Overview
Emphysematous cholecystitis, also known as acute gaseous cholecystitis or clostridial cholecystitis, is generally considered a surgical emergency, comprising an acute infection of the gallbladder wall caused by gas-forming organisms (eg, Clostridium, Escherichia coli). [1] An infrequent, insidious, and rapidly progressive form of acute cholecystitis, emphysematous cholecystitis can be even more deadly. In general, only 1-4% of cases of acute cholecystitis will progress to emphysematous cholecystitis, which is then associated with higher rates of gangrene, perforation, and a mortality of up to 20%. [2, 3]
An estimated 500,000 cholecystectomies are performed per year in the United States. [4] Assuming all patients with emphysematous cholecystitis undergo surgery, this would indicate that at least 5,000 cholecystectomies are performed per year for emphysematous cholecystitis. Although the number of patients who are treated successfully without surgery is small, the number of patients who die without surgery is unknown. The literature suggests that percutaneous cholecystostomy may serve as an alternate treatment for high-risk surgical candidates. [5, 6]
The diagnosis is often made by the radiographic presence of air within the gallbladder wall or lumen (see the image below). Elderly males, especially those with diabetes, are particularly susceptible to emphysematous cholecystitis. The computed tomography (CT) scan below shows an affected patient.
 Emphysematous Cholecystitis. Emphysematous cholecystitis in a 47-year-old man with diabetes who experienced abdominal pain. This computerized tomography scan shows gas within the wall of the gallbladder (horizontal arrow) as well as within the lumen of the gallbladder (vertical arrow). Courtesy of Helen Morehouse, MD.
Emphysematous Cholecystitis. Emphysematous cholecystitis in a 47-year-old man with diabetes who experienced abdominal pain. This computerized tomography scan shows gas within the wall of the gallbladder (horizontal arrow) as well as within the lumen of the gallbladder (vertical arrow). Courtesy of Helen Morehouse, MD.
See Can't-Miss Gastrointestinal Diagnoses, a Critical Images slideshow, to help diagnose the potentially life-threatening conditions that present with gastrointestinal symptoms.
For more information, see Acute Cholecystitis.
Etiology and Pathophysiology
Four pathogenetic factors are proposed in the development of emphysematous cholecystitis.
Vascular compromise of the gallbladder
The cystic artery is often the sole arterial supply of the gallbladder. Occlusion or stenosis results in compromised viability of the gallbladder, in which arteriosclerosis is the usual causative abnormality, although the condition has also been described after an embolic event. Vascular compromise of the cystic artery renders the gallbladder ischemic and facilitates the proliferation of gas-forming organisms and bacterial translocation in the devitalized tissue with low oxygen saturation. [7] Bactericidal bile is rendered alkaline, facilitating further bacterial growth. Histopathologic reviews of emphysematous gallbladders reveal a higher incidence of endarteritis obliterans compared with the typical acute cholecystitis secondary to cholelithiasis. [8]
A case of emphysematous cholecystitis that developed following hepatic artery embolization appeared to substantiate the theory that vascular compromise is a main pathogenic factor. [9] In another report, gallbladder torsion progressed to emphysematous cholecystitis, probably due to ischemic necrosis (secondary to torsion) facilitating infection and translocation of gas-forming bacteria. [10]
Emphysematous cholecystitis has also been reported as an adverse event caused by sunitinib, administered for the treatment of gastrointestinal stromal tumor (GIST), probably due to the thromboembolic side effect of this class of drugs (vascular endothelial growth factor [VEGF] receptor inhibitors). [11]
Cholelithiasis
Gallstones are observed in 40-80% of patients with emphysematous cholecystitis. [5, 12] Impaction of stones in the cystic duct can lead to localized edema of the gallbladder wall, which contributes to the vascular compromise of the gallbladder. Nevertheless, emphysematous cholecystitis in the presence of acalculous cholecystitis is well established, occurring frequently in the emphysematous form, suggesting that there is a difference in the pathogenesis between emphysematous cholecystitis and acute calculous cholecystitis. [13] Indeed, the proportion of patients with acalculous cholecystitis in association with emphysematous cholecystitis exceeds that of patients with ordinary acute calculous cholecystitis, suggesting that gallstones may not be central to its underlying pathogenesis. [13, 14]
Impaired immune protection
The majority of patients with emphysematous cholecystitis have diabetics between the ages of 50 and 70 years. [3] In cases of hyperglycemia, as often seen in diabetes, macrophage migration is impaired and often decreases a body's ability to combat pathogenic infections. Both metabolic abnormalities and older age likely contribute to the increased risk of infection.
Infection with gas-forming organisms
Commonly isolated microorganisms are clostridial species, E coli, and Klebsiella species. Less frequently, Enterococci and anaerobic Streptococci are among the other organisms detected. Although the intramural gas observed in patients with emphysematous cholecystitis seems to result from gas-forming bacteria, whether these bacteria represent the primary cause of the disorder or are secondary invaders remains unclear. Concomitant emphysematous cholecystitis and emphysematous pyelonephritis raise the possibility of septic seeding of the gallbladder wall. Infectious complications following endoscopic retrograde cholangiopancreatography (ERCP) have also been reported. [15, 16]
In an analysis of bile in 109 cases of emphysematous cholecystitis, 95 of 109 (87%) had a positive culture, of which 46% were clostridial species (79% of the clostridial cultures grew Clostridium welchii) and 33% grew E coli, often as a copathogen with clostridia. [13]
In a separate series of 20 patients with emphysematous cholecystitis, Garcia-Sancho Tellez et al reported gallbladder culture results in which E coli grew in 40%, Bacteroides fragilis in 30%, and C perfringens in 20%. [17]
The bacteriologic patterns of simple (ie, nonemphysematous) acute cholecystitis are vastly different—only 12% of the positive bile cultures grew clostridia. [13] Thus, there is nearly a 4-fold difference in the incidence of clostridial infection in patients with emphysematous cholecystitis compared with those with acute cholecystitis. [13]
It is thought that these organisms acquire pathogenicity when they proliferate in a devascularized gallbladder. Specifically, Clostridium produces several different exotoxins, the most prevalent being oxygen-stable lecithinase-C, an alpha-toxin which is hemolytic, tissue necrotizing, and lethal. [18] This alpha-toxin induces profound shock via increased capillary permeability, cardiotoxicity, and leukocyte dysfunction.
Presentation
Despite the potentially lethal nature of this disease, patients with emphysematous cholecystitis have deceptively mild clinical findings that are frequently indistinguishable from acute cholecystitis. The insidious nature of this condition may mislead the clinician, and the patient may unsuspectingly rapidly deteriorate with sudden cardiovascular collapse and even death.
Symptoms
Initially, the most common clinical complaints are right upper quadrant pain and fever. The pain is localized to the right upper quadrant and often radiates to the back, but it is unrelated to position or physical activity. The patient may also complain of generalized abdominal pain consistent with peritonitis. Nausea and vomiting occur less frequently. [19]
In addition, a prior history of self-limited episodes of abdominal pain may be present. However, the clinician must be aware that elderly patients may develop acute intra-abdominal disorders with few or no localizing symptoms or signs. [7]
Physical findings
The physical examination usually reveals an elderly patient with fever and tachycardia who may be obtunded in the presence of septic shock. If concomitant choledocholithiasis or common duct obstruction and/or intrahepatic disease is present, these patients may be significantly jaundiced.
Evaluation of the abdomen generally reveals tenderness in the right upper quadrant, but there may also be diffuse tenderness consistent with peritonitis. In certain cases, there could be overlying erythema of the right side secondary to perforation of the gallbladder with intraperitoneal abscess. [20] In addition, an enlarged tense gallbladder may be noted, which is best demonstrated by light palpation. Bowel sounds are diminished or absent, especially in the presence of peritonitis. Transient relief of right upper quadrant pain followed by the appearance of peritoneal signs is the hallmark of perforation.
Major fluid sequestration (ie, "third-spacing" of fluid), florid septic shock, or peritonitis may occur as late clinical presentations.
Staging
Staging of the disease is image based (see Abdominal Ultrasonography). Diagnostic visualization on plain radiographs of the abdomen is thought to represent late-stage disease (see Abdominal Radiography). Computed tomography (CT) imaging differentiates preperforation disease from postperforation disease (see CT Scanning of the Abdomen). [14]
Diagnosis
Two levels of differential diagnosis for emphysematous cholecystitis should be considered: clinical and radiologic.
The clinical differential diagnosis is that of acute cholecystitis (nonemphysematous), both calculous and acalculous, as well as bacterial sepsis, peritonitis, and abdominal sepsis.
The radiologic differential diagnosis is that of finding gas in the biliary tree, which may be due to a biliary-enteric fistula (spontaneous or surgical); may occur after endoscopic retrograde cholangiopancreatography (ERCP), especially following a sphincterotomy; or may be due to cholangitis caused by gas-forming organisms. [21, 22] Imaging studies are key to the diagnosis of emphysematous cholecystitis.
Although urinalysis, chest radiography, and electrocardiography add little to establish a diagnosis, these studies should be obtained as part of the initial assessment of the patient, including laboratory work and radiographic imaging.
Laboratory Studies
Complete blood cell count with differential
Patients often have a leukocytosis that may be strikingly high, but this feature cannot differentiate emphysematous cholecystitis from acute cholecystitis.
Liver function tests
Liver tests results are usually normal or slightly elevated (eg, aspartate aminotransferase [AST], alanine aminotransferase [ALT]), reflecting the patient's febrile state and potentially reflecting concurrent choledocholithiasis. Significantly elevated liver function tests, especially elevated alkaline phosphatase (ALP), bilirubin, or gamma-glutamyl transpeptidase (GGTP), may suggest a common duct obstruction or intrahepatic disease.
Serum glucose
Serum glucose is often elevated, as many patients with emphysematous cholecystitis are also diabetic. Generally, hyperglycemia is associated with an increased risk of emphysematous cholecystitis due to its association with microvascular angiopathy. [23]
Abdominal Radiography
The key radiographic finding in emphysematous cholecystitis is air inside the gallbladder wall, gallbladder lumen (seen in 95% of patients), or in the biliary tree (15%). [17]
Abdominal radiographs may show the classic picture of a gallbladder wall containing gas (see the images below). The gallbladder is often fluid-filled, and gas that has leaked into its lumen collects in the least dependent portion. [24] Note that the absence of a gas-filled gallbladder wall on an abdominal radiograph does not exclude a diagnosis of emphysematous cholecystitis. [22, 25]
Inflammation and gas formation may extend to the pericholecystic tissues and extrahepatic ducts. This picture has been regarded as specific for emphysematous cholecystitis, but the sensitivity is unknown.
Pneumoperitoneum may be present, but this is rare. Occasionally, pneumobilia can be the sole radiographic finding. [13]
 Emphysematous Cholecystitis. Plain abdominal radiograph showing air in the gallbladder (arrow).
Emphysematous Cholecystitis. Plain abdominal radiograph showing air in the gallbladder (arrow).
 Emphysematous Cholecystitis. Emphysematous cholecystitis in a 61-year-old nondiabetic man with right upper quadrant abdominal pain, fever, and leukocytosis. This plain film shows the gallbladder with multiple stones. The wall of the fundus is delineated by intramural gas. Extramural gas also appears to be present in the soft tissues over the superior aspect of the gallbladder.
Emphysematous Cholecystitis. Emphysematous cholecystitis in a 61-year-old nondiabetic man with right upper quadrant abdominal pain, fever, and leukocytosis. This plain film shows the gallbladder with multiple stones. The wall of the fundus is delineated by intramural gas. Extramural gas also appears to be present in the soft tissues over the superior aspect of the gallbladder.
 Emphysematous Cholecystitis. Emphysematous cholecystitis in a 78-year-old man with diabetes with minimal abdominal distress. The plain film shows an enlarged gallbladder with multiple stones. The wall of the gallbladder is outlined by intramural gas.
Emphysematous Cholecystitis. Emphysematous cholecystitis in a 78-year-old man with diabetes with minimal abdominal distress. The plain film shows an enlarged gallbladder with multiple stones. The wall of the gallbladder is outlined by intramural gas.
With the advent of other imaging techniques, especially computed tomography (CT) scanning, the importance of plain radiographs of the abdomen has declined (see CT Scanning of the Abdomen). Changes noted on CT scans and ultrasonograms of the abdomen (see Abdominal Ultrasonography) can be observed before the classic abnormalities are visible on a plain abdominal radiograph. [14] Furthermore, the presence of abnormal findings on a plain film of the abdomen may indicate advanced disease, [14] as the classic picture observed on abdominal radiographs is believed to represent a late phase in the evolution of emphysematous cholecystitis and may predict poor outcomes.
Abdominal radiographs are less sensitive than ultrasonograms and CT scans, [26] and they may be unrevealing in up to 60% of cases. This consideration has altered both the diagnostic workup and the surgical options: early diagnosis requires CT scan imaging, and the presence or absence of gas outside the gallbladder will influence the choice of the surgical approach. [14]
Abdominal Ultrasonography
Ultrasonography is the most common imaging modality currently employed to visualize the gallbladder, especially in patients with the clinical suspicion of acute cholecystitis. This modality helps to detect acute emphysematous cholecystitis earlier than plain abdominal radiography and identifies the condition in 90-95% of cases.
Emphysematous cholecystitis is classically described ultrasonographically in three stages, as described below. [21]
Stage I
Gas is present in the gallbladder lumen. There is a dense band of hyperreflective echoes with distal reverberations when the gallbladder is full of gas, or a band of reverberations in the gas-filled portion of the gallbladder when the gallbladder is only partially full of gas.
Stage II
Gas is present in the gallbladder wall. There is an area of high reflectivity in the gallbladder wall with reverberations that may change position with patient movement, or a bright hyperreflective ring emanating from the entire gallbladder circumference.
Stage III
Gas is present in the pericholecystic tissue and inside the gallbladder wall and lumen—suggesting gangrene and perforation.
Effervescent gallbladder
In some cases, there may be multiple tiny echogenic foci in the gallbladder lumen, arising from the dependent part of the gallbladder and "floating" to the nondependent wall, reminiscent of bubbles rising in a glass of champagne. [27, 28, 29]
Ring-down effect/comet tail
Curvilinear gaseous artifacts in the gallbladder, the "ring-down effect" or "comet tail," are diagnostic of emphysematous cholecystitis, but the frequency with which these are observed is not clear. [28]
Disadvantages
One disadvantage of ultrasonography is that extensive gallbladder wall gas may be interpreted as nonvisualization of the gallbladder, resulting in a false-negative result. [14] In addition, the characteristic findings of intraluminal or intramural gas may be highly echogenic reflectors on ultrasonography, which can be mistaken for a porcelain gallbladder or stones adherent to the gallbladder wall. These findings are not diagnostic of emphysematous cholecystitis. The cognizant clinician should question the paradoxical absence (ie, ultrasonographic nonvisualization) of a gallbladder in the clinical setting of a patient who likely has gallbladder disease. [14]
Although ultrasonography is highly specific (90-95%) to diagnose acute emphysematous cholecystitis, its sensitivity is lower. Computed tomography (CT) scanning may help further consolidate the diagnosis in equivocal cases. However, if the diagnosis is made by ultrasonography, surgical intervention should be considered and CT imaging is unwarranted.
CT Scanning of the Abdomen
Evaluation with abdominal computed tomography (CT) scanning is now considered the primary imaging modality to confirm acute emphysematous cholecystitis, as it is the most sensitive and specific imaging modality for identifying gas in the gallbladder lumen or wall (see the images below). [30, 31, 32] CT scanning demonstrates emphysematous changes in the gallbladder wall that are diagnostic of this condition, and it is highly sensitive for tiny bubbles of air which may not be seen on ultrasonography. CT scanning can also provide precise information regarding the location and extent of air and fluid collections, such as extension into the pericholecystic tissues and the hepatic ducts. Gas in the peritoneum indicates perforation. [2]
Emphysematous Cholecystitis. Emphysematous cholecystitis in a 47-year-old man with diabetes who experienced abdominal pain. This computerized tomography scan shows gas within the wall of the gallbladder (horizontal arrow) as well as within the lumen of the gallbladder (vertical arrow). Courtesy of Helen Morehouse, MD.
CT scanning should be performed early in the evaluation when the clinical picture warrants, and it is indicated in cases where ultrasonographic or abdominal radiographic results are equivocal. Early use of CT scanning may eliminate the need for further imaging studies and can expedite appropriate clinical management. [33, 34]
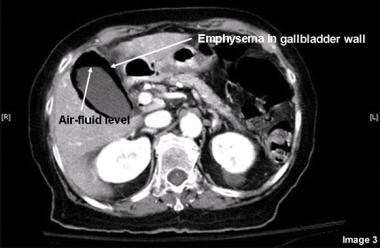 Emphysematous Cholecystitis. Computed tomography scan of a patient with emphysematous cholecystitis showing an air-fluid level in the gallbladder as well as air in the gallbladder wall.
Emphysematous Cholecystitis. Computed tomography scan of a patient with emphysematous cholecystitis showing an air-fluid level in the gallbladder as well as air in the gallbladder wall.
MRI of the Abdomen
Magnetic resonance imaging (MRI) can provide extensive information on intramural necrosis and intraluminal gas. Gas in the gallbladder lumen and wall appear as signal void areas. [35] Characteristic MRI findings of emphysematous cholecystitis are numerous floating signal void bubbles in the upper dependent portions of the gallbladder (gallstones are usually in the lower dependent portion) (see the image below).
 Emphysematous Cholecystitis. Coronal heavily T2-weighted magnetic resonance image shows numerous signal void bubbles (arrowheads) in the lumen of the distended gallbladder and the common bile duct. Courtesy of Radiological Society of North America (RSNA), originally published in Watanabe Y, Nagayama M, Okumura A, et al. MR imaging of acute biliary disorders. RadioGraphics 2007;27:477-95.
Emphysematous Cholecystitis. Coronal heavily T2-weighted magnetic resonance image shows numerous signal void bubbles (arrowheads) in the lumen of the distended gallbladder and the common bile duct. Courtesy of Radiological Society of North America (RSNA), originally published in Watanabe Y, Nagayama M, Okumura A, et al. MR imaging of acute biliary disorders. RadioGraphics 2007;27:477-95.
In a report, a gas-fluid level was shown by a signal void in the nondependent portion of the gallbladder contrasted against an intermediate signal intensity in the dependent portion. Gas within the wall was demonstrated by a rim of low signal intensity. Extraluminal gas, suggesting perforation, may cause small magnetic field inhomogeneous collections referred to as "blooming" artifacts. [36]
Histologic Findings
Following the invasion of the gallbladder wall by gas-forming bacteria, the different layers become separated (full-thickness necrosis), leading to characteristic tissue crepitus. Histologically, colonies of bacteria can be observed forming intramural abscesses, and obliteration of the cystic artery is seen secondary to endarteritis obliterans. Gallbladder contents are often purulent. Even with prompt intervention, necrosis and gangrene are observed in 75% of gallbladders at surgery. [13]
Medical Treatment
It should be emphasized that definitive management of emphysematous cholecystitis requires surgical intervention, although sporadic cases of presumed emphysematous cholecystitis treated only with antibiotics and supportive measures have been described. [14, 37] Thus, prompt surgical cholecystectomy with excision of the gallbladder and its highly infectious bile is the mainstay of treatment, because any delay may result in septic shock or mortality with this disease process.
Antibiotics
Immediately initiate empiric broad-spectrum antibiotics and and continue such therapy postoperatively until the patient clinically improves. Once microbial and culture data results are known, antibiotic agents can be specifically tailored.
Intravenous antibiotics of choice are often those with beta-lactamase inhibitor activity or combinations that provide coverage for anaerobic and gram-negative organisms. Suitable choices include ampicillin-sulbactam, meropenem or piperacillin-tazobactam (Zosyn), or dual therapy with cefepime with metronidazole for anaerobic and Bacteroides coverage.
Antibiotic regimens are suggested with the following caveats: (1) Antibiotics are not a definitive therapy for this condition, and (2) antibiotic regimens should be evaluated in light of changing bacterial sensitivities, changing antibiotic options, and changing patient characteristics.
Fluid management
Initiate fluid replacement and correction of electrolyte deficits and metabolic imbalances in preparation for surgery. It is to be emphasized that these temporary and preparatory maneuvers are not intended to reverse the basic disease process.
Consultations
Consultations with surgical, internal medicine, and gastroenterology specialists are indicated in cases of emphysematous cholecystitis. Additionally, the services of an interventional radiologist is indicated when percutaneous gallbladder drainage is considered an option—particularly for critically ill patients or those with multiple comorbidities.
If there is concern for concurrent choledocholithiasis, a gastroenterology consultation is imperative. Consultation with infectious disease specialists may be indicated for antibiotic optimization, along with other consultations based on patient comorbidities.
Interventional Radiology
Interventional radiology techniques are used in emphysematous cholecystitis to allow drainage and decompression followed by interval excision of the gallbladder. These techniques are particularly useful for critically ill and comorbid patients. [38]
Percutaneous cholecystostomy
Percutaneous cholecystostomy is an option mainly for patients in such poor clinical condition that they cannot tolerate general anesthesia. Cholecystostomy (done under local anesthesia by an interventional radiologist with ultrasonographic guidance) is considered a temporary measure to control sepsis. Once the sepsis is controlled and the patient improves, an interval (ie, 4-6 weeks later) cholecystectomy can be performed for definitive therapy. Several small clinical trials have shown that a percutaneous cholecystostomy can be used as definitive therapy in a minority of high-risk surgical patients. [5, 6]
Unresolved issues
With increasing clinical experience with percutaneous drainage, surgical survival appears to have improved. However, the following important issues remain unresolved:
-
With improving diagnostic techniques, specifically ultrasonography and computed tomography (CT) scanning, the disease process is likely to be at an early stage of its evolution. For this reason, it may be amenable to a combination of radiologic drainage, concomitant antibiotic therapy, and interval cholecystectomy in a well-prepared, stable patient.
-
Case descriptions and small clinical trials do not yet clarify the appropriate interval between interventional drainage and surgical excision of the gallbladder.
At the very least, current experience suggests that interventional radiologic drainage can be performed without increasing the overall mortality, and it appears to be a reasonable temporizing option in a critically ill patient. Some relatively recent literature suggests that percutaneous cholecystostomy tube placement may serve as the definitive treatment for a minority of patients with this pathology, though further large-scale studies are needed for confirmation. [5] Further experience is required to determine the role of percutaneous transhepatic gallbladder drainage. The final management algorithm for emphysematous cholecystitis has yet to been written.
Surgical Treatment
Management of emphysematous cholecystitis is primarily surgical. Antibiotics and fluid replacement are started immediately to stabilize the patient, but because of the risk of perforation in emphysematous cholecystitis, surgery should be performed emergently. Overall, surgical mortality may be as high as 25%. [17]
Open or laparoscopic cholecystectomy
Traditionally, early open cholecystectomy was the initial treatment of choice acute emphysematous cholecystitis. Laparoscopic cholecystectomy for this condition was first described in 1994, and experience with this technique continues to increase. Although laparoscopic cholecystectomy is feasible, there is no current comparative analysis to compare mortality and postoperative complications between the two approaches. A preoperative diagnosis of perforation would likely preclude a laparoscopic approach, as demonstrated by preoperative abdominal imaging by computed tomography (CT) scanning or magnetic resonance imaging (MRI). [39, 40]
As long as fundamental surgical principles are maintained (and depending on the patient and surgeon skill/comfort level) laparoscopic cholecystectomy is a safe and effective treatment for this disease process. [39, 40, 41] Surgeons should be aware that there is a high conversion rate to open laparotomy due to the anatomic distortion caused by acute inflammation, [42] although with current techniques, emphysematous cholecystitis can be treated initially with a laparoscopic approach while maintaining a low threshold for conversion. Due to the degree of inflammation present, the surgeon should consider postoperative drainage of the gallbladder fossa (eg, Jackson-Pratt drain) to potentially decrease the risk of postoperative fluid collections and abscess formation.
Common bile duct exploration
If the patient has concurrent common bile duct stones, common bile duct exploration can be done transcystically or via choledochotomy, open or laparoscopic, to clear the common bile duct. An alternative choice is to consider a postoperative endoscopic retrograde cholangiopancreatography (ERCP), performed by a gastroenterology consultant.
Adjuvant Therapy
Hyperbaric oxygen therapy (HBO) has been described as an adjuvant therapy to surgery for emphysematous cholecystitis. [18] In a small study from Croatia, patients with acute emphysematous cholecystitis were exposed to HBO within 8 hours after surgery at a pressure of 3.0 bars 3 times daily for 90 minutes, with an air break of 15 minutes within the first 24 hours and for the next 5 days twice daily under the same conditions.
The rationale for the use of HBO on clostridia and other anaerobes is based on the formation of free radicals in the absence of free-radical degrading enzymes (eg, superoxide dismutases, catalases, and peroxidases). Achieving tissue partial oxygen pressure above 250 mmHg is necessary to stop bacterial growth and inactivate the exotoxins.
Note: Although HBO may be beneficial as adjunctive therapy, it is not considered an adequate alternative to surgical cholecystectomy.
Dietary and Activity Considerations
The episode of emphysematous cholecystitis itself should not impose any dietary requirements. However, the patient should be kept on nothing by mouth (NPO) until a surgical consultation has taken place. Any gallbladder stimulation secondary to oral intake is likely to exacerbate the pathophysiologic process.
Once cholecystectomy has been successfully performed, the patient can be started on a diet depending on the clinical scenario and advanced gradually. Upon discharge, dietary recommendations reflect the presence of active comorbid diseases.
Early postoperative activity is dictated by surgical considerations. Upon discharge after the operation, patients should experience no limitation of activity that was not present before the episode.
Postoperative Monitoring
Patients should be observed for the development of pseudomembranous enterocolitis manifested by diarrhea, particularly in the setting of recent antibiotic use. This diagnosis is established by demonstrating C difficile toxin in the stool. Treatment is usually started with oral vancomycin, and it sometimes escalates to include intravenous metronidazole and rectal vancomycin enemas based on the severity of the condition.
Patients should also be observed for the development of early postoperative complications, including a cystic duct stump leak, a retained common bile duct stone, a common bile duct stricture, or postcholecystectomy diarrhea (see Complications).
Patient education
Educate patients to watch for features of bile duct obstruction, including changes in the color of the skin, eyes, urine, and stool, which may indicate a retained common duct stone or stricture.
Complications and Prognosis
Septic shock
The most feared complication of emphysematous cholecystitis is potentially lethal septic shock, which can occur in up to 25% of cases. Untreated emphysematous cholecystitis can progress to soft-tissue gas gangrene due to the hematogenous spread of microorganisms to the muscles and eventual septic shock and death. [2] Once the diagnosis of acute emphysematous cholecystitis is made, the patient should be resuscitated, broad-spectrum antibiotics initiated, and surgical treatment pursued without delay.
Morbidity can be as high as 50%, often related to the sequelae of septic shock. [17] Other postoperative complications include postoperative abscess, bile leak, bile duct injury, and wound infection. Placing a closed-suction drain (eg, Jackson-Pratt drain) at the time of operation may help decrease the rate of fluid collections and subsequent abscess formation postoperatively. Bile duct injury may be avoided by intraoperative cholangiography to help delineate the biliary tree anatomy, especially in cases with dense inflammation causing distortion of the anatomy in the Calot triangle. [43]
Gangrenous cholecystitis and gallbladder perforation
Emphysematous cholecystitis evolves to gangrenous cholecystitis in 75% of the cases. [17] Once gangrenous cholecystitis is present, perforation of the gallbladder is often inevitable, occasionally giving rise to pneumoperitoneum and frank peritonitis. Both gangrene and perforation are relatively infrequent in simple acute calculous cholecystitis. In fact, the incidence of gangrene is 30 times greater, and the incidence of perforation is 5-fold higher in emphysematous cholecystitis as compared to simple acute cholecystitis. [13]
There is no significant difference in the mortality and in the sequence of gangrene and perforation in acute emphysematous cholecystitis between diabetic and nondiabetic individuals. [17] Gangrene and perforation have also been noted in patients with emphysematous cholecystitis who were symptomatic for less than 72 hours, reinforcing the concept that the initial presentation may be misleading to the clinician and that the patient can rapidly deteriorate clinically with hemodynamic collapse and septic shock.
Overall mortality
The overall mortality from emphysematous cholecystitis ranges from 15% to 25%, often due to a delay in the diagnosis. These rates are 5 times the operative mortality for nonemphysematous cholecystitis. In addition to the septic character of the disease, comorbidities including advanced age and diabetes mellitus are associated with greater mortality. [13]
Special Concerns
Although most patients with emphysematous cholecystitis have the typical clinical presentation as previously described (see Presentation), there are some issues the clinician must be aware of.
Older patients may not present with significant abdominal pain or fever, even in the presence of frank peritonitis. The Murphy sign may be absent. [3]
Acute emphysematous cholecystitis is a separate entity compared with acute calculous cholecystitis. The epidemiologic profile and the disease course (rapid progression) are different. The clinician can be misled by a deceptively mild initial presentation. Once the diagnosis is made radiographically, the patient should undergo operative treatment without delay.
A plain film of the abdomen may not be diagnostic. A normal finding on a plain film does not exclude the diagnosis of emphysematous cholecystitis. [14, 22, 25] In addition, the gallbladder may not be readily observed on ultrasonographic examination. Indeed, the apparent absence of a visualized gallbladder on ultrasonograms in a patient with biliary tract features should prompt the clinician to proceed to an abdominal computed tomography (CT) scan. [14] Ultimately, a CT scan is the most reliable and valuable diagnostic test for emphysematous cholecystitis.
Delay in the diagnosis or treatment and any intraoperative/technical misadventures may expose the clinician to legal liability due to a high rate of gallbladder perforation. An intraoperative cholangiogram to help delineate the biliary anatomy—which may be distorted due to the presence of extensive inflammation—may help decrease the rate of bile duct injury.
-
Emphysematous Cholecystitis. Emphysematous cholecystitis in a 47-year-old man with diabetes who experienced abdominal pain. This computerized tomography scan shows gas within the wall of the gallbladder (horizontal arrow) as well as within the lumen of the gallbladder (vertical arrow). Courtesy of Helen Morehouse, MD.
-
Emphysematous Cholecystitis. Emphysematous cholecystitis in a 61-year-old nondiabetic man with right upper quadrant abdominal pain, fever, and leukocytosis. This plain film shows the gallbladder with multiple stones. The wall of the fundus is delineated by intramural gas. Extramural gas also appears to be present in the soft tissues over the superior aspect of the gallbladder.
-
Emphysematous Cholecystitis. Emphysematous cholecystitis in a 78-year-old man with diabetes with minimal abdominal distress. The plain film shows an enlarged gallbladder with multiple stones. The wall of the gallbladder is outlined by intramural gas.
-
Emphysematous Cholecystitis. Plain abdominal radiograph showing air in the gallbladder (arrow).
-
Emphysematous Cholecystitis. Computed tomography scan of a patient with emphysematous cholecystitis showing an air-fluid level in the gallbladder as well as air in the gallbladder wall.
-
Emphysematous Cholecystitis. Coronal heavily T2-weighted magnetic resonance image shows numerous signal void bubbles (arrowheads) in the lumen of the distended gallbladder and the common bile duct. Courtesy of Radiological Society of North America (RSNA), originally published in Watanabe Y, Nagayama M, Okumura A, et al. MR imaging of acute biliary disorders. RadioGraphics 2007;27:477-95.
Tables

What would you like to print?
- Overview
- Etiology and Pathophysiology
- Presentation
- Diagnosis
- Laboratory Studies
- Abdominal Radiography
- Abdominal Ultrasonography
- CT Scanning of the Abdomen
- MRI of the Abdomen
- Histologic Findings
- Medical Treatment
- Interventional Radiology
- Surgical Treatment
- Adjuvant Therapy
- Dietary and Activity Considerations
- Postoperative Monitoring
- Complications and Prognosis
- Special Concerns
- Show All
- Media Gallery
- References