Practice Essentials
Human Cytomegalovirus (CMV) is a member of the family Herpesviridae, also known as Human Herpesvirus 5 (HHV-5). It is the largest (220 nm in diameter) and most complex herpesvirus, with a 235,000 double-stranded DNA genome. CMV seroprevalence in immunocompetent adults varies from 40-100% globally. [1]
Signs and symptoms
CMV usually causes an asymptomatic infection or produces mild flulike symptoms; afterwards, it remains latent throughout life and may reactivate.
Most patients with CMV infection exhibit few clinical findings on physical examination.
-
Primary CMV infection may be a cause of fever of unknown origin.
-
Symptoms, when apparent, develop 9-60 days after primary infection.
-
Pharyngitis may be present.
-
Examination of the lungs may reveal fine crackles.
-
The lymph nodes and spleen may be enlarged, so CMV should be included in the differential diagnoses of infections that produce lymphadenopathy.
In immunocompromised individuals, symptomatic disease usually manifests as a mononucleosis syndrome. Symptomatic CMV disease can affect almost every organ of the body, resulting in fever of unknown origin, pneumonia, hepatitis, encephalitis, myelitis, colitis, uveitis, retinitis, and neuropathy. Rarer manifestations of CMV infections in immunocompetent individuals include Guillain-Barré syndrome, meningoencephalitis, pericarditis, myocarditis, thrombocytopenia, and hemolytic anemia.
CMV is an opportunistic infection in patients with advanced HIV/AIDS and can effect multiorgan systems. The most common sites of CMV related gastrointestinal infection are the esophagus and the colon. These patients may have concurrent CMV reitinitis and should have formal opthalmologic screening.
See Clinical Presentation for more detail.
Diagnosis
Lab studies
CMV has been detected via culture, serologies, antigen assays, polymerase chain reaction (PCR), and cytopathology. In the transplant population, antigen assays or PCR is used (sometimes in conjunction with cytopathology) for diagnosis and treatment determinations.
Imaging studies
The diagnosis of CMV pneumonia can be suggested by chest radiography findings, but these findings cannot be used to differentiate between other common causes of pneumonia in immunocompromised hosts. A chest radiograph finding consistent with pneumonia and a bronchoalveolar lavage (BAL) result that is CMV positive is a common method for diagnosis.
See Workup for more details.
Management
Healthy people who are infected with CMV but who have no symptoms usually do not require medical treatment.
Antiviral treatment is used for immunocompromised individuals who have eye infections or life-threatening illnesses due to CMV. The drug of choice for prevention of CMV disease in solid-organ transplant patients is valganciclovir. [2] Other than CMV retinitis, however, ganciclovir remains the mainstay of treatment, at least initially.
Second-line treatments include foscarnet, cidofovir, or maribavir.
There is no vaccine to prevent CMV infection.
See Treatment and Medication for more detail.
Background
Cytomegalovirus (CMV) is a double-stranded DNA virus and is a member of the Herpesviridae family. The other family members include herpes simplex virus type 1 (HSV-1 or HHV-1) and herpes simplex virus type 2 (HSV-2 or HHV-2), varicella zoster virus (VZV), human herpes virus (HHV)–6, HHV-7, and HHV-8. CMV shares many attributes with other herpes viruses, including genome, virion structure, and the ability to cause latent and persistent infections. CMV has the largest genome of the herpes viruses. Replication may be categorized into immediate early, delayed early, and late gene expression based on time of synthesis after infection. The DNA is replicated by rolling circles. Human CMV grows only in human cells and replicates best in human fibroblasts.
At least 50-60% of the US population has been exposed to CMV, [3] with a prevalence of more than 90% in high-risk groups (eg, male homosexuals), and outside of the US prevalence can be more than 90%. [4, 5, 6] The prevailing age of infection varies worldwide. In developing countries, most infections are acquired during childhood, whereas in developed countries, up to 50% of young adults are CMV seronegative. The incidence of CMV seropositivity rises with age and in a US-based study was reported to increase from 36% in children aged 6-11 years to 91% in individuals older than 80 years. [7] Other factors associated with CMV seropositivity include ethnicity (77% in Mexican Americans and 71% in Blacks), [8] female sex, foreign-born status, and low socioeconomic status. [8]
CMV usually causes an asymptomatic infection; afterward, it remains latent throughout life and may reactivate. Infection is defined as isolation of CMV, its viral proteins, or its nucleic acid from any tissue sample or body fluid. [9] In immunocompetent individuals, symptomatic disease usually manifests as a mononucleosis syndrome, which was first described in adults in 1965. [10]
Clinically significant CMV disease (reactivation of previously latent infection or newly acquired infection) frequently develops in patients immunocompromised by HIV infection, solid-organ transplantation, or bone marrow transplantation, as well as in those receiving high-dose steroids, tumor necrosis antagonists, or other immunosuppressing medications for conditions such as systemic lupus erythematosus (SLE), rheumatoid arthritis, Crohn disease, or psoriasis, among others. In patients coinfected with HIV, CMV infection leads to progression to AIDS and eventually death, even in those receiving antiretroviral therapy (ART). [11]
Symptomatic CMV disease in immunocompromised individuals can affect almost every organ of the body, resulting in fever of unknown origin, pneumonia, hepatitis, encephalitis, myelitis, colitis, uveitis, retinitis, and neuropathy.
Individuals at an increased risk for CMV infection include individuals who attend or work at daycare centers, patients who undergo blood transfusions, persons who have multiple sex partners, and recipients of CMV mismatched organ or bone marrow transplants.
CMV is transmitted from person to person via close contact with an individual who is excreting the virus. It can be spread through the placenta, blood transfusions, organ transplantation, and breast milk. It also can be spread through sexual transmission.
In the United States, congenital CMV transmission from a mother with acute infection during pregnancy is a significant cause of neurologic abnormalities and deafness in approximately 8000 newborns annually. [12, 13]
Multiple genetically distinct strains of CMV exist. Differences in genotypes may be associated with differences in virulence. Infection with more than one strain of CMV is possible and has been observed in organ transplant recipients. Dual infection is a possible explanation for congenital CMV infection in children of CMV-seropositive mothers.
Pathophysiology
CMV is a lytic virus that causes a cytopathic effect in vitro and in vivo. The pathologic hallmark of CMV infection is an enlarged cell with viral inclusion bodies. Cells that exhibit cytomegaly also are seen in infections caused by other Betaherpesvirinae. The microscopic description given to these cells is most commonly an "owl's eye," depicted in the image below. Although considered diagnostic, such histologic findings may be minimal or absent in infected organs.
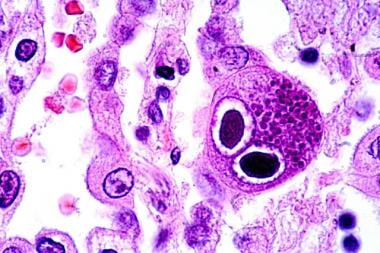 Hematoxylin-eosin–stained lung section showing typical owl-eye inclusions (480X). Courtesy of Danny L Wiedbrauk, PhD, Scientific Director, Virology & Molecular Biology, Warde Medical Laboratory, Ann Arbor, Michigan.
Hematoxylin-eosin–stained lung section showing typical owl-eye inclusions (480X). Courtesy of Danny L Wiedbrauk, PhD, Scientific Director, Virology & Molecular Biology, Warde Medical Laboratory, Ann Arbor, Michigan.
When the host is infected, CMV DNA can be detected with polymerase chain reaction (PCR) in all the different cell lineages and organ systems in the body. Upon initial infection, CMV infects the epithelial cells of the salivary gland, resulting in a persistent infection and viral shedding. Infection of the genitourinary system leads to clinically inconsequential viruria. Despite ongoing viral replication in the kidney, renal dysfunction is rare except in renal transplant recipients, in whom CMV is associated with rare cases of glomerulopathy and possible graft rejection.
Immunology
Primary CMV infection is defined as infection in an individual who was previously CMV seronegative. [9] In these patients, CMV immunoglobulin M (IgM) antibodies may be found as early as 4-7 weeks after initial infection and may persist as long as 16-20 weeks. Most neutralizing antibodies are directed against an envelope glycoprotein gB. Studies have shown that more than 50% of neutralizing activity in convalescent serum is attributable to glycoprotein gB. However, virion tegument proteins such as pp150, pp28, and pp65 evoke strong and durable antibody responses.
CMV is an immunomodulatory virus and may aggravate underlying immune disorders (eg, SLE).
The presence of CMV DNA in the blood and viruria are commonly found in healthy CMV seropositive women. Naturally acquired immunity to the virus does not seem to prevent reinfection or the duration of viral shedding. [14]
Cell-mediated immunity is considered the most important factor in controlling CMV infection. Patients deficient in cell-mediated immunity are at greatest risk for CMV disease. CMV-specific CD4+ and CD8+ lymphocytes play an important role in immune protection after primary infection or reactivation of latent disease. Studies of bone marrow transplant recipients have revealed that those who do not develop CMV-specific CD4+ or CD8+ cells are at higher risk for CMV pneumonitis. Additionally, no cases of CMV pneumonia have been reported in allogeneic marrow transplant recipients receiving infusions of CMV-specific CD8+ cells. [15]
Primary cytomegalovirus infection and viremia
Both replication of CMV DNA and morphogenesis of the virion capsid take place in the nucleus. Following maturation of the capsid, newly synthesized viral DNA is cleaved by an enzyme that results in packaging of linear genomic DNA. Subsequently, viral DNA-containing capsids acquire an inner layer of tegument proteins during their egress from the nucleus, including essential interactions between proteins and capsid protein, that stabilize the interaction between the capsid and the inner tegument layer of the virion. This then is transported along the cytoskeleton until the particle is enveloped. After this, the virus is released from the cell. [1]
Congenital cytomegalovirus disease
CMV is the leading cause of congenital infection worldwide (0.2-6.1% of live births), as well as the most common congenital viral infection in the United States (20000 to 30000 infants/year, mostly Black infants) and the leading cause of sensorineural hearing loss and neurodevelopmental delay in children. Congenital CMV-related sequelae affect over 5000 children per year and add significant cost in direct medical care in the United States. The transplacental transmission rate after maternal primary infection is around 32%. The risk for transmission is low following maternal infection occurring more than 11 weeks before conception. [16, 17, 18, 19]
Most infants are asymptomatic, however, symptomatic infants are seen in about 10% of the patients with a broad range of disease manifestations. These include thrombocytopenia, petechiae, hepatomegaly, splenomegaly, hepatitis, intrauterine growth restriction, CNS involvement (microcephaly, ventriculomegaly, intracerebral calcifications, white matter changes with seizures, and abnormal tone), ophthalmologic abnormalities (chorioretinitis, optic atrophy), and sensorineural hearing loss. Mortality due to congenital CMV infection is low (approximately 4% of infants). Symptomatic disease can be classified as moderate to severe (multiple manifestations with or without CNS involvement) or mild disease (1-2 manifestations with no CNS involvement). [16, 19]
In the pediatric population, congenital CMV infection is the most common cause of non-genetic sensorineural hearing loss (SNHL); this also is the most common permanent sequelae of congenital CMV infection. Around 40-60% of these neonates are at risk for permanent sequelae. [20] Other complications include cognitive impairment, chorioretinitis, and cerebral palsy. Other manifestations include motor deficits and seizures as well in 23% and 19%, respectively. CMV screening approaches could lead to the identification of many more infants with congenital CMV infection than are identified because of clinical signs. Trials are ongoing to formulate a vaccine for pregnant individuals. [16, 21, 22]
Increased rates of reactivation and cervical shedding are seen in advanced stages of gestation, and congenital infection is associated with sequelae previously described. Prevention includes hand hygiene to minimize occupationally acquired CMV (such as daycare centers), as well as limiting the number of sexual partners (during pregnancy). [23]
Cytomegalovirus pneumonia
This can be seen in an immunocompetent as well as an immunocompromised host, including hematopoietic stem cell transplantation (HSCT) recipients and solid organ transplant recipients. Pneumonitis is the most common manifestation of CMV infection in HSCT recipients and has a high mortality. Especially in neonates, it can lead to chronic lung disease and fibrosis. Symptoms include dry cough, shortness of breath, and fever. Imaging abnormalities include abnormal chest Xray with interstitial infiltrates as well as ground-glass opacities seen in computed tomography (CT) scans that could be nonspecific for CMV infections and should be correlated with serologic testing, viral load, respiratory samples, and histopathology. [24]
Cytomegalovirus hepatitis
CMV hepatitis is defined as elevated bilirubin and/or liver enzymes levels in combination with the detection of CMV in the absence of other causes for hepatitis. [9] CMV may be detected via culture, histopathology, immunohistochemistry, or in situ hybridization. CMV PCR alone is not satisfactory for diagnosis, as a positive result may reflect transient viral shedding. [9] The first described case of CMV hepatitis involved a child with chorioretinitis, hepatosplenomegaly, and cerebral calcifications.
Hepatitis has been commonly observed in patients with primary CMV infection and mononucleosis. Levels of hepatocellular enzymes may be mildly and transiently increased, and, in rare cases, jaundice may develop. The prognosis of CMV hepatitis in immunocompetent hosts typically is favorable, but death has been reported in immunosuppressed patients. Histology typically reveals mononuclear cell infiltration of the portal areas but also may reveal granulomatous inflammation. [25]
Cytomegalovirus gastritis and colitis
CMV GI disease is defined as the combination of symptoms of the upper and lower GI tract, mucosal lesions visible on endoscopy, and detection of CMV via culture, histopathology, immunohistochemistry, or in situ hybridization. [9] CMV colitis first was described in 1985 in 2 homosexual men who presented with abdominal pain, diarrhea, and hematochezia. [26] CMV PCR alone is insufficient for diagnosis, as a positive result may simply reflect transient viral shedding.
CMV may infect the GI tract from the oral cavity through the colon. The typical manifestation of disease is ulcerative lesions. In the oral cavity, these may be indistinguishable from ulcers caused by HSV or aphthous ulceration. Gastritis may present as abdominal pain and even hematemesis, whereas colitis more frequently presents as a diarrheal illness. CMV disease of the GI tract often is shorter-lived than that of other organ systems because of the frequent sloughing of infected cells of the GI mucosa.
Cytomegalovirus CNS disease
CMV CNS disease is defined as CNS symptoms in combination with CMV detection in CSF (culture, PCR) or brain biopsy tissue (culture, histopathology, immunohistochemistry, in situ hybridization). [9] The association between CMV and Guillain-Barré Syndrome involves 2 groups. Younger patients (typically < 35 y) present with sensory defects and facial palsy, antiganglioside (GM2) IgM response, and milder long-term sequelae. [27] A second group includes women older than 50 years. These observations were made in France and thus may not be applicable to other populations due to different ages of primary CMV exposure.
Cytomegalovirus retinitis
CMV retinitis is one of the most common opportunistic infections in persons with AIDS, typically those with CD4+ lymphocyte counts below 50 cells/µL. Although the number of cases has decreased with the use of antiretroviral therapy (ART), new cases continue to be reported. Individuals with CMV retinitis typically exhibit a progressive decrease in visual acuity, which may progress to blindness if untreated. Unilateral and bilateral disease may exist. Long-term CMV treatment is necessary to prevent retinitis relapse. All lesions suspected to be CMV retinitis must be confirmed by an ophthalmologist.
Immune reconstitution syndrome (IRIS) is reported in 16-63% of HIV-infected patients with CMV retinitis following the initiation of ART. [28, 29, 30] In one study, the median time to IRIS following ART initiation was 43 weeks but has been reported as early as 4 weeks or as late as 4 years. [31, 29] CMV IRIS may manifest as painless floaters, blurred vision, photopia, decreased visual acuity, or ocular pain. Some patients may develop macular edema leading to vision loss or proliferative vitreoretinopathy, spontaneous vitreal hemorrhage, and retinal detachment.
Cytomegalovirus nephritis
CMV nephritis is defined as CMV detection in combination with a renal biopsy showing CMV-associated changes in the setting of renal failure. [9] CMV PCR alone is inadequate for diagnosis. Of note, detection of CMV in the urine of a patient with renal failure does not meet diagnostic criteria for CMV nephritis. [9] CMV viremia has been associated with acute glomerular injury. [32]
Cytomegalovirus syndrome
In general, it is better to avoid this term in stem cell transplant recipients, as other viruses (eg, HHV-6) also can cause fever and bone marrow suppression. [9] However, in solid organ transplant recipients, CMV syndrome is better defined: fever (>38°C) for at least 2 days within a 4-day period, CMV detection in blood, and either neutropenia or thrombocytopenia. [9]
Graft versus host disease
CMV infection has been associated with acute graft verus host disease in bone marrow transplant recipients. Multiple genotypes (gB 1-4) of CMV exist, each with variations in the gene encoding envelope glycoprotein gB. The association of gB types with acute graft versus host disease and death related to myelosuppression has been examined. Taking into account disease type, donor-recipient HLA matching, donor CMV serostatus, and age, Torok-Storb et al (1997) found that gB3 and gB4 were linked to a higher degree of myelosuppression and death. [33] Interestingly, no specific CMV genotypes were linked to worse outcome in solid organ transplant recipients, although mixed gB genotype infections were associated with higher viral loads and delayed viral clearance. [34]
Frequency
United States
CMV infection is thought to be specific to humans. The age at presentation, clinical manifestations, and route of infection may vary from person to person, but very few people escape infection during their lifetime.
International
Serologic surveys conducted worldwide demonstrate CMV to be a ubiquitous infection of humans. Depending on the population surveyed, CMV may be found in more than 90% of people, depending on socioeconomic conditions.
Mortality/Morbidity
CMV seldom is associated with mortality in nonimmunocompromised hosts (< 1%). Substantial morbidity may occur in patients with a mononucleosis syndrome, as described in Adult Cytomegalovirus Infection in the Immunocompetent Host.
In both solid organ and marrow transplant recipients, CMV causes substantial morbidity and mortality. For example, even with antiviral therapy, the mortality rate in allogeneic marrow transplant recipients with interstitial pneumonia varies from 15-75%.
CMV RNA can be detected in 15% of fetal tissues or placentae, indicating that CMV infection during pregnancy contributes to stillbirths. [35]
Age
CMV prevalence increases with age. Age also has been found to be a risk factor for CMV disease in certain transplant populations.
Prognosis
The prognosis of CMV hepatitis generally is good. Most patients recover completely. Symptoms can persist, usually in the form of fatigue, for several months after primary infection.
CMV pneumonia in marrow transplant recipients once carried a mortality rate higher than 85%. The use of ganciclovir plus high-dose immune globulin for the treatment of CMV pneumonia in allogeneic marrow transplant recipients has lowered the mortality rate to 30-60%.
Because patients who develop CMV disease are immunocompromised, their prognosis may be determined by their underlying disease. The need for mechanical ventilation is a poor prognostic sign.
Patient Education
For excellent patient education resources, visit eMedicineHealth's patient education article Mononucleosis.
-
Here, using immunofluorescent technique, a specimen of human embryonic lung (25X) reveals the presence of cytomegalovirus. Courtesy of the CDC and Dr Craig Lyerla.
-
Hematoxylin-eosin–stained lung section showing typical owl-eye inclusions (480X). Courtesy of Danny L Wiedbrauk, PhD, Scientific Director, Virology & Molecular Biology, Warde Medical Laboratory, Ann Arbor, Michigan.
Tables

What would you like to print?


 15 Fingernail and Toenail Abnormalities
15 Fingernail and Toenail Abnormalities


