Background
Fungal keratitis was first described by Leber in 1879. [1] This entity is a very common cause of corneal infection in developing countries, although it is not common in Western countries. If not diagnosed and treated promptly and effectively, significant damage can occur. [2]






Keratitis is a general term meaning any inflammation of the cornea. The term fungal keratitis refers to a corneal infection caused by fungi. One type of fungus that can infect the cornea is Fusarium. When Fusarium infects the cornea, the eye disease is referred to as Fusarium keratitis. [1, 2]
The early stage of fungal keratitis remains a diagnostic and therapeutic challenge to the ophthalmologist. [1] There is difficulty in establishing the clinical diagnosis, isolating the etiologic fungal organism in the laboratory, and treating the keratitis effectively with topical antifungal agents. Unfortunately, delayed diagnosis is common, primarily because of lack of suspicion. When a diagnosis has been made, management remains a challenge because of the poor corneal penetration of antifungal agents.
The incidence of fungal keratitis has increased over the past 30 years. [1] This increased occurrence of fungal keratitis is a result of the frequent use of topical corticosteroids along with antibacterial agents in treating patients with keratitis. With better laboratory facilities, the awareness about fungal keratitis has increased.
Classification
Of the 70 different fungi that have been implicated as causing fungal keratitis, the 2 medically important groups responsible for corneal infection are yeast and filamentous fungi (septate and nonseptate).
Yeast produces characteristic creamy, opaque, pasty colonies on the surface of culture media. Candida is the most representative pathogen in this group, primarily affecting those corneas already compromised by topical steroids, surface pathology, or both.
A feathery or powdery growth on the surface of culture media is produced by septate filamentary fungi, which are the most common cause of fungal keratitis.
Fluid movement in the cornea
For the past 15 years, the author (Singh) has been studying the possibility of fluid channels existing in the cornea. Some of the observations are summarized below.
The channels in the cornea are normally invisible. However, if it becomes semiopaque for some reason, the channels tend to stand out.
The question arises as to where the corneal network of channels ends. It joins a peripheral circular corneal channel, which is present in every eye, but becomes visible as a transparent line in all cases of arcus senilis. It is the “lucid interval,” which actually is a canal, the canal of Singh. The corneal network joins canal of Singh in multiple layers all around the limbus.
If cases of arcus senilis are studied regularly with optical coherence tomography, the Singh canal and Schlemm canal will be visualized as being connected through ”aqueducts.” The corneal channel structure helps to understand and explain many observations in corneal infections.
Pathophysiology
Many fungal organisms associated with ocular infections are ubiquitous, saprophytic organisms and have been reported as causes of infection only in the ophthalmic literature. Fungal isolates have been classified into the following groups: Moniliaceae (nonpigmented filamentary fungi, including Fusarium and Aspergillus species), Dematiaceae (pigmented filamentary fungi, including Curvularia and Lasiodiplodia species), and yeasts (including Candida species). [2]
Corneal trauma is the most frequent and major risk factor for fungal keratitis. In fact, the physician should have a high level of suspicion in a patient with a history of corneal trauma, particularly with plant or soil matter. Fungi gain access into the corneal stroma through a defect in the epithelium, then multiply and cause tissue necrosis and an inflammatory reaction. The epithelial defect usually results from trauma (eg, contact lens wear, foreign material, prior corneal surgery). The organisms can penetrate an intact Descemet membrane and gain access into the anterior chamber or the posterior segment. Mycotoxins and proteolytic enzymes augment the tissue damage.
Fungal keratitis also has been described to occur secondary to fungal endophthalmitis. In these cases, fungal organisms extend from the posterior segment through the Descemet membrane and into the corneal stroma. Another possibility is entry through corneoscleral trabeculae in to the many channels in the cornea that exist as a network.
In the advanced countries of the West, fungi are not a common cause of microbial keratitis. However, in the developing countries, fungal infections are extremely common. Farm injuries are the most important cause. Fungi cannot penetrate the intact corneal epithelium. They need a penetrating injury or a previous epithelial defect to enter the cornea. Once within the cornea, however, they are able to proliferate and spread through the corneal channels.
Organisms that infect preexisting epithelial defects belong to the normal microflora of the conjunctiva and adnexa. The most common pathogen that invades a preexisting epithelial defect is Candida. Filamentous fungi are the principal causes of posttraumatic infection. The intrinsic virulence of fungi depends on the fungal substances produced and the host response generated.
Filamentous fungi proliferate within the corneal stroma without release of chemotactic substances, thereby delaying the host immune/inflammatory response. In contrast, Candidaalbicans produces phospholipase A and lysophospholipase on the surface of blastospores, facilitating the entrance to the tissue. Fusariumsolani, which is a virulent fungus, is able (as are other filamentous fungi), to spread within the corneal stroma and penetrate the Descemet membrane.
The trauma that accompanies contact lens wear is miniscule; contact lenses are not a common risk factor for fungal keratitis. Candida is the principal cause of keratitis associated with therapeutic contact lenses, and filamentous fungi are associated with refractive contact lens wear. Photorefractive keratectomy and laser in-situ keratomileusis (LASIK) cases, on a rare occasion, can develop fungal infection, which may result in severe damage to the cornea, even loss of an eye. Infections may develop in a series of patients if an infected fluid is used in a number of patients at one session.
Topical steroid use has definitively been implicated as a cause of increased incidence, development, and worsening of fungal keratitis. Other risk factors to consider are foreign bodies and immunosuppressive diseases.
Epidemiology
Frequency
Worldwide
In 2021, Brown et al published a systematic literature review on the epidemiology of fungal keratitis. They searched papers from Jan 1, 1946, to July 26, 2019. They could estimate that a minimum of 1 million cases of fungal keratitis occur every year, and this number rises to over 1.4 million if negative cultures are assumed to be fungal. They also found that the highest ratio of fungi vs bacteria occurs in subtropical and tropical countries, predominantly in male agricultural workers. [3]
Sharma et al published a recent review with the findings of the newest studies about prevalence in cultures in fungal keratitis. There were data from India, Nepal, Saudi Arabia, Japan, USA, Thailand, Turkey, Brazil, Australia and Iran. They found 8 studies with higher prevalence of Fusarium worldwide. But, when comparing studies from India, Bangladesh and Saudi Arabia Aspergillus was the most common organism. Candida was the most common fungi found in cultures Japan. [4]
United States
The incidence of fungal keratitis varies according to geographic location and ranges from 2% of keratitis cases in New York to 35% in warm weather Florida. Fusarium species are the most common cause of fungal corneal infection in the southern United States (45-76% of fungal keratitis), whereas Candida and Aspergillus species are more common in northern states.
In a large series of fungal keratitis from south Florida, Rosa et al reported that Fusarium oxysporum was the most common isolate (37%), followed by, in order of decreasing frequency, Fusarium solani (24%), Candida, Curvularia, and Aspergillus species. [5, 6]
Fusarium species are commonly found in soil, in water, and on plants throughout the world, particularly in warmer climates. Past studies of Fusarium keratitis have found that most incidences of Fusarium keratitis have been caused by an eye injury with vegetative matter (eg, being hit in the eye with a palm branch).
A number of individuals have contracted Fusarium keratitis from contact lens wear, especially through the use of the Bausch & Lomb ReNu with Moisture Lock contact lens solution. This number is generally very small, particularly in the northern part of the United States.
On March 8, 2006, the Centers for Disease Control and Prevention (CDC) received a report from an ophthalmologist in New Jersey regarding 3 patients with contact lens-associated Fusarium keratitis during recent months. Initial contact with several corneal disease specialty centers in the United States revealed that other centers also had seen recent increases in Fusarium keratitis.
The CDC began an investigation of the Fusarium keratitis outbreak. There were 130 confirmed cases of Fusarium keratitis. Over 60% of people with confirmed Fusarium keratitis had used Bausch & Lomb ReNu with Moisture Lock contact lens solution, and 37 of these cases resulted in cornea transplant surgery.
The US Food and Drug Administration (FDA) recalled Bausch & Lomb ReNu with Moisture Lock contact lens solution.
According to Bausch & Lomb, "unique characteristics of the formulation of the ReNu with Moisture Lock product in certain unusual circumstances can increase the risk of Fusarium infection."
Mortality/Morbidity
Fungal organisms can extend from the cornea into the sclera and intraocular structures. Fungi can cause severe infections, such as scleritis, endophthalmitis, or panophthalmitis. These infections usually are very difficult to treat and may result in severe visual loss or even loss of the eye.
Sex
Fungal keratitis is more common in males than in females and often occurs in patients with a history of outdoor ocular trauma.
Prognosis
Prognosis depends on several factors, including the extent of corneal involvement upon presentation, the patient's health status (eg, immunocompromised), and the timing of establishing a clinical diagnosis confirmed by culture in the laboratory.
Patients with mild infections and an early microbiologic diagnosis have a good prognosis; however, controlling or eradicating an infection that spreads into the sclera or the intraocular structures is very difficult.
Approximately one third of fungal infections result in either medical treatment failure or corneal perforation.
Patient Education
Patients who wear contact lenses should consult their eye care professional concerning use of an appropriate cleaning/disinfecting product. (Patients should discontinue use of Bausch & Lomb ReNu with Moisture Lock contact lens solution.)
Patients should consider performing a “rub and rinse” lens cleaning method, rather than a no rub method, regardless of which cleaning/disinfecting solution used, in order to minimize the number of germs and to reduce the chances of infection.
Patients should continue to follow proper lens care practices. Wash their hands with soap and water and dry (lint-free method) them before handling lenses. Wear and replace lenses according to the schedule prescribed by their eye care professional. Follow the specific lens cleaning and storage guidelines from their eye care professional and the solution manufacturer. Keep the contact lens case clean and replace every 3-6 months.
Patients should remove the lenses and consult their eye care professional immediately if they experience symptoms, such as redness, pain, tearing, increased light sensitivity, blurry vision, discharge, or swelling.
-
Fungal corneal ulcer.
-
Perforated fungal ulcer.
-
Fungal infection under treatment.
-
Perforated fungal corneal ulcer.
-
Fungal ulcer in an elderly woman.
-
Fungal ulcer.
-
Fungal corneal ulcer, with excessive vascularization.
-
Marginal ulcer, fungus positive.
-
Healed fungal ulcer.
-
Fungal keratitis.
-
Corneal perforation, blocked by a crystalline lens and being covered by epithelium.
-
Fungal keratitis, being controlled.
-
Fungal infection.
-
Fungal infection.
-
Fungal abscess.
-
Fungal corneal abscess/ulcer. A proven case of fungal infection, 5 days' duration. Intense infiltration around the abscess.
-
Surgical trauma producing edema and striate keratitis. The corneal channels stand out in semiopaque corneal tissue, since they themselves are no-tissue spaces.
-
Surgical trauma producing edema and striate keratitis. The corneal channels stand out in semiopaque corneal tissue, since they themselves are no-tissue spaces.
-
A network of channels is visible in a case of megalocornea with faint opacification of stroma. The channels stand out as nonstructures.
-
This kind of opacification is termed keratitis. Anatomically, it appears to be a microchannel structure.
-
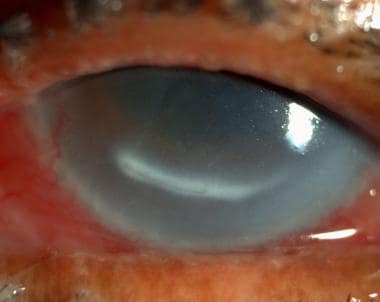
A network of corneal channels stands out inside the arcus senilis of an old patient. Whatever causes the opacification in the corneal tissue is not able to opacify the emptiness of corneal channels.
-
Network of corneal channels in a 92-year-old patient.
-
The corneal channels open in the lucid interval channel of Singh.
-
Peripheral corneal channel network and canal of Singh in 3 dimensions.
-
Optical section of corneal channels in a case of arcus senilis.
-
The lucid interval in optical section clearly shows its triangular configuration and an anterior and posterior wall. The apex continues towards corneal channels in the stroma. The lucid interval channel is connected to limbal lymphatics.
-
The lucid interval channel is connected to the lymphatics at the limbus and the corneal channels centrally.
-
A blunt wire of 100 micrometers diameter has been pushed into the canal of Singh.
-
A 230-micrometer blunt cannula in the canal of Singh.
-
This networklike pattern of fungal corneal infection is explained only by the preferential path of spread through the corneal channel network.
-
The fungal infection travels in various directions. Also seen are satellite lesions. Satellite lesions and other appearances are explained by the presence of channels in the cornea.
-
Notice centrifugal, linear, circular, and satellitelike spread of fungal infection through the corneal channels.
-
This patient presented with infection of the lucid interval of Singh without any evidence of corneal ulceration as a starting point, suggesting systemic spread. A satellite of infection is seen near the 6-o'clock position.
-
Same patient with infection of the lucid interval of Singh without any evidence of corneal ulceration as a starting point, suggesting systemic spread. A big and a small satellite at the 6-o'clock position.
-
The same eye showing the spread of fungal infection on the nasal side of the Singh canal. This patient showed no evidence of corneal injury, thus a systemic origin of infection is a distinct possibility.
-
The whole of the infected lucid interval canal of Singh was opened. The scraping showed the presence of hyphae. The patient was treated by oral medication, local drops, and intracorneal antifungal voriconazole injections. Final vision was 6/6 uncorrected. There was no recurrence.
-
Optical coherence tomography scans clearly showing the canal of Singh connected to the Schlemm canal.
-
Optical coherence tomography scans clearly showing the canal of Singh connected to the Schlemm canal.
-
Fungal keratitis under treatment. The infection has spread into the nearby lucid interval canal of Singh.
-
The same case as in the previous photo. Optical coherence tomography scans shows the presence of exudates in the lucid interval canal of Singh and the adjoining trabecular meshwork.
