Practice Essentials
A complex partial seizure, now known as a focal impaired awareness seizure according to the updated classification system from the International League Against Epilepsy (ILAE), [1] starts focally within the brain and causes impairment of consciousness. In most patients, focal impaired awareness seizures represent underlying temporal lobe epilepsy. See the image below.
Signs and symptoms
Focal impaired awareness seizures typically last 30 seconds to 2 minutes. Longer seizures may occur when seizures become generalized with full-body convulsions or transform to a state of partial status epilepticus.
Aura
-
Typically of brief duration, rarely lasting longer than seconds
-
Eight different varieties are recognized: somatosensory, visual, auditory, gustatory, olfactory, autonomic, abdominal, and psychic
-
Auras precede temporal lobe seizures in approximately 80% of cases; the most common are abdominal (a rising epigastric sensation) and psychic (fear, déjà vu, jamais vu)
-
Parietal lobe seizures may begin with a contralateral sensation, usually of the positive type (electrical sensation, tingling)
-
Occipital lobe seizures may begin with contralateral visual changes, usually of the positive type (eg, colored lines, spots, or shapes) or a loss of vision
-
Temporal-parietal-occipital seizures may produce more formed auras
Impaired consciousness
-
Usually, during a focal impaired awareness seizure, the patient is unresponsive and does not remember events that occurred
Background
Broadly, seizures may be classified as either generalized or focal. The term “complex partial seizure” was originally defined by the International League Against Epilepsy (ILAE) in 1981. In 2017, the ILAE updated its seizure classification system and complex partial seizures are now known as focal impaired awareness seizures. [1] A focal impaired awareness seizure starts focally within the brain and causes impairment of consciousness. This definition is based on both clinical and electroencephalographic (EEG) data.
On the other hand, seizures may also be described in accordance with a pure semiologic approach that uses patient symptoms alone. Thus, seizures are classified solely on the basis of their predominant symptom type (motor, sensory, etc). (See Clinical Presentation.) This approach relies on clinical data alone and underscores the importance of obtaining an accurate history.
A seizure, in and of itself, does not constitute a diagnosis of epilepsy. Recognizing a seizure is the first step in the workup for a diagnosis of possible epilepsy. A focal impaired awareness seizure is most commonly a manifestation of temporal lobe epilepsy, but the term is so broadly defined (ie, as any focal seizure with impairment of consciousness) that it is very nonspecific. For this reason, many clinicians make a point of distinguishing between temporal and extratemporal complex partial seizures.
For more information, see Epilepsy and Seizures and Simple Partial Seizures.
Pathophysiology
Single-photon emission computed tomography (SPECT) ictal studies show hypoperfusion of the bilateral frontal and parietal association cortex and hyperperfusion of the mediodorsal thalamus and rostral brainstem. Ictal effects on these structures resulting from the spread of epileptic discharges or a transsynaptic mechanism may mediate impaired consciousness during complex partial seizures. [18]
In most patients, focal impaired awareness seizures are representative of underlying temporal lobe epilepsy. Over time, patients with temporal lobe epilepsy have increased neuroexcitability within the mesial temporal lobes. Pathologic studies suggest focal changes that include neuronal loss, [19] reorganization, neurogenesis, and altered neurotransmitter receptors.
Etiology
In the majority of cases, focal impaired awareness seizures are of unknown etiology (ie, cryptogenic). Potential causes include the following:
-
Hippocampal sclerosis (mesial temporal lobe)
-
Neoplasms
-
Cortical malformations
-
Vascular malformations
-
Central nervous system (CNS) infections
-
Immune-mediated CNS inflammation
-
Hypoxic-ischemic brain injury
-
Head trauma
-
Inheritable conditions
Febrile seizures, especially complex, are associated with an increased risk of later development of complex partial seizures and epilepsy. [20]
Epidemiology
The prevalence of epilepsy is approximately 0.5–1 case per 100 persons. [21] Focal impaired awareness seizures occur in about 35% of persons with epilepsy. Partial seizures are more common in countries where cysticercosis is prevalent.
The incidence of partial seizures, now called focal aware seizures [1] , in people younger than 60 years is 20 cases per 100,000 person-years. This figure rises to 80 cases per 100,000 person-years in people aged 60–80 years.
Prognosis
The mortality rate in individuals with epilepsy is 2-3 times that in the general population. [22] Most deaths are due to the underlying cause (ie, epilepsy) with the remainder due to accidents, sudden unexpected death in epilepsy (SUDEP), and suicides. SUDEP has no apparent cause. It occurs in 1 in 2500 persons with mild epilepsy and 1 in 250 persons with severe epilepsy. SUDEP is most common among those with frequent or medically intractable seizures. [23]
Individuals with epilepsy are at increased risk for trauma, burns, and aspiration.
-
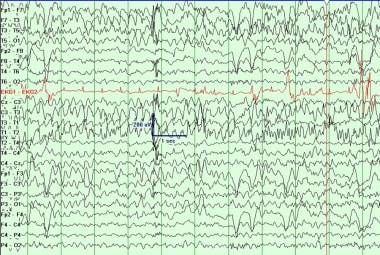
Note oral and hand automatisms at initiation of event. Patient is not following commands or answering questions during the event.
-
Left temporal sharp wave.
-
Left temporal lobe seizure.






