Practice Essentials
Pyogenic granulomas (PGs) are benign vascular lesions that occur most commonly on the acral skin of children. [1, 2] The term pyogenic granuloma is a misnomer. Originally, these lesions were thought to be caused by bacterial infection; however, the etiology has not been determined. The histopathologic appearance is fairly characteristic; the lesion is, in fact, a lobular capillary hemangioma. [3]
Recognition of pyogenic granuloma as a clinically polypoid or exophytic circumscribed lesion is of importance to the clinician and pathologist because this feature distinguishes pyogenic granulomas from most malignant vascular tumors. Although pyogenic granulomas may be multiple (especially on the skin) and necrosis is common, invasion of adjacent structures is not observed. The lesions grow rapidly and are extremely vascular, frequently bleeding either spontaneously or after minor trauma. [4] They are usually easily treated with surgical removal but may recur.
Uncommon variants include pyogenic granuloma with satellitosis, [5, 6, 7] intravenous pyogenic granulomas, [8] subcutaneous pyogenic granulomas, [9, 10] and eruptive pyogenic granulomas. [11, 12, 13] Satellite lesions of smaller pyogenic granulomas may develop at the same time as the primary lesion or may occur after attempted treatment of the primary lesion. See the images below.
 Pyogenic granulomas are usually solitary lesions. The fingers and hands are common locations for these to develop. A history of minor trauma at the site shortly before development of the lesion is frequent.
Pyogenic granulomas are usually solitary lesions. The fingers and hands are common locations for these to develop. A history of minor trauma at the site shortly before development of the lesion is frequent.
 Pyogenic granulomas usually bleed with little or no trauma. This patient shows a positive bandage sign. Because the lesions bleed so easily, patients frequently present with a bandage covering the site.
Pyogenic granulomas usually bleed with little or no trauma. This patient shows a positive bandage sign. Because the lesions bleed so easily, patients frequently present with a bandage covering the site.
 Pyogenic granulomas usually have a distinct margin that consists of a rim of keratin (dry skin). Notice the moist area of skin produced by the bandage, which was removed shortly before the photograph was taken.
Pyogenic granulomas usually have a distinct margin that consists of a rim of keratin (dry skin). Notice the moist area of skin produced by the bandage, which was removed shortly before the photograph was taken.
 Pyogenic granulomas may be pedunculated and quite large. An area of necrosis is also common.
Pyogenic granulomas may be pedunculated and quite large. An area of necrosis is also common.
 Pyogenic granulomas may occur at various sites. More than 60% of all lesions develop on the head and neck.
Pyogenic granulomas may occur at various sites. More than 60% of all lesions develop on the head and neck.

Signs and symptoms
See Presentation for a full discussion.
Pyogenic granulomas (PGs) appear as smooth firm nodules, with or without crusts, and they may have a bright or dusky red color. They are usually solitary, well circumscribed, dome shaped, 1-10 mm in diameter, and sessile or pedunculated.
In children, pyogenic granulomas are most commonly located on the head and neck (62.4%) and, in order of decreasing frequency, on the trunk (19.7%), upper extremity (12.9%), and lower extremity (5%). Most (88.2%) occur on the skin, and the rest involve mucous membranes of the oral cavity and conjunctivae.
In pregnant women, pyogenic granulomas are most often found on the gingival mucosa [14, 15] but they have been known to appear in nonoral areas such as the fingers and inguinal crease.
Pyogenic granulomas may occur within a port-wine stain; the presence of a vascular birthmark in the region of the pyogenic granuloma may be significant.
Amelanotic melanoma may closely mimic a pyogenic granuloma in appearance. Closely examine the skin immediately adjacent to the lesion for any pigmentary irregularity.
Diagnostics
Lesions that do not respond appropriately to conservative treatment should undergo biopsy to confirm the diagnosis.
Proliferation of capillaries is present, with prominent endothelial cells embedded in edematous gelatinous stroma in a characteristic lobular configuration (see image below).
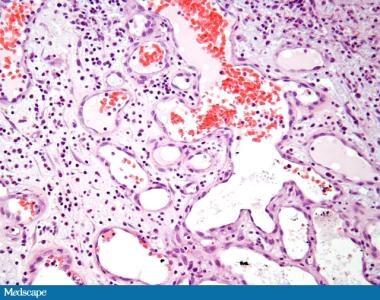 Histologic image showing epidermal erosion and crusting, thinned epidermis, vascular proliferation, and mixed inflammation with lymphocytes, histiocytes, and neutrophils. Courtesy of Medscape Dermatology.
Histologic image showing epidermal erosion and crusting, thinned epidermis, vascular proliferation, and mixed inflammation with lymphocytes, histiocytes, and neutrophils. Courtesy of Medscape Dermatology.
The epidermis is commonly eroded.
A dense infiltrate and granulation tissue with polymorphonuclear leukocytes may be present.
Hyperproliferation of the epidermis is usually present at the margins of the vascular growth, which results in a collarette of epidermis. [16, 17, 18]
Management
Please see Treatment.
Pathophysiology
Although most patients (74.2%) do not have a history of trauma or predisposing dermatologic conditions, in many cases, a history of recent trauma at the site is present. Large numbers of lesions may occur following damage to diffuse areas skin by burns or other trauma. [19, 20] A nitric oxide synthase–dependent mechanism is thought to contribute to angiogenesis and the rapid growth of pyogenic granulomas (PGs). They are benign vascular proliferations, but the specific pathophysiology of these lesions is unknown.
Etiology
Originally, pyogenic granulomas (PGs) were thought to be caused by bacterial infection; the etiology has yet to be determined. Postulated etiologies include viral, hormonal, and, more recently, angiogenic factors.
Pyogenic granulomas have been evaluated for the presence of human papillomavirus (HPV) because warts occur in similar age groups and sites. Lesions were tested for HPV 6, 11, 16, 31, 33, 35, 42, and 58. No viruses were present.
Recurrent pyogenic granuloma with satellitosis is an uncommon variant. In one patient with recurrent pyogenic granuloma with satellitosis, Warthin-Starry staining of the lesions revealed clumps of dark bacilli as found in patients with bacillary angiomatosis. [5] An indirect immunofluorescence assay showed elevated immunoglobulin G antibodies against Bartonella (Rochalimaea) henselae. The patient did not present an obvious risk for human immunodeficiency virus (HIV) infection or immunosuppression; no antibodies against HIV-1 and HIV-2 were found. Recurrent pyogenic granulomas with satellitosis may be a localized variant of bacillary angiomatosis.
There have been cases of pyogenic granuloma induced by ibrutinib in adults, although the exact pathogenesis is unknown. [21]
Epidemiology
US frequency
Pyogenic granulomas (PGs) account for 0.5% of skin lesions in infants and children and are also found in the oral mucosa in 2% of pregnant women.
Race-, sex-, and age-related information
No substantial difference in incidence is found between races.
One study of 178 patients younger than 17 years reported the male-to-female ratio as 3:2. [16] In adults, pyogenic granulomas are more common in females because of pregnancy-related lesions.
Pyogenic granulomas are most common in the first 5 years of life. [22]
Prognosis
Prognosis is excellent after simple removal and wound care. Most pyogenic granulomas (PGs) are asymptomatic except for mild tenderness and a tendency to bleed with little or no trauma. They are benign and easily treated. Rarely, pyogenic granulomas in unusual sites such as the intestines may result in significant bleeding [23, 24, 25] or other major complications. [26]
-
Pyogenic granulomas are usually solitary lesions. The fingers and hands are common locations for these to develop. A history of minor trauma at the site shortly before development of the lesion is frequent.
-
Pyogenic granulomas usually bleed with little or no trauma. This patient shows a positive bandage sign. Because the lesions bleed so easily, patients frequently present with a bandage covering the site.
-
Pyogenic granulomas usually have a distinct margin that consists of a rim of keratin (dry skin). Notice the moist area of skin produced by the bandage, which was removed shortly before the photograph was taken.
-
Pyogenic granulomas may be pedunculated and quite large. An area of necrosis is also common.
-
Pyogenic granulomas may occur at various sites. More than 60% of all lesions develop on the head and neck.
-
Unlike pyogenic granulomas, cherry angiomas such as these are slow to develop, do not bleed easily, are frequently multiple, are more commonly found on the trunk, and seldom have a history of prior trauma.
-
Several malignant tumors may mimic pyogenic granulomas. This lesion is a squamous cell carcinoma. Amelanotic melanomas (little or no overt pigment) are also included in the differential diagnosis. These tumors are usually slower growing than pyogenic granulomas and are uncommon in children. Tissue removed as part of the treatment process should be sent for histopathologic examination to confirm the diagnosis.
-
Small pyogenic granuloma.
-
Histologic image showing epidermal erosion and crusting, thinned epidermis, vascular proliferation, and mixed inflammation with lymphocytes, histiocytes, and neutrophils. Courtesy of Medscape Dermatology.
