Practice Essentials
Löffler syndrome is a transient respiratory illness associated with blood eosinophilia and radiographic shadowing. (See the image below.) It was initially described by Löffler in 1932. In 1952, Crofton included Löffler syndrome as one of the 5 categories for conditions that cause pulmonary infiltrates with eosinophilia. The original description of Löffler syndrome listed parasitic infection with Ascaris lumbricoides as its most common cause; however, other parasitic infections and acute hypersensitivity reactions to drugs are included as etiologies for simple pulmonary eosinophilia.
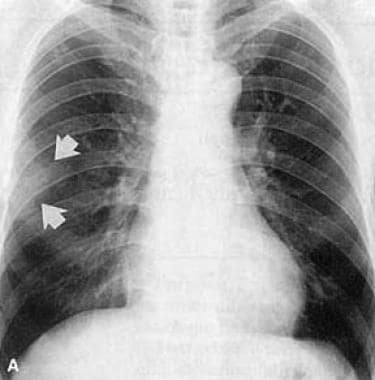 Initial chest radiograph of a 54-year-old man showing subtle opacity (arrows) in the right middle lung zone.
Initial chest radiograph of a 54-year-old man showing subtle opacity (arrows) in the right middle lung zone.
Signs and symptoms
Symptoms of Löffler syndrome are usually mild or absent and tend to spontaneously resolve after several days or, at most, after 2-3 weeks. Cough is the most common symptom among symptomatic patients.
See Presentation for more detail.
Diagnosis
Laboratory studies
The following studies are indicated in Löffler syndrome:
-
Complete blood cell (CBC) count with differential
-
Stool examination
-
Immunoglobulin E (IgE) level
-
Analysis of sputum or gastric lavages
-
Bronchoalveolar lavage
Imaging studies
The following studies may be included in the workup:
-
Chest radiography
-
Chest computed tomography (CT) scanning
See Workup for more detail.
Management
The minimal nature of symptoms in most patients with Löffler syndrome usually denotes that no pharmacologic therapy is required for this self-limiting condition. Surgical
-
Initial chest radiograph of a 54-year-old man showing subtle opacity (arrows) in the right middle lung zone.
-
Follow-up chest radiograph of a 54-year-old man showing migrating opacity in the left lower lobe (arrows) obtained 20 days after the previous image.
-
High-resolution CT scan (1 mm collimation) obtained in a 54-year-old man showing consolidation with surrounding ground-glass opacity in the left lower lobe. Dilated airways are observed within the lesion. This CT scan was obtained between the first and second images above.
