Practice Essentials
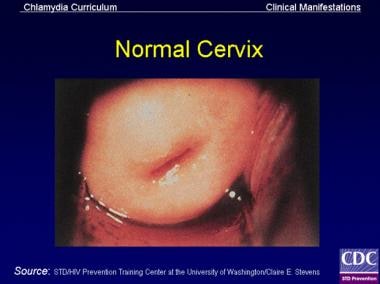
Cervicitis is an inflammation of the uterine cervix, characteristically diagnosed by: (1) a visible, purulent or mucopurulent endocervical exudate in the endocervical canal or on an endocervical swab specimen and/or (2) sustained, easily induced endocervical bleeding when a cotton swab is gently passed through the cervical os. [1, 2] A normal cervix is pictured below. (See Presentation.)
Noninfectious cervicitis
Noninfectious cervicitis can be caused by the following:
-
Local trauma - eg, cervical irritation caused by tampons, a cervical cap, the string from an intrauterine contraceptive device, a pessary, or a diaphragm
-
Radiation
-
Chemical irritation - eg, vaginal douches, latex exposure, or contraceptive creams
-
Systemic inflammation - eg, Behçet syndrome
-
Malignancy
Infectious cervicitis
The infectious etiologies of cervicitis, all of which are sexually transmitted infections (STIs), are significantly more common than the noninfectious causes. This article focuses on the infectious etiologies of cervicitis. (See Etiology.)
Infectious cervicitis may be caused by Chlamydia trachomatis (see the first image below), Neisseria gonorrhoeae , or herpes simplex virus (HSV) (see the second image below). In most cases of cervicitis, however, lab tests fail to isolate an organism; this is particularly true in women with low risk factors. (See Etiology and Workup.) [1]
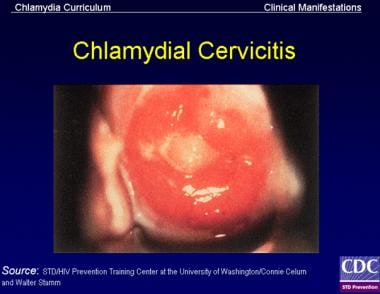 Signs of chlamydial cervicitis on speculum examination may include mucopurulent endocervical discharge and spontaneous or easily induced endocervical bleeding or any zones of ectopy.
Signs of chlamydial cervicitis on speculum examination may include mucopurulent endocervical discharge and spontaneous or easily induced endocervical bleeding or any zones of ectopy.
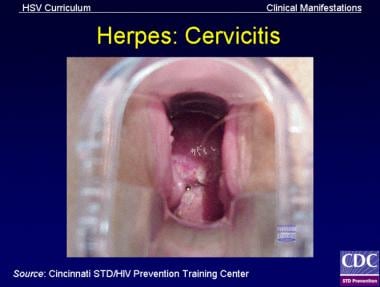 Herpes simplex virus (HSV) cervicitis may involve the exocervix or endocervix, and it may be symptomatic or asymptomatic. Usually, the cervix appears abnormal to inspection, with diffuse vesicular lesions, ulcerative lesions, erythema, or friability.
Herpes simplex virus (HSV) cervicitis may involve the exocervix or endocervix, and it may be symptomatic or asymptomatic. Usually, the cervix appears abnormal to inspection, with diffuse vesicular lesions, ulcerative lesions, erythema, or friability.
Trichomonas vaginalis, which, technically, causes vaginal infections, is commonly included in the discussion of cervicitis.
Because the female genital tract is contiguous from the vulva to the fallopian tubes, there is some overlap between vulvovaginitis and cervicitis; both conditions are commonly categorized as lower genital tract infections. Infections involving the endometrium and fallopian tubes are commonly categorized as upper genital tract infections and are not discussed in this article. (See DDx.)
Etiology
The most common etiologies of cervicitis are infectious, with sexual transmission of organisms such as with C trachomatis and N gonorrhoeae being the primary means by which it is spread. [1] Other etiologic organisms include Trichomonas vaginalis and herpes simplex virus (HSV), especially primary type 2 HSV. [1]
Noninfectious causes of cervicitis include local trauma, radiation, chemical irritation, systemic inflammation, and malignancy. Limited data exist to suggest frequent douching, as well as Mycoplasma genitalium infection and bacterial vaginosis, as potential causes. [1]
Risk factors
Risk factors for cervicitis include the following:
-
Multiple sex partners
-
Young age
-
Single marital status
-
Urban residence
-
Low socioeconomic status
-
Alcohol or drug use
Genetic predisposition, largely due to a variable host immune response, also plays an important role in the variability in infectious complications. [3] Variants in the genes that regulate toll-like receptors (TLRs), an important component in the innate immune system, have been associated with an increased progression of C trachomatis infection to pelvic inflammatory disease (PID). [4]
M genitalium
Although the role of M genitalium in PID is unclear, a study of 2378 British female students reported that this organism does not appear to be a significant etiologic agent for PID in this population (the incidence of PID was 3.9% over 12 mo in women with M genitalium infection vs 1.7% in noninfected women). [5]
In a later study, however—a Swedish report on 5519 women at an outpatient gynecologic service—it was noted that M genitalium was a strong independent risk factor for PID and cervicitis, although there was a lower frequency of both conditions relative to women with C trachomatis infection. [6] Further investigation is needed to determine the role of M genitalium in PID, infertility, and cervicitis. [7]
A study by Dehon et al found a high prevalence of M genitalium (7.4%) among the HIV-infected women and also found that chronic M genitalium infection was associated with increased secretion of proinflammatory cytokines and marked inflammatory cervical infiltrates in the cervix with enrichment of HIV target cells. The study concluded that not only was M genitalium implicated as an etiologic agent of cervicitis in HIV-infected women but that it also provided a potential mechanism for enhanced HIV transmission to an uninfected partner. [8]
Epidemiology
Occurrence in the United States
The Centers for Disease Control and Prevention (CDC) estimates that over 19 million new sexually transmitted infections (STIs) occur annually, almost half of them among persons aged 15-24 years. [9] In addition to potentially severe health consequences, STIs pose a tremendous economic burden, with direct medical costs as high as $17 billion in a single year. [9]
Trichomonas is the most common curable STI. Although an estimated 3.7 million people are infected (2.3 million in women ages 14-49 y), about 70% of these individuals are asymptomatic. [10] About 7.4 million new cases occur each year in women and men. [11]
Chlamydia, however, is the most frequently reported infectious disease in the US, with the majority of cases occurring in individuals aged 25 years or younger. [12] The reported incidence of chlamydial infections has steadily increased over the past 2 decades, with 1.3 million cases reported in 2010. [9] Although this increased incidence may reflect changes in screening efforts, many cases are not reported or are undiagnosed. More than 50% of sexually active young women are not screened annually, despite CDC recommendations. [9]
Gonorrhea is the second most commonly reported infectious disease in the United States, with more than 300,000 cases reported in 2010. [9] Annually, approximately 700,000 new gonococcal infections occur. [13] Much like chlamydia, gonorrhea is believed to be underreported. In a study of 1469 emergency department patients diagnosed with cervicitis, Burnett et al found that 1.8% and 9.3% of patients with cervicitis were also positive for gonorrhea or chlamydia, respectively. [14] Of a separate group of 343 patients with pelvic inflammatory disease (PID), 4.4% and 10% were positive for gonorrhea or chlamydia, respectively. [14]
The annual rates of infection by herpes simplex virus (HSV) is difficult to estimate, because the vast majority of initial infections are asymptomatic or unrecognized. In addition, HSV infections are not required to be reported in the US. [9]
The prevalence of HSV type 2 is about 16% (primarily among Black women: 48%). [15]
International occurrence
Worldwide, 448 million adults (aged 15-49 years) become infected with a curable STI (trichomoniasis, chlamydia, syphilis, or gonorrhea) every year. [16] Other STIs are caused by various bacterial (chancroid, donovanosis) and viral (eg, human immunodeficiency virus [HIV], hepatitis B virus [HBV], cytomegalovirus [CMV]) pathogens, as well as by parasites (vaginal trichomoniasis, vulvovaginitis, balanoposthitis [men]). [16]
Human papillomavirus
The prevalence of HPV, a cause of cervical cancer, varies roughly 20-fold internationally. In various studies, the seroprevalence of HSV-2 is higher in the United States (13-40%) than in Europe (7-16%) and is highest in Africa (30-40%).
Among the countries evaluated in a worldwide analysis, Spain had the lowest prevalence of HPV; only 1.4% of women in Spain tested positive for HPV. [17] The highest prevalence of HPV was seen in sub-Saharan Africa; 26% of women in Nigeria tested positive for the virus. South America tended to have rates that were between those of Europe and sub-Saharan Africa, whereas rates in Asia varied widely (with the lowest rates in Hanoi, Vietnam, and the highest in India and Korea). [17]
M genitalium
M genitalium infections have been implicated in cervicitis, PID, and female infertility. [6, 7] A review of more than 27,000 women from 48 published reports found an overall global prevalence of 7.3% M genitalium urogenital infection in high-risk populations and 2.0% in low-risk populations. [7] The investigators reported the prevalence of this agent in the general population as between that of C trachomatis and N gonorrhoeae. Furthermore, in 7 of 14 studies of lower tract inflammation, there was a positive association between M genitalium with urethritis, vaginal discharge, and microscopic evidence of cervicitis and/or mucopurulent discharge. [7]
Race-, sex-, and age-related differences
No race predilection exists for cervicitis. Known risk factors include urban residence and low socioeconomic status.
Cervicitis can only be present in females. Male urethritis is more often symptomatic; therefore, diagnosis is usually made earlier in males than in females. Females with cervicitis are most often asymptomatic, so they do not seek evaluation or treatment as readily. Risk factors for cervicitis include age younger than 25 years, single marital status, and a new sexual partner within the past 6 weeks. Biologic (eg, postulated immaturity of the female reproductive tract) and behavioral factors (eg, greater number of partners, low awareness of acquired immunodeficiency syndrome [AIDS] and other STIs, and limited use of protection against STIs) are thought to contribute to this risk. Routine screening of sexually active adolescents and young adults is therefore recommended.
Routine chlamydia screening of sexually active women younger than 25 years is recommended by the US Preventive Services Task Force (USPSTF), American Cancer Society (ACS), American College of Obstetricians and Gynecologists (ACOG), American Society for Colposcopy and Cervical Pathology (ASCCP), and American Society for Clinical Pathology (ASCP) to prevent the consequences of untreated chlamydial infection (eg, PID, infertility, ectopic pregnancy, chronic pelvic pain). [18, 19, 20] Fewer than half of young, sexually active females in the United States are screened for chlamydia. [9]
Prognosis
Gonorrhea, chlamydia, and trichomoniasis infections can be cured with antibiotic therapy, whereas antiviral therapy can reduce the number of herpes simplex virus (HSV) outbreaks, the duration of symptoms, and the severity of symptoms.
Complications from untreated infectious cervicitis depend on the pathogen. Untreated gonorrhea and chlamydia infections can lead pelvic inflammatory disease (PID), which can then result in infertility, chronic pelvic pain, and ectopic pregnancy. Other morbidity may include spontaneous abortion, premature rupture of membranes, and preterm delivery if infection is present during pregnancy.
Certain subtypes of HPV are linked with the development of cervical cancer. Untreated active HSV infections in the perinatal and neonatal period can cause intellectual disability, blindness, low birth weight, stillbirth, meningitis, and death.
Patient Education
Patients must understand that cervicitis is a preventable, sexually transmitted infection (STI) and that the most effective way to prevent the transmission of the infective agents that cause the disease is to avoid sexual intercourse with infected partners.
Ideally, both partners should be tested for common STIs, including human immunodeficiency virus, before initiating a sexual relationship. If the risk of infection is unknown by testing, then a condom should be used for all sexual acts. Condoms are available for men and women and have been proven to decrease the transmission of many STIs, including HIV, when used appropriately and consistently.
To avoid reinfection following cure, infected women must ensure that all of their sexual partners are treated for STIs.
For patient education resources, see the Women's Health Center and the Pregnancy Center, as well as Cervicitis, Pelvic Inflammatory Disease, Ectopic Pregnancy, Female Sexual Problems, and Pap Smear.
-
Normal cervix
-
Cervix of a lactating woman without sexually transmitted infections. The patient had twice given birth vaginally.
-
Cervical cellularity (ectopy), which is often present in adolescents, allows for greater adherence of infectious organisms in the cervix. The risk of acquiring acute salpingitis for a sexually active 15-year-old is 1:8, compared with 1:80 for women aged 24 years and older.
-
Signs of chlamydial cervicitis on speculum examination may include mucopurulent endocervical discharge and spontaneous or easily induced endocervical bleeding or any zones of ectopy.
-
In women with gonococcal cervicitis, the cervix may show mucopurulent or purulent cervical discharge and easily induced cervical bleeding.
-
Herpes simplex virus (HSV) cervicitis may involve the exocervix or endocervix, and it may be symptomatic or asymptomatic. Usually, the cervix appears abnormal to inspection, with diffuse vesicular lesions, ulcerative lesions, erythema, or friability.
-
T vaginalis can have a characteristic "frothy" gray or yellow-green vaginal discharge and pruritus. The occurrence of cervical petechiae, or "strawberry cervix," is a classic presentation that is seen in less than 2% of cases. T vaginalis may also infect the Skene glands and the urethra and may be asymptomatic in women.
-
Papanicolaou (Pap) stain, high power, showing the Herpes simplex virus (HSV) infecting cells with multiple nuclei, intranuclear inclusions, and margination of the chromatin to the outer portion of the nuclei.
-
Pap stain, high power, showing human papillomavirus (HPV) infecting a cell with a dark, wrinkled nucleus surrounded by a clear cytoplasmic halo.
-
Pap stain, high power (under oil immersion), showing 2 pear-shaped structures representing Trichomonas. Small, pale nuclei and cytoplasmic granules are present.
