Practice Essentials
Immunoglobulin A (IgA) nephropathy is characterized by predominant IgA deposition in the glomerular mesangium. [1, 2] It is one of the most common causes of glomerulonephritis in the world. [3, 4, 5] IgA nephropathy was first described by Berger and Hinglais in 1968, and is also known as Berger disease. [6, 7]
Pathologically, a spectrum of glomerular lesions can be seen, but mesangial proliferation with prominent IgA deposition is observed in almost all biopsies. See the images below.
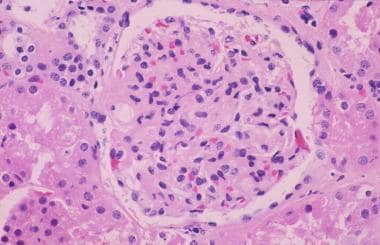 Light microscopy of a glomerulus from a patient with immunoglobulin A nephropathy showing increased mesangial matrix and cellularity.
Light microscopy of a glomerulus from a patient with immunoglobulin A nephropathy showing increased mesangial matrix and cellularity.
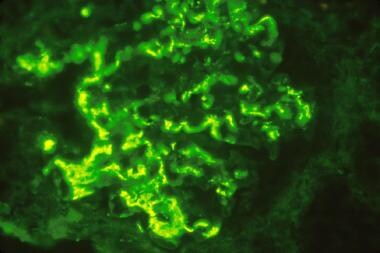 Immunofluorescence microscopy demonstrating large mesangial immunoglobulin A (IgA) deposits diagnostic of IgA nephropathy.
Immunofluorescence microscopy demonstrating large mesangial immunoglobulin A (IgA) deposits diagnostic of IgA nephropathy.
Although IgA nephropathy is a limited nonsystemic kidney disease, many systemic illnesses are sporadically associated with mesangial IgA deposition. Henoch-Schönlein purpura (HSP), a systemic illness, has been closely linked to IgA nephropathy. Other systemic diseases in which mesangial deposits of IgA are regularly observed include systemic lupus erythematosus, hepatitis, dermatitis herpetiformis, and ankylosing spondylitis.
Signs and symptoms
Patients with IgA nephropathy (especially adults) may be asymptomatic, albeit with persistent microscopic hematuria and proteinuria and often hypertension. Symptomatic presentations include the following:
-
Episodic gross hematuria
-
Rapidly progressive glomerulonephritis
-
Proteinuria- less than 3 g/day
-
Nephrotic syndrome
-
Chronic kidney disease
See Presentation for more detail.
Diagnosis
The workup for IgA nephropathy includes the following:
-
Urinalysis of a first-void urine sample, with sediment examination for RBCs and RBC casts
-
Proteinuria testing (24-hour measurement of urinary protein or urine protein/creatinine ratio, plus urine protein electrophoresis in patients older than 50 years with proteinuria, to exclude monoclonal light chains)
-
Kidney function assessment with 24-hour creatinine clearance test or estimation of glomerular filtration rate
-
Kidney biopsy to confirm the diagnosis
See Workup for more detail.
Management
Treatment of IgA nephropathy includes the following:
-
All patients should be given supportive therapy to control hypertension and proteinuria, including renin-angiotensin system blockade and dietary sodium restriction.
-
Tonsillectomy is appropriate only for patients with recurrent tonsillar infections.
-
Immunosuppression has become controversial. [8] Corticosteroids are the option with the most convincing evidence to support their use, but if used, they should be administered only to carefully selected patients, and preferably should not be given for more than 6 months.
-
Cyclophosphamide should be reserved for rapidly progressive crescentic glomerulonephritis.
The US Food and Drug Administration (FDA) has approved the following agents to reduce proteinuria in adults with IgA nephropathy who are at risk of rapid disease progression:
-
A targeted-release formulation of the corticosteroid budesonide (Tarpeyo)
-
Sparsentan (Filspari), a dual angiotensin II and endothelin-1 receptor antagonist
-
Iptacopan (Fabhalta), a complement inhibitor
Kidney transplantation is effective in patients with IgA nephropathy that has progressed to end-stage renal disease. However, the disorder frequently recurs after transplantation
See Treatment and Medication for more detail.
For discussion of this disorder in children, see Pediatric IgA Nephropathy.
For patient education resources, see Blood in the Urine.
For further information, see Mayo Clinic - Kidney Transplant Information.
Pathophysiology
IgA nephropathy appears to result from an ordered sequence of events, starting with galactose-deficient IgA1, which contains less than a full complement of galactose residues on the O-glycans in the hinge region of the heavy chains. [9] These may act as auto-antigens that trigger the production of glycan-specific autoantibodies and the formation of circulating immune complexes that are deposited in renal mesangium. These then induce glomerular injury through pro-inflammatory cytokine release, chemokine secretion, and the resultant migration of macrophages into the kidney. [10] Immune complexes formed by IgG or IgA antibodies with galactose-deficient IgA lead to deposition in the glomerulus.
Deposited IgA is predominantly polymeric IgA1, which is mainly derived from the mucosal immune system. The association of some cases of IgA nephropathy with syndromes that affect the respiratory tract or gastrointestinal tract, such as celiac disease, led to the suggestion that IgA nephropathy is a disease of the mucosal immune system. This concept is also supported by the clinical observation that hematuria worsens during or after upper respiratory tract or gastrointestinal tract infections. Any bacterial or viral infections can precipitate IgA nephropathy.
An association between IgA nephropathy and inflammatory bowel disease (IBD)—especially Crohn disease, but also ulcerative colitis—has been reported. IBD may be diagnosed before or after onset of IgA nephropathy. [11] A Swedish population-based cohort study found elevated risk of progression to end-stage kidney disease in patients with comorbid IgA nephropathy and IBD. [12]
Data strongly suggest that the alternative complement pathway plays a key role in the pathophysiology of IgA nephropathy. Although the formation of immune complexes and their deposition in the glomerular mesangium cannot activate complement through the classic pathway, it may directly activate the alternative complement pathway, which contributes to kidney inflammation and glomerular injury. [13]
Epidemiology
Frequency
United States
IgA nephropathy is found in about 10% of biopsies performed for glomerular disease in the United States. Prevalence rates are lower in the United States than in Asian countries. These lower rates may be influenced by a conservative approach by nephrologists in the US, who are reluctant to perform kidney biopsies in asymptomatic patients with only mild abnormalities on urinalyses.
International
Distribution of IgA nephropathy varies in different geographic regions throughout the world. IgA nephropathy is observed in up to 40% of all biopsies performed for glomerular disease in Asia, compared with 20% in Europe and 10% in North America. High prevalence rates are observed in Singapore, Japan, Australia, Hong Kong, Finland, and southern Europe, whereas low prevalence rates are the rule in the United Kingdom, Canada, and the United States.
A study from Scotland found a significant twofold increase in the diagnosis of IgA nephropathy in the patients residing in the most socioeconomically deprived areas compared with the least deprived ones. The variation was not explained by the demographics of the underlying population. [14]
In a study by Zhou from eastern China utilizing kidney biopsies from 2001-2017, IgA nephropathy was the most common type of primary glomerulonephritis, accounting for 50% of cases. The diagnosis rate of IgA nephropathy remained steady over that 15-year period; however, the prevalence of membranous nephropathy increased, becoming the second most common type. [15]
In Asia, routine urinalyses are performed for schoolchildren, and kidney biopsies are performed for patients with asymptomatic hematuria, thus raising the reported prevalence of the disease. The estimated annual incidence in Japan is 3.9–4.5 per 100,000 population. [16]
The prevalence of IgA nephropathy is highest in geographic areas with large numbers of endemic helminthic species that infest humans, and most of the IgA nephropathy susceptibility loci identified by genome-wide association studies include genes involved in the maintenance of the intestinal epithelial barrier and response to mucosal pathogens, which would confer protection against helminthic infestation. Thus, the increased risk of IgA nephropathy in these populations may be an untoward consequence of a protective adaptation to helminthic infections. It would also explain the association of mucosal infections as a frequent trigger for IgA nephropathy. [17]
Mortality/morbidity
This disorder is thought to follow a benign course in most cases. However, many patients are at risk for slow progression to end-stage renal disease, which develops in approximately 15% of patients by 10 years and 20% by 20 years, though these percentages depend on how the disease is defined.
Race-, sex-, and age-related demographics
IgA nephropathy is more common in Asians and Whites and is rare in Blacks, both in the United States and in Africa. The condition is frequently observed in Native Americans of the Zuni and Navajo tribes.
IgA nephropathy is more common in males than in females. Virtually all studies show a male predominance of at least 2:1, with reported ratios of up to 6:1. [18] The higher male predilection is observed in White patients in northern Europe and the United States.
IgA nephropathy can affect all ages but is most common in the second and third decades of life. Eighty percent of patients are aged 16-35 years at the time of diagnosis. The condition is uncommon in children younger than 10 years.
Lifestyle and risk of progression to end-stage renal disease
In a study by Huang et al in Chinese subjects with IgA nephropathy, which compared cases that progressed to end-stage renal disease (ESRD) with controls that did not, the proportion of patients who were males, smokers, alcohol drinkers, and physically inactive was signficantly higher in cases than in controls. Alcohol use proved to be an independent risk factor for progression to ESRD, while regular exercise was associated with decreased risk; males who did not exercise seemed especially likely to progress to ESRD. These authors concluded that physical exercise should be encouraged in IgA nephropathy patients, especially in males, for a better renal outcome, and cessation of alcohol use might help prevent disease progression. [19]
Prognosis
Although IgA nephropathy usually follows a benign course, end-stage renal disease (ESRD) develops in 15-20% of patients within 10 years of onset and in about 25-30% of patients by 20 years. Efforts have been made to determine clinical and histologic features associated with progression to ESRD. [20, 21]
The Oxford classification of IgA nephropathy, or MEST score, published in 2009, comprises four histologic features that are independent predictors of clinical outcome. [4] The IgA Nephropathy Classification Working Group added crescents to the Oxford classification, to form the MEST-C score. [22, 23] The features that determine the MEST-C score are as follows:
-
M – Mesangial cellularity, defined as more than four mesangial cells in any mesangial area of a glomerulus: M0 is mesangial cellularity in < 50% of glomeruli; M1, ≥50%
-
E – Endocapillary proliferation, defined as hypercellularity due to an increased number of cells within glomerular capillary lumina: E0 is absence of hypercellularity; E1 is hypercellularity in any glomeruli
-
S – Segmental glomerulosclerosis, defined as adhesion or sclerosis (obliteration of capillary lumina by matrix) in part of but not the whole glomerular tuft: S0 is absence of segmental glomerulosclerosis, S1 is presence of segmental glomerulosclerosis in any glomerulus
-
T – Tubular atrophy/interstitial fibrosis, defined as the estimated percentage of cortical area showing tubular atrophy or interstitial fibrosis, whichever is greater: T0 is 0-25%; T1 is 25-50%; T2 is > 50%
-
C – Crescents: C0 (no crescents), C1 (crescents in less than one-fourth of glomeruli), C2 (crescents in over one-fourth of glomeruli).
The clinical significance of the individual MEST-C features is as follows:
-
M1 – Worse outcomes than M0
-
E1 – Worse renal survival in patients not on immunosuppression and improved renal survival with immunosuppression
-
S1 – Predictive of worse outcomes
-
T – Strongest predictor of worse outcomes
-
C1 – Predictive of worse outcomes if no immunosuppression is given, but not if immunosuppression is used; C2 is predictive of worse outcomes regardless of immunosuppression
Other predictors of poor renal outcomes include the following:
-
High serum creatinine level (> 120 mmol/L) at presentation
-
Hypertension (diastolic pressure > 95 mm Hg or need for antihypertensive treatment)
-
Proteinuria: Urinary protein excretion < 1 g/24 hr is associated with 56% renal survival and > 3.5 g/24 hr with 7% renal survival [24]
-
Extensive interstitial fibrosis and tubular atrophy on kidney biopsy
-
C4d staining on biopsy
A calculator for estimating the risk of progression to ESRD in patients with IgA nephropathy has been developed by Xie et al, based on a cohort of 619 Chinese patients. [25] It has yet to be validated in other ethnic groups. The calculator uses four variables:
-
Glomerular filtration rate
-
Hemoglobin level
-
Serum albumin level
-
Systolic blood pressure
-
Light microscopy of a glomerulus from a patient with immunoglobulin A nephropathy showing increased mesangial matrix and cellularity.
-
Electron microscopy showing large dark mesangial deposits.
-
Immunofluorescence microscopy demonstrating large mesangial immunoglobulin A (IgA) deposits diagnostic of IgA nephropathy.
