Practice Essentials
Q fever (see the image below) is a zoonosis caused by Coxiella burnetii, an obligate gram-negative intracellular bacterium. Cattle, sheep, and goats are the primary reservoirs, although a variety of species may be infected. Transmission to humans occurs primarily through inhalation of aerosols from contaminated soil or animal waste. Other rare modes of transmission include tick bites, ingestion of unpasteurized milk or dairy products, and human-to-human transmission.
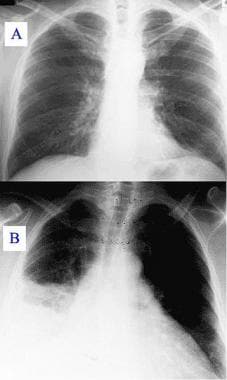 A: Chest radiograph with normal findings. B: Chest radiograph demonstrating Q fever pneumonia.
A: Chest radiograph with normal findings. B: Chest radiograph demonstrating Q fever pneumonia.
Signs and symptoms
Acute Q fever
The 3 main clinical presentations of acute Q fever are as follows:
-
A self-limited, influenzalike febrile illness (up to 40°C) (88-100%) of abrupt onset, which often is accompanied by headache (68-98%) (typically retrobulbar), myalgia (47-69%) (arthralgia is uncommon), chills (68-88%), fatigue (97-100%), and sweats (31-98%); the temperature returns to normal within 5-14 days
-
Pneumonia (predominant in North America), usually mild in nature (crackles auscultated in 50% of cases) or as an incidental radiographic finding; when there is respiratory involvement, patients have a dry, nonproductive cough (24-90%), dyspnea, and pleuritic chest pain; this condition rarely is fulminant but occasionally progresses to acute respiratory distress syndrome (ARDS)
-
Hepatitis (predominant in Europe), usually with mild elevation of transaminases (2-3 times the reference range) and may be associated with antismooth muscle, antiphospholipid, or antinuclear antibodies; jaundice and acute gastrointestinal (GI) symptoms (nausea and vomiting, diarrhea [rare], right upper quadrant abdominal pain) are rare; manifestations resolve within 2-3 weeks.
Background
Q fever is a zoonosis caused by Coxiella burnetii, an obligate gram-negative intracellular bacterium. Most commonly reported in southern France and Australia, Q fever occurs worldwide (except in New Zealand).
C burnetii infects various hosts, including humans, ruminants (cattle, sheep, goats), and pets—and, in rare cases, reptiles, birds, and ticks. This bacterium is excreted in urine, milk, feces, and birth products. These products, especially the latter, contain large numbers of bacteria that become aerosolized after drying. C burnetii is highly infectious, and only a few organisms can cause disease.
Because of its sporelike life cycle, C burnetii can remain viable and virulent for months. Infection can be acquired via inhalation or skin contact, and direct exposure to a ruminant is not necessary for infection. Transmission by tick bite is well recognized but rare. Rare human-to-human transmissions involving exposure to the placenta of an infected woman and blood transfusions have been reported. Sexual transmission also is possible.
C burnetii infection in livestock often goes unnoticed. In humans, acute C burnetii infection often is asymptomatic or mistaken for an influenzalike illness or atypical pneumonia (see the following image). In rare cases, C burnetii infection becomes chronic, with devastating results, especially in patients with preexisting valvular heart disease. Because of its highly infectious nature and an inhalational route of transmission, C burnetii is recognized as a potential agent of bioterrorism. The Centers for Disease Control and Prevention (CDC) classifies Q fever as a Category B agent. [2]
A: Chest radiograph with normal findings. B: Chest radiograph demonstrating Q fever pneumonia.
See also Rickettsial Infection, Pediatric Bacterial Endocarditis, Infective Endocarditis, Community-Acquired Pneumonia, Ticks and Tick-Borne Diseases: Slideshow, and Remaining Vigilant Against Bioterrorism: Slideshow.
Historical information
Edward Derrick first described the illness Q (for query, owing to the elusiveness of its etiology) fever in 1937 during a cluster of acute febrile illness in abattoir workers in Brisbane, Queensland, Australia. [3] The causative organism later was isolated from Derrick's patients by Burnet and Freeman as a Rickettsia species. Simultaneously, although primarily disseminated as an aerosol via inhalation or ingestion, Davis and Cox identified vector transmission when they identified same organism from ticks collected near Nine Mile Creek in Montana during an investigation of Rocky Mountain spotted fever in 1938. First named Rickettsia diaporica and Rickettsia burnetii, the current name of Coxiella burnetii was applied in 1948.
Pathophysiology
As noted earlier, Q fever is a ubiquitous zoonotic disease caused by C burnetii, with protean clinical manifestations that are not fully understood. [4] C burnetii has a worldwide distribution from its reservoirs (including mammals, birds, and ticks), and the development of Q fever is strongly related to exposure to farm animals (primarily cattle, sheep, and goats) and particularly parturient animals (including cats and rabbits) because the organism is reactivated in pregnant animals. In one reported case, an obstetrician developed symptoms of Q fever 1 week after delivering a child to a woman who had Q fever. [5] A characteristic of infection with C burnetii is that only humans regularly express the disease.
Initially classified as a species of the genus Rickettsia because of its obligatory intracellular growth requirements, C burnetii now is recognized as a bacterium within the gamma group of Proteobacteria. Genome and 16SrRNA sequencing have identified substantial homology with Legionella pneumophila, also a member of that taxonomic group.
C burnetii is a strict, intracellular, pleomorphic, gram-negative coccobacillus with an incubation period of 9-40 days; the average incubation period is 20 days (range, 18-21 d). Q fever is primarily transmitted by: (1) aerosolization from newborn animals, their placentas, [6] and contaminated hides and fur; (2) ingestion of raw milk and goat cheese; (3) transfusions of blood products; (4) mother to offspring (ie, vertical) transmission; and (5) tick bites. Even wind patterns may make a difference by spreading aerosolized organisms downwind. [7] Outbreaks of Q fever have occurred in an industrial setting from straw board that had been drilled open during part of the construction process. Although the respiratory system is the main organ system affected, the gastrointestinal (GI) and cardiac systems also can be affected.
Morphologic variants
C burnetii lives inside acidic lysosomes, a point that has therapeutic implications, [8] and it has 2 morphologic variants [9] : the small-cell variant (SCV) (0.2 x 0.7 microns), which survives well in the environment because of its resistance to heat and desiccation, pressure, and chemical agents [1] ; and the large-cell variant (LCV), which multiplies in the host monocyte and macrophage. [10] These variants are antigenically different. [10]
The small-cell variant is a sporelike structure, enabling the organism to persist on fomites for more than 1 year. After passive entry into the host-cell phagosome, the organism delays the fusion of the phagosome with lysosomes, presumably using this delay to transform from the small-cell variant into the large-cell variant. Thereafter, the large-cell variant exploits and persists within the acidified phagolysosome of the monocytes and macrophages, using it as a nursery. [11]
C burnetii attaches to host macrophages by means of spectrin-binding proteins called ankyrin and is internalized into the cell, where it fuses with lysosomes to form phagolysosomes. The acidic environment of the phagolysosomes has little effect in defending the host against the invading organism, which multiplies and disseminates itself from this environment. This process is thought to occur mainly in the lungs, the main port of entry of C burnetii. Marrie and Raoult postulated that these morphologic variants create an impairment in the bacterial responses within the host, enabling the persistence of the illness in chronic cases. [3]
Proliferation of organisms within the phagolysosome eventually ruptures the host cell. The infected pulmonary macrophages also are transported systemically, with the reticuloendothelial system (liver, spleen, bone marrow [most commonly]) being the most heavily infected. Immune responses result in inflammation that manifests as formation of non-necrotizing granulomata, termed doughnut granulomata due to the characteristic appearance of a fibrin ring surrounding a fat vacuole. Although classically associated with acute Q fever, doughnut granulomata can develop in other conditions, such as visceral leishmaniasis, cytomegalovirus or Epstein-Barr infections, Hodgkin lymphoma, and allopurinol hypersensitivity reaction.
Infectious phases
Like other gram-negative bacteria, C burnetii possesses a lipopolysaccharide as a virulence factor that also is responsible for an antigenic phase variation, an important property that first was utilized for serologic diagnosis by Bengtson in 1941. [3, 10, 11, 12] The infection has 2 phases, which are analogous to the lipopolysaccharide rough and smooth phase of Enterobacteriaceae organisms. Bacterial isolates from naturally infected and laboratory-infected eukaryotic cell hosts are virulent and have a phase I (smooth) lipopolysaccharide that helps protect the microorganism from the host’s defense mechanisms. Isolates obtained after repeated passages through embryonated hens’ eggs are rendered avirulent by chromosomal deletions and have a phase II (rough) lipopolysaccharide.
The phase 1 form is responsible for acute Q fever infections. The phase 2 form has been identified during transmission of C burnetii in immunoincompetent hosts, such as embryonated hen eggs or cell-culture systems. [13] Variations between phase 1 and phase 2 appear to be correlated with changes in smooth or rough lipopolysaccharides.
Immune response
Antibodies against phase I and II antigens can be measured in sera of affected hosts. Phase II antibodies are positive in acute Q fever, whereas phase I antibodies remain elevated in chronic disease. During acute Q fever, immunoglobulin M (IgM) antibodies develop against phase 1 and phase 2 forms, whereas immunoglobulin G (IgG) antibodies develop only against the phase 2 form. In chronic Q fever, both IgG and immunoglobulin A (IgA) antibodies are formed against both phase 1 and phase 2 forms. The selective development of the antibodies against each of the 2 forms of C burnetii has become the basis for serologic testing for acute versus chronic Q fever.
The immune response against C burnetii is both cell mediated and humoral, with cell-mediated immunity appearing to be most important in fending off this organism. Individuals with certain conditions (eg, pregnancy, human immunodeficiency virus [HIV] infection, immunosuppression, heart-valve lesions, and vascular abnormalities) may be at greater risk for more severe disease, [7] and those with impaired cell-mediated immunity are at increased risk for chronic Q fever. Infected pregnant women are at risk for spontaneous abortion, premature labor, and intrauterine growth restriction (IUGR), as placental infection may cause direct infection of the fetus. [7]
Potential as biologic warfare agent
In addition to its high infectivity, C burnetii is an extremely virulent organism, as just a single bacterium can cause infection. [8] This feature promoted its development as an agent for biologic warfare. C burnetii has been mass produced and weaponized. It is classified as a category B agent, because it lacks the capacity to cause mass fatalities while causing notable debilitation. The potential effect of an intentional release of 50 kg of C burnetii along a 2-km line upwind of a population of 500,000 is an estimated 150 deaths, 125,000 cases of acute illness, and 9000 cases of chronic illness, according to World Health Organization (WHO) estimates. [14]
Etiology
Q fever is most often related to inhalation of aerosolized organisms during animal exposure, occupational exposure, and tick bites (usually to domesticated household and farm animals). C burnetii —a strict, intracellular, pleomorphic, gram-negative coccobacillus classified as a Legionellae species—is the causative organism; it localizes in the mammary glands, uterus, and feces of domestic and small mammals. However, because of the persistence of Coxiella organisms in nature as a sporelike structure (making it highly resistant to inactivation; it can survive for months in dust and feces particles), C burnetii can infect people with no known contact with animals. For example, an outbreak of Q fever was reported in people living along a road on which farm vehicles contaminated with straw and manure traveled. Laboratory outbreaks have also occurred. Only 1 case of documented human-to-human transmission exists.
Why chronic Q fever develops in certain patients is unknown. Current understanding of chronic Q fever indicates activation of a previously asymptomatic infection.
Epidemiology
United States statistics
Q fever became a reportable disease in 1999, except for Delaware, Iowa, Oklahoma, Vermont, and West Virginia. [1] Before then, the annual incidence rate was 21 cases. From 2000 to 2004, the mean annual incidence of Q fever rose to 51 cases, with the highest incidence in the Midwest states, although the largest total number of cases was reported in California. Indeed, Q fever was reported to be endemic to California during the 1950s. [15] In 2005, 136 cases were reported to the CDC; in 2006, 169 cases were reported. Dairy and slaughterhouse workers are most at risk. In 2006, the incidence was reported to be 0.06 per 100,000 population.
More recently, Q fever has been reported in US military personnel deployed in Iraq and in Afghanistan, including some patients who were infected without known animal exposure. [12] Indeed, since 2003, more than 200 cases of acute Q fever have been reported among US military personnel deployed to Iraq.
In May 2010, the Centers for Disease Control and Prevention (CDC) issued a health advisory warning about the potential for Q fever among travelers returning from Iraq and The Netherlands. [16] There have been increasing reports of Q fever among deployed US military personnel and civilian contractors caused by endemic transmission in Iraq. In addition, a large ongoing outbreak of Q fever in the Netherlands may place travelers to these regions at risk for infection. [16] In The Netherlands, almost 4000 cases of acute Q fever have been diagnosed since 2007, but none of those have involved US travelers. [16]
International statistics
First described in Australia in 1937, multiple international reports of Q fever clusters have been described over the years. The frequency ranges from 5% in urban areas to 30% in rural areas. Because Q fever infection can frequently be asymptomatic or present as a flulike illness in its milder forms, this results in an underrepresentation of the actual incidence. Epidemiologic serologic testing of specimens from blood donors has discovered a higher incidence throughout Africa, ranging from 18% to 37%, whereas "at-risk" farmers in the United Kingdom demonstrated 29% seropositivity. The United Kingdom reports approximately 100 cases annually.
In southern France and Spain, Q fever is highly prevalent; this disease is the second most common cause of community-acquired pneumonia and causing 5% to 8% of endocarditis cases. More recently, a few clusters of Q fever were reported in the province of Nova Scotia, Canada, and were related to exposure to parturient cats.
Q fever is endemic in the Middle East. Transmission may be influenced by hot, dusty conditions and livestock farming practices that may facilitate windborne spread.
In addition, a large number of Q fever cases have been reported in The Netherlands since 2007, with over 3700 human cases reported through March 2010. [16, 17] Infected dairy goat farms are believed to be the source of the outbreak, and most human cases have been reported in the southern region of the country. [16]
Moreover, acute disease seems to have regional variations. An influenzalike illness is the most common presentation of Q fever in Australia. Hepatitis has been reported in France, southern Spain, and Ontario, Canada. Pneumonia is more common in Crete; Switzerland; Nova Scotia, Canada; and the Basque region of Spain. The reason for these variations is unknown, but animal studies suggest important strain differences could be a factor.
Racial, sexual, and age differences in incidence
Although Q fever has no reported racial predilection, there are differences between the sexes and variations among age groups.
Symptomatic Q fever is more common in males (ratio range, 1.5-3.5:1), [12] accounting for 77% of Q fever cases reported in the United States. In Australia and France, males are 5-fold and 2.5-fold more likely than females to develop disease, respectively. Occupational and recreational exposure (eg, on farms, in industry [abattoirs], in work as veterinarians, while hunting) could represent a selection bias.
Adults are affected more often than children; the average age of infected individuals is approximately 45-50 years. Where cattle are the reservoir, the disease is most prevalent in active men aged 25-40 years. The incidence, as determined by the age at which seroconversion of blood donors occurs, can be deceptive because children, elderly persons, and sick persons do not donate blood.
Patients older than 15 years are more likely to present with clinical symptoms. Symptomatic Q fever is rare in children but, if present, manifests as in adults, whether acute or chronic. [12] During the largest outbreak in Switzerland, symptomatic Q fever was 5 times more likely to occur in those aged 15 years or older than those younger than 15 years, [18] whereas a study in Greece indicated that the prevalence of clinical cases in children increased with age.
Data from one study suggested an increasing incidence of hepatitis with young age and an increasing incidence of pneumonia with aging. Infection during pregnancy can lead to premature birth, low birth weight, and spontaneous abortion. Chronic Q fever also has been associated with recurrent miscarriages.
Prognosis
Acute Q fever is a self-limited disease (in 38% of cases) and has an excellent prognosis if properly diagnosed and treated. More than 50% of patients are asymptomatic, and only 2% to 4% require hospitalization. The mortality rate for symptomatic patients is less than 1%. Children are usually more mildly affected than adults.
Chronic Q fever requires prolonged antimicrobial therapy and close follow-up care with an infectious disease specialist. Frequent relapses (50%) are observed despite adequate therapy, and this disease carries mortality rates that can exceed 60%. The most common cause of chronic Q fever is endocarditis. Untreated endocarditis is almost universally fatal, although the mortality rate decreases to less than 10% with appropriate treatment; the overall mortality rate remains 10% to 25%.
Complications of Q fever may include the following:
-
Thrombocytopenia
-
Endocarditis caused by chronic infection as well as infection of vascular aneurysms and prostheses, which can lead to severe heart failure
-
Spontaneous abortion and premature labor
-
Reactivation during pregnancy
-
Meningoencephalitis
-
Increased rate of abortions
-
Chronic fatigue syndrome
Patient Education
Patient education focuses primarily on issues of avoidance and deterrence, such as the following:
-
Avoid ingestion of unpasteurized milk and dairy products, particularly goat cheese
-
Avoid parturient and farm animals and exposure to animal birth products (eg, placenta), especially in the setting of immunosuppression, pregnancy, or known valvular heart disease
-
Birthing should take place in indoor facilities
-
Properly dispose of placentae, fetal membranes, and aborted material
-
Minimize occupational exposure
-
Maintain appropriate precautions during periods of potential exposure
-
Take precautions to avoid tick bites, including using permethrin, diethyltoluamide (DEET), and other repellents (see Tick-borne Diseases)
-
Identify infections in domesticated animal populations
See also Prevention.
For patient education information, see Ticks.
-
A: Chest radiograph with normal findings. B: Chest radiograph demonstrating Q fever pneumonia.
