Practice Essentials
A claw toe is a lesser toe with dorsiflexion of the proximal phalanx on the lesser metatarsophalangeal (MTP) joint and concurrent flexion of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints (see the images below).


The term claw toe is most likely derived from the affected toe's similarity in appearance to the claw of an animal or talon of a bird (see the image below). The talon typically curves upward before it makes a descending C-shaped curve.

Claw toe is distinguished from hammer toe by the combination of dorsiflexion of the MTP joint and plantarflexion of the DIP joint in the former condition (see the image below). In contrast, a hammer toe may have some hyperextension at the MTP joint or some flexion at the DIP joint, but it does not have both concurrently. Typically, the DIP joint is extended in a hammer toe.

Hammer toe is differentiated from curly toe, which has combined plantarflexion of all three joints (see the first image below), as well as from mallet toe, which has a neutral position of the MTP and PIP joints and flexion at the DIP joint (see the second and third images below). Clawing often affects multiple toes (see the fourth image below). [1, 2, 3]




Table 1 contains descriptions of lesser toe deformities.
Table 1. Lesser Toe Deformities (Open Table in a new window)
Deformity |
MTP Joint |
PIP Joint |
DIP Joint |
Hammer toe |
Dorsiflexed* or neutral |
Plantarflexed |
Neutral, hyperextended, or plantarflexed* |
Claw toe |
Dorsiflexed |
Plantarflexed |
Plantarflexed |
Mallet toe |
Neutral |
Neutral |
Plantarflexed |
Curly toe |
Neutral or plantarflexed |
Plantarflexed (>5°) |
Plantarflexed (>5°) |
*Cannot coexist |
|||
Indications for treatment are those presentations that produce pain (see Presentation). Contraindications for operative treatment include poor vascularity to the toe (including vascular problems that could lead to ischemia and possible need for amputation following surgery, such as diabetes or atherosclerosis) and poor skin quality. An open infected wound should also be resolved prior to surgery.
Pharmacologic treatment for claw toes may be appropriate, depending on the underlying cause; however, such treatments are not believed to reverse the claw toe position. Conservative therapy (including footwear changes and use of a metatarsal bar or padding) may be helpful.
Various operative procedures are available for treatment of a claw toe. (See Treatment.) When to perform each of the procedures and the extent of the surgical procedure on a single toe, and other aspects of operative treatment remain controversial. Minimally invasive (percutaneous) approaches to treatment of lesser-toe deformities such as claw toe have been developed and are associated with high correction potential and low complication rates. [4]
Pathophysiology
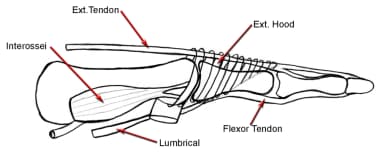
The extensor tendon crosses and is held over the MTP joint by an aponeurotic band of fibrous tissue. Although it does not insert into the proximal phalanx, it is able to dorsiflex the proximal phalanx of the MTP joint through this aponeurotic band, which goes around the MTP joint and is inserted onto the plantar plate (see the image below).
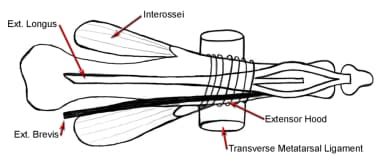
The extensor tendon splits into three parts over the proximal phalanx. The central slip attaches itself to the dorsal aspect of the base of the middle phalanx. The medial and lateral slips rejoin distally to insert on the dorsal aspect of the base of the distal phalanx (see the image below). The extensor tendon is only capable of extending the PIP and DIP joints when the MTP joint is in neutral flexion; otherwise, this is accomplished by the intrinsic musculature. [5, 6, 7, 8]
The intrinsics are made of the lumbricals, which are strong extenders of the PIP and DIP joints by virtue of their attachment onto the extensor sling and the interossei. Interossei are weak extensors of the interphalangeal (IP) joints because so few fibers reach the extensor sling. Furthermore, when the MTP joint is hyperextended, the lumbrical power in extending the PIP and DIP joints is reduced because of a mechanical disadvantage.
The flexor digitorum longus (FDL) tendon inserts into the plantar aspect of the distal phalanx, and the flexor digitorum brevis (FDB) inserts onto the middle phalanx. Thus, no major antagonist to dorsiflexion of the proximal phalanx is present. Hence, when the proximal phalanx dorsiflexes, static tightening of the flexors occurs, which subsequently flexes the PIP and DIP joints. Stabilization of the lesser MTP joint comes from the static restraint of the plantar plate and the collateral ligaments.
The collateral ligaments have been reported as the primary stabilizers of the lesser MTP joint. The two sets of collateral ligaments both emanate from the lateral metatarsal head. The phalangeal collateral ligament inserts into the proximal phalanx, and the accessory collateral ligament inserts onto the plantar plate. The plantar plate is attached from the base of the proximal phalanx to an origin on the metatarsal head, just proximal to the plantar articular cartilage.
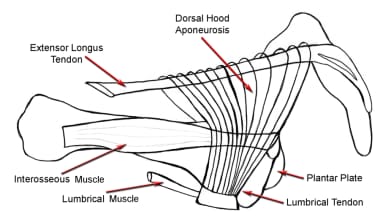
When the collateral ligaments and plantar plate lose resiliency or are stretched through repetitive dorsal directing forces on the proximal phalanx from ground reactive forces, the proximal phalanx dorsiflexes. Without a strong plantar flexor attached to the proximal phalanx, the proximal phalanx remains in dorsiflexion, and the PIP and DIP joints subsequently flex (see the image below).
When the flexed position of the PIP and DIP joints remains constant, the collateral ligaments fibrose along the sides of the PIP and DIP joints, and the position of their joints becomes fixed. When this occurs, the claw toe deformity becomes rigid, whereas previously it was considered flexible. This separation of flexible and rigid most often occurs at the PIP joint.
Etiology
Claw toe deformity results from altered anatomy or neurologic deficit that leads to an imbalance between the intrinsic and extrinsic musculature to the toes. [9, 10]
Epidemiology
The prevalence of claw and hammer toe deformities is in the range of 2-20%, gradually increasing with advancing age. Accordingly, claw toe is most often seen in patients in the seventh and eighth decades of life. Women are affected four to five times more than men are. Little is mentioned in the literature regarding these deformities in non-shoe-wearing populations. [11, 12, 13, 14]
Most people have no underlying disease responsible for the claw toe deformity, but it can occur in association with neuromuscular diseases, such as multiple sclerosis, Friedreich ataxia, Charcot-Marie-Tooth disease, cerebral palsy, mild dysplasia, stroke, and lumbar nerve-root impingement. Metabolic diseases such as diabetes and inflammatory arthropathies such as rheumatoid arthritis and psoriasis can also be accompanied by claw toe deformity.
Prognosis
The experiences of other authors indicate that complete correction of the toe is necessary to achieve the best result. Of course, this presumes careful attention to detail and a toe with normal vascularity.
Taylor [15] and Pyper, [16] via transfer of both the long and the short flexor to the extensor hood without bony resection, achieved only 72% and 51% good results, respectively. Pyper also noted that with soft-tissue procedures alone, the deformity recurred and results were somewhat unpredictable. [16] Therefore, Frank et al [17] and McCluskey et al [18] recommended PIP resection along with soft-tissue procedures to realign the toe.
Barbari et al [19] reviewed 31 patients who had surgery on multiple toes. These authors concluded that the best cosmetic results were achieved in younger patients, and they noted that active or passive motion in the IP joints was present in 60% of these cases. Of course, restriction in range of motion (ROM) is an intended outcome of the procedure. Patients must be aware that in most instances, they will sacrifice prehensile action of the toe for less pain, will have better shoe-wearing capabilities, and, ideally, will have an improved cosmetic result.
Specific disease entities seem to fare similarly; Cyphers et al [20] reported 60% good results in patients with myelomeningocele.
A prospective multicenter observational study of 117 patients requiring PIP joint realignment who underwent placement of angled intramedullary implants found that implantation resulted in a high rate of fusion and a good outcome. [21] None of the patients with incomplete joint fusion who had a stable joint with no pain required reoperation.
-
Claw toe is named for its similarity to animal claw or talon.
-
Claw toe.
-
Plastic model of claw toe.
-
Hammer toe.
-
Plastic model of hammer toe.
-
Curly toe.
-
Mallet toes 3 and 4.
-
Mallet toe.
-
Multiple claw toes.
-
Claw toe. Extensor tendon connecting with extensor hood.
-
Claw toe. Extensor tendon splits into 3 parts distally.
-
Claw toe. Plantar plate stretches out, and proximal phalanx is dorsiflexed.
-
Callus at tip of second claw toe.
-
Pad beneath multiple claw toes to reduce pressure at tips.
-
Claw toe. Silicone cap on second toe and sleeve on third toe, with sleeve reversed to show silicone inside.
-
Claw toe. Extensor tendon exposure.
-
Claw toe. Z lengthening of extensor tendon.
-
Claw toe. Capsulotomy.
-
Claw toe. Collateral ligament release.
-
Claw toe. Repaired extensor tendon.
-
Claw toe. Make longitudinal incision across the plantar metatarsophalangeal joint.
-
Claw toe. Split tendon sheath to expose flexor tendons.
-
Claw toe. Isolate flexor digitorum longus tendon from flexor digitorum brevis, and place it under tension.
-
Claw toe. Cut flexor digitorum longus tendon just proximal to its attachment.
-
Claw toe. Pull flexor digitorum longus tendon loose from its attachment.
-
Claw toe. Separate 2 raphes of the flexor digitorum longus tendon.
-
Claw toe. Grasp each side (raphe) of flexor digitorum longus tendon with small hemostat.
-
Claw toe. Make dorsal incision to grasp flexor digitorum longus tendon.
-
Claw toe. Through dorsal incision, curve hemostat around proximal phalanx, avoiding neurovascular bundle, and grasp tip of same-side flexor digitorum longus tendon.
-
Claw toe. Repair each end of raphe to other raphe and split extensor tendon.
-
Final repair of claw toe.
-
Multiple repaired claw toes; Kirschner wires added for stability.
-
Claw toe. Elliptical outline of skin incision.
-
Claw toe. Redundant skin being excised.
-
Claw toe. Isolate distal portion of proximal phalanx.
-
Claw toe. Remove distal portion of proximal phalanx.
-
Claw toe. Feather edges of proximal phalanx to ensure no prominent edges.
-
Claw toe. Remove articular cartilage of middle phalanx.
-
Claw toe. Drill pin retrograde from middle phalanx out of tip of toe.
-
Claw toe. After pin has been drilled back into proximal phalanx and metatarsal head, repair skin and extensor tendon over proximal interphalangeal joint.
-
Claw toe. Bent pin at end of toe; proximal incision has been used for Z-lengthening of extensor tendon.
-
Claw toe. Dorsal approach to proximal interphalangeal joint and extensor tendon.
-
Claw toe. Z-lengthened extensor tendon with end of proximal phalanx exposed.
-
Claw toe. Remove distal portion of proximal phalanx.
-
Claw toe. Grasp end of proximal phalanx for removal.
-
Claw toe. Remove articular cartilage of middle phalanx.
-
Claw toe. Bone ends of proximal interphalangeal joint.
-
Claw toe. Place wire in middle of proximal phalanx.
-
Claw toe. Drill wire out of tip of toe, then back through proximal phalanx and metatarsal head.
-
Claw toe. Toe in straightened position, with dorsal incision used to expose dorsal metatarsophalangeal capsule for release.
-
Claw toe. Algorithm to determine appropriate surgical procedure and postoperative treatment.
-
Claw toe. Video shows flexor-to-extensor tendon transfer with extensor Z-lengthening tenotomy and dorsal capsular release in 54-year-old man with multiple claw toes following brain injury. Toe is pinned with 0.54-mm Kirschner wire just prior to transferring tendon dorsally (not shown in video). Remaining lesser toes, 2 and 4, underwent identical procedure after this video was made. In addition, fifth toe had flexor digitorum longus release with extensor tendon lengthening, and great toe underwent interphalangeal fusion with extensor hallucis longus Z-lengthening.
-
"Sausage toe" complication after Girdlestone-Taylor tendon transfer.
Tables
Deformity |
MTP Joint |
PIP Joint |
DIP Joint |
Hammer toe |
Dorsiflexed* or neutral |
Plantarflexed |
Neutral, hyperextended, or plantarflexed* |
Claw toe |
Dorsiflexed |
Plantarflexed |
Plantarflexed |
Mallet toe |
Neutral |
Neutral |
Plantarflexed |
Curly toe |
Neutral or plantarflexed |
Plantarflexed (>5°) |
Plantarflexed (>5°) |
*Cannot coexist |
|||





