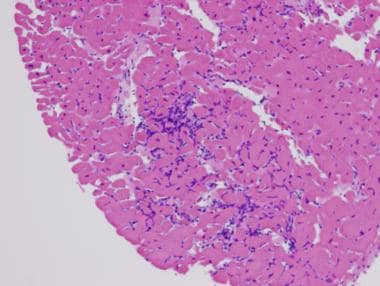 Myocarditis. Hematoxylin and eosin staining. Low power. This image shows numerous lymphocytes with associated myocyte damage. Photo courtesy of Dr Donald Weilbaecher.
Myocarditis. Hematoxylin and eosin staining. Low power. This image shows numerous lymphocytes with associated myocyte damage. Photo courtesy of Dr Donald Weilbaecher.
Signs and symptoms
Myocarditis usually manifests in an otherwise healthy person and can result in rapidly progressive heart failure and arrhythmia. Patients with myocarditis have a clinical history of acute decompensation of heart failure, but they have no other underlying cardiac dysfunction or have low cardiac risk.
Patients with myocarditis may present with the following signs and symptoms:
-
Mild symptoms of chest pain (in concurrent pericarditis), fever, sweats, chills, dyspnea
-
In viral myocarditis: Recent history (≤1-2 wk) of flulike symptoms of fevers, arthralgias, and malaise or pharyngitis, tonsillitis, or upper respiratory tract infection
-
Palpitations, syncope, or sudden cardiac death due to underlying ventricular arrhythmias or atrioventricular block (especially in giant cell myocarditis)
-
Heart failure
See Clinical Presentation for more detail.
Diagnosis
The diagnosis of acute myocarditis is usually presumptive, based on patient demographics and the clinical course. Because many cases of myocarditis are not clinically obvious, a high degree of suspicion is required.
Patients with myocarditis usually present with signs and symptoms of acute decompensation of heart failure (eg, tachycardia, gallop, mitral regurgitation, edema) and, in those with concomitant pericarditis, with pericardial friction rub.
Specific findings in special cases are as follows:
-
Sarcoid myocarditis: Lymphadenopathy, also with arrhythmias, sarcoid involvement in other organs (up to 70%)
-
Acute rheumatic fever: Usually affects heart in 50-90%; associated signs, such as erythema marginatum, polyarthralgia, chorea, subcutaneous nodules (Jones criteria)
-
Hypersensitive/eosinophilic myocarditis: Pruritic maculopapular rash and history of using offending drug
-
Giant cell myocarditis: Sustained ventricular tachycardia in rapidly progressive heart failure [1]
-
Peripartum cardiomyopathy: Heart failure developing in the last month of pregnancy or within 5 months following delivery
Testing
Laboratory studies use to evaluate suspected myocarditis may include the following:
-
Complete blood count
-
Erythrocyte sedimentation rate level (and that of other acute phase reactants [eg, C-reactive protein])
-
Rheumatologic screening
-
Cardiac enzyme levels (eg, creatine kinase or cardiac troponins)
-
Serum viral antibody titers
-
Viral genome testing in endomyocardial biopsy
-
Electrocardiography
Imaging studies
The following imaging studies may be used to assess patients with suspected myocarditis:
-
Echocardiography: To exclude other causes of heart failure (eg, amyloidosis or valvular or congenital causes) and to evaluate the degree of cardiac dysfunction
-
Antimyosin scintigraphy: To identify myocardial inflammation
-
Coronary angiography: To rule out coronary ischemia as cause of new-onset heart failure
-
Gadolinium-enhanced magnetic resonance imaging: To assess extent of inflammation and cellular edema; nonspecific
Procedures
Endomyocardial biopsy is the standard tool for diagnosing myocarditis. However, the use of routine endomyocardial biopsy in establishing the diagnosis of myocarditis rarely is helpful clinically, since histologic diagnosis seldom has an impact on therapeutic strategies, unless giant cell myocarditis is suspected. [2, 3]
The Heart Failure Society of America 2010 comprehensive heart failure practice guideline recommends considering endomyocardial biopsy for patients with acute deterioration of heart function of unknown origin that is not responding to medical treatment. [4]
See Workup for more detail.
Management
In general, treatment of either acute or chronic myocarditis is aimed at reducing congestion and improving cardiac hemodynamics in heart failure, as well as providing supportive therapy, with the hope of prolonging survival. Treatment of heart failure follows the same treatment regimen regardless of the underlying cause (ie, inhibitors, beta-adrenergic blockers).
Pharmacotherapy
Medications used in the management of myocarditis include the following:
-
Vasodilators (eg, nitroglycerin, sodium nitroprusside)
-
Angiotensin-converting enzyme inhibitors (eg, enalapril)
-
Diuretics (eg, furosemide)
Anticoagulation when there is definite indication such as atrial fibrillation or intracardiac thrombus.
Antiarrhythmics can be used cautiously, although most antiarrhythmic drugs have negative inotropic effects that may aggravate heart failure. (Supraventricular arrhythmias should be converted electrically.) High-grade ventricular ectopy and ventricular tachyarrhythmia should be treated cautiously with beta blockers and antiarrhythmics.
Inotropic drugs (eg, dobutamine, milrinone) may be necessary for severe decompensation, although they are highly arrhythmogenic. Long-term treatment follows the same medical regimen, including angiotensin-converting enzyme inhibitors, beta blockers, and aldosterone receptor antagonists. However, in some instances, some of these drugs cannot be implemented initially because of hemodynamic instability.
Nonpharmacotherapy
Supportive care in patients with myocarditis includes the following:
-
Hemodynamic and cardiac monitoring
-
Administration of supplemental oxygen
-
Fluid management
Surgical option
Surgical intervention in myocarditis may include the following:
-
Temporary transvenous pacing for complete heart block
-
Cardiac transplantation
-
Extreme cases: Ventricular assist device or percutaneous circulatory support; left ventricular assistive devices (LVADs) and extracorporeal membrane oxygenation [5]
See Treatment and Medication for more detail.
Background
Myocarditis is an inflammatory disease of the myocardium with a wide range of clinical presentations, from subtle to devastating. More specifically, it is described as "an inflammatory infiltrate of the myocardium with necrosis and/or degeneration of adjacent myocytes" [6] and it can be characterized on the basis of etiology, phase, severity, predominant symptoms, and pathological features. [7]
Myocarditis usually manifests in an otherwise healthy person and can result in rapidly progressive (and fatal) heart failure and arrhythmia. [8, 9] In the clinical setting, myocarditis is synonymous with inflammatory cardiomyopathy. It is diagnosed by established histologic, immunologic, and immunochemical criteria; however, electrocardiographic and imaging studies can aid in diagnosis. (See Etiology, Presentation, and Workup.)
Lieberman further classified myocarditis as follows [10] :
-
Fulminant myocarditis: Follows a viral prodrome; distinct onset of illness consisting of severe cardiovascular compromise with ventricular dysfunction and multiple foci of active myocarditis; either resolves spontaneously or results in death
-
Acute myocarditis: Less distinct onset of illness, with established ventricular dysfunction; may progress to dilated cardiomyopathy
-
Chronic active myocarditis: Less distinct onset of illness, with clinical and histologic relapses; development of ventricular dysfunction associated with chronic inflammatory changes (including giant cells)
-
Chronic persistent myocarditis: Less distinct onset of illness; persistent histologic infiltrate with foci of myocyte necrosis but without ventricular dysfunction (despite symptoms, eg, chest pain, palpitations)
These terms are still used to describe the clinical presentation and progression of myocarditis, particularly in the absence of ongoing histologic evaluation. (See Etiology and Presentation.)
Patient education
Patients should be advised of the current understanding of the natural history of myocarditis and the strengths and limitations of different diagnostic testing and therapeutic options. (See Etiology, Presentation, Workup, Treatment, and Medication.)
Etiology
Myocarditis is probably caused by a wide variety of infectious organisms, autoimmune disorders, and exogenous agents, with genetic and environmental predisposition. [7] There remains debate about the specific mechanisms that govern "the transition from the initial trigger to myocardial inflammation and from acute myocardial damage to chronic ventricular dysfunction." [7] Most cases are presumed to be caused by a common pathway of host-mediated, autoimmune-mediated injury, although direct cytotoxic effects of the causative agent and damages due to cytokine expression in the myocardium may play some role in myocarditis etiology. Damage occurs through the following mechanisms:
-
Direct cytotoxic effect of the causative agent
-
Secondary immune response, which can be triggered by the causative agent
-
Cytokine expression in the myocardium (eg, tumor necrosis factor [TNF] ̶ alpha, nitric oxide synthase)
-
Aberrant induction of apoptosis [11]
In myocarditis related to coronavirus disease 2019 (COVID-19), cardiac inflammation is generally due to direct cardiac invasion with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) or a result of the intense cytokine storm that often arises during the course of the disease. [12]
Myocardial damage has two main phases, as follows:
-
Acute phase (first 2 wk): Myocyte destruction is a direct consequence of the offending agent, which causes cell-mediated cytotoxicity and cytokine release, contributing to myocardial damage and dysfunction; detection of the causal agent is uncommon during this stage
-
Chronic phase (>2 wk): Continuing myocyte destruction is autoimmune in nature, with associated abnormal expression of human leukocyte antigen (HLA) in myocytes (and in the case of viral myocarditis, persistence of the viral genome in myocardium)
Viral myocarditis
In viral myocarditis, viral isolates differ in tissue tropism and virulence. For example, coxsackievirus A9 is a self-limiting myocarditis, whereas coxsackievirus B3 causes severe myocarditis resulting in a high mortality rate. The induction of the coxsackie-adenovirus receptor (CAR) and the complement deflecting protein decay accelerating factor (DAF, CD55) may allow efficient internationalization of the viral genome.
Viral replication may lead to further disruption of metabolism and to perturbation of inflammation and its response. Vasospasm induced by endothelial cell viral infection may also contribute to further damage. [13]
New evidence of dystrophin disruption by expression of enteroviral protease 2A points to yet another unique pathogenic mechanism. [14] In contrast, some viruses (such as parvovirus B19) may focus on pericapillary depositions, contributing to diastolic dysfunction rather than to direct myocyte destruction. Regardless, viral persistence provides the necessary stimuli for autoimmune or other inflammatory responses.
Idiopathic myocarditis
Approximately 50% of the time, myocarditis is classified as idiopathic, although a report by Klugman et al found that 82% of the pediatric cases studied were considered idiopathic. [15] The investigators also determined that 3% of cases in the study had a known bacterial or viral etiology, and that 6% of cases were related to other diseases.
In idiopathic cases, a viral etiology is often suspected but unproved, even with sophisticated immunohistochemical and genomic studies. Studies on patients with idiopathic dilated cardiomyopathy found evidence of viral particles in endomyocardial biopsy specimens in up to two thirds of the patients. [16]
Causes
Causes of myocarditis include the following:
-
Viral: Enterovirus, [11] coxsackie B, adenovirus, influenza, cytomegalovirus, poliomyelitis, Epstein-Barr virus, HIV-1, viral hepatitis, mumps, rubeola, varicella, variola/vaccinia, arbovirus, respiratory syncytial virus, herpes simplex virus, yellow fever virus, rabies, parvovirus
-
Rickettsial: Scrub typhus, Rocky Mountain spotted fever, Q fever
-
Bacterial: Diphtheria, tuberculosis, streptococci, meningococci, brucellosis, clostridia, staphylococci, melioidosis, Mycoplasma pneumoniae, psittacosis
-
Spirochetal: Syphilis, leptospirosis/Weil disease, relapsing fever/Borrelia, Lyme disease
-
Fungal: Candidiasis, aspergillosis, cryptococcosis, histoplasmosis, actinomycosis, blastomycosis, coccidioidomycosis, mucormycosis
-
Protozoal: Chagas disease, toxoplasmosis, trypanosomiasis, malaria, leishmaniasis, balantidiasis, sarcosporidiosis
-
Helminthic: Trichinosis, echinococcosis, schistosomiasis, heterophyiasis, cysticercosis, visceral larva migrans, filariasis
-
Bites/stings: Scorpion venom, snake venom, black widow spider venom, wasp venom, tick paralysis
-
Drugs (usually causing hypersensitivity myocarditis)
-
Chemotherapeutic drugs: Doxorubicin and anthracyclines, streptomycin, cyclophosphamide, interleukin-2, anti-HER-2 receptor antibody/Herceptin
-
Antibiotics: Penicillin, chloramphenicol, sulfonamides
-
Antihypertensive drugs: Methyldopa, spironolactone
-
Antiseizure drugs: Phenytoin, carbamazepine
-
Amphetamines, cocaine, catecholamines
-
Chemicals: Hydrocarbons, carbon monoxide, arsenic, lead, phosphorus, mercury, cobalt
-
Physical agents (radiation, heatstroke, hypothermia)
-
Acute rheumatic fever
-
Systemic inflammatory disease: Giant cell myocarditis, sarcoidosis, Kawasaki disease, Crohn disease, systemic lupus erythematosus, ulcerative colitis, Wegener granulomatosis, thyrotoxicosis, scleroderma, rheumatoid arthritis
-
Peripartum cardiomyopathy
-
Posttransplant cellular rejection
Epidemiology
Occurrence in the United States
The frequency of myocarditis is difficult to ascertain, owing to the wide variation of clinical presentation. Incidence is usually estimated at 1-10 cases per 100,000 persons. Incidence of positive right ventricular biopsy findings in patients with suspected myocarditis is highly variable (ranging from 0-80%). According to estimates, as many as 1-5% of patients with acute viral infections may have involvement of the myocardium.
International occurrence
A population study in Finland found that, in a study of more than 670,000 healthy young male military recruits, 98 cases had myocarditis mimicking myocardial ischemia, 1 case presented as sudden death, and 9 cases presented as recent-onset dilated cardiomyopathy. [17, 18]
A Japanese 20-year series of 377,841 autopsies found idiopathic, nonspecific, interstitial, or viral myocarditis in only 0.11% of individuals. [19]
Race-, sex-, and age-related demographics
No particular race predilection is noted for myocarditis except for peripartum cardiomyopathy (a specific form of myocarditis that appears to have a higher incidence in patients of African descent).
The incidence of myocarditis is similar between males and females, although young males are particularly susceptible.
Patients are usually fairly young. The median age of patients affected with lymphocytic myocarditis is 42 years. Patients with giant cell myocarditis may be older (mean age 58 years), but this condition usually does not discriminate with respect to age, sex, or presenting symptoms.
Other susceptible groups include immunocompromised individuals, pregnant women, and children (particularly neonates).
Prognosis
Patients with fulminant myocarditis have a high mortality risk when the condition is not recognized and treated early; death occurs from cardiogenic shock, fatal ventricular tachyarrhythmias, or bradycardia. [20] Prompt recognition and initiation of circulatory support and maintenance of end-organ function are key to a favorable outcome. [20] Those who survive fulminant myocarditis have a good prognosis. In a study of 147 cases of myocarditis monitored for an average of 5.6 years, 93% of the 15 patients with fulminant disease were alive without transplant 11 years after biopsy, compared with 45% of the 132 patients with less severe disease. Left ventricular dilation was not as severe in the fulminant cases as in the nonfulminant ones. [21, 22]
Expression of soluble Fas and Fas ligands at initial presentation appears to be a good serologic marker to predict the prognosis of acute myocarditis, while antimyosin autoantibodies are associated with development of worse cardiac dysfunction in chronic myocarditis. [23]
Predictors of death or need for heart transplantation after acute myocarditis in multivariate analyses include syncope, low ejection fraction, and left bundle-branch block, all indicators of advanced cardiomyopathy. [24]
Morbidity and mortality
Most patients with mild symptoms recover completely without any residual cardiac dysfunction, although a third subsequently developing dilated cardiomyopathy. [18, 25, 26, 27] Eosinophilic myocarditis, left undiagnosed, can result in progressive, irreversible, and fatal myocardial damage. [28] Cardiogenic shock may occur in fulminant cases of myocarditis.
In the Myocarditis Treatment Trial, the 1-year mortality rate was 20% and the 4-year mortality rate was 56% in a population with symptomatic heart failure presentation and left ventricular ejection fraction lower than 45% at baseline. [29] Severe heart block requiring permanent pacemaker placement occurred in 1% of patients in the trial.
In a study of patients with giant cell myocarditis, 89% of patients either died or underwent transplantation, with median survival from symptom onset to death or transplantation being only 5.5 months. [30]
A study by Klugman et al reported a 92% survival rate among 216 pediatric patients with myocarditis. [15] According to the investigators, nonsurviving patients were characterized by a greater severity of illness at presentation and a frequent need for extracorporeal membrane oxygenation and other intensive care unit therapies. With regard to postpartum cardiomyopathy, the mortality rate at 1 year can be as high as 50%.
-
Myocarditis. Hematoxylin and eosin staining. Low power. This image shows numerous lymphocytes with associated myocyte damage. Photo courtesy of Dr Donald Weilbaecher.
-
Myocarditis. Hematoxylin and eosin staining. High power. Toxoplasmosis (numerous purple granular-like structures within a myocyte) is demonstrated.
-
Myocarditis. Hematoxylin and eosin staining. High power. Lymphocytes, histiocytes, and a multinucleated giant cell representing sarcoidosis (a diagnosis of exclusion) is shown.
