Practice Essentials
Sulfonylureas are oral hypoglycemic agents extensively used in the treatment of type 2 diabetes, [1] The wide availability of these medications increases the potential for intentional or unintentional overdose in pediatric and adult populations.
First-generation sulfonylurea compounds became widely available in 1955. They are acetohexamide, chlorpropamide, tolazamide, and tolbutamide. First-generation agents have long half-lives (eg, 49 hours for chlorpropamide). Second-generation sulfonylureas were introduced in 1984 and include glipizide, glyburide, and glimepiride. Second-generation sulfonylureas are more potent and have shorter half-lives than the first-generation sulfonylureas.
Other oral agents besides sulfonylureas are used to treat type 2 diabetes, including biguanides, alpha-glucosidase inhibitors, thiazolidinediones, selective sodium-glucose cotransporter 2 (SGLT2) inhibitors, glucagon-like peptide-1 (GLP-1) agonists, and dipeptidyl peptidase IV (DPP-4) inhibitors. [2] Metformin, a biguanide, is one such agent. Even in overdose, for the most part those agents do not decrease serum glucose below euglycemia; consequently, they are appropriately referred to as antihyperglycemic agents rather than hypoglycemic agents. Overdose of antihyperglycemic agents can have other dangerous adverse effects (for example, lactic acidosis from metformin, [3] decreased kidney function from an SGLT2 inhibitor [4] ). However, this article focuses on acute overdose of sulfonylureas.
Hypoglycemia from sulfonylureas can result from small doses, can be delayed in onset, and can be persistent. The risk of hypoglycemia varies by drug and patient populations. For example, glyburide has greater hypoglycemic effects than glipizide and glimepiride, particularly in patients with kidney dysfunction and in the elderly. [5]
Prolonged observation and intensive care to restore and maintain euglycemia may be required. [6] (See Treatment and Medication.)
Pathophysiology
Sulfonylureas are sulfonamide derivatives but do not have any antibacterial activity. The exact mechanism of sulfonylureas' hypoglycemic effect remains to be elucidated. These drugs are mainly effective in patients with functional pancreatic beta cells. Sulfonylureas bind to receptors that are associated with potassium channels sensitive to adenosine triphosphate in beta-cell membrane. The binding inhibits efflux of potassium ions from the cells, resulting in depolarization, influx of calcium ions, and release of preformed insulin. Sulfonylureas may also cause the decrease of serum glucagon and potentiate the action of insulin at the extrapancreatic tissues.
Normal hypoglycemic counterregulation is illustrated in the image below.
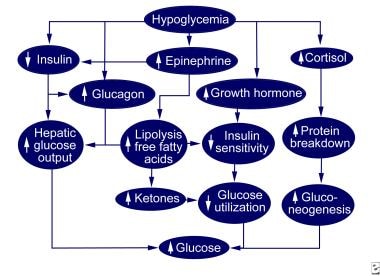 Normal hypoglycemic counterregulation.
Normal hypoglycemic counterregulation.
Epidemiology
Frequency
United States
The American Association of Poison Control Centers' (AAPCC) National Data Collection System compiles an annual report of human poison exposure cases. Overall, the number of exposures to oral sulfonylureas fell from 2012 to 2022. [7, 8, 9, 10, 11, 12, 13, 14, 15, 16] Approximately half of exposures are in the pediatric population and are due to unintentional ingestion.
Table. Sulfonylurea exposures reported to the American Association of Poison Control Centers' National Data Collection System from 2012-2022 (Open Table in a new window)
Year |
Exposures |
< 6 Years |
≥6 Years |
Unintentional Exposures |
Overall Mortality* |
Pediatric Mortality |
2012 |
1753 |
850 |
798 |
1449 |
1† |
- |
2013 |
1590 |
778 |
762 |
1340 |
0 |
0 |
| 2014 | 1584 | 778 | 769 | 1316 | 2 | 0 |
| 2015 | 1659 | 807 | 852 | 1413 | 2 | 0 |
| 2016 | 1582 | 677 | 905 | 1295 | 2† | - |
| 2017 | 1471 | 693 | 778 | 1240 | 2† | - |
| 2018 | 1512 | 613 | 899 | 1199 | 1† | |
| 2019 | 1370 | 570 | 800 |
1113 | 0 | |
| 2020 | 1189 | 482 | 707 | 957 | 1† | |
| 2021 | 1084 | 409 | 640 | 844 | 2† | |
| 2022 | 1098 | 416 | 649 | 840 | 2† | |
*Overall mortality includes adult and pediatric cases † Patient age not noted |
||||||
Race, Sex, and Age
No racial or sex predilection has been reported in sulfonylurea exposure. Toxicity can occur in all ages, but most hypoglycemic overdoses occur in persons 6-19 years old.
Prognosis
Prognosis depends mainly on the early recognition of sulfonylurea exposures, the amount ingested, and the half-life of the drug. Most patients with oral hypoglycemic poisoning recover without any complications. In severe cases, possible complications include coma, recurrent seizures, permanent neurologic deficits, intellectual disability, and death.
Patient Education
Parents should keep medication inaccessible to children. For patient education resources, see the Poisoning - First Aid and Emergency Center, as well as Poisoning, Activated Charcoal, and Poison Proofing Your Home.
-
Normal hypoglycemic counterregulation.
Tables
Year |
Exposures |
< 6 Years |
≥6 Years |
Unintentional Exposures |
Overall Mortality* |
Pediatric Mortality |
2012 |
1753 |
850 |
798 |
1449 |
1† |
- |
2013 |
1590 |
778 |
762 |
1340 |
0 |
0 |
| 2014 | 1584 | 778 | 769 | 1316 | 2 | 0 |
| 2015 | 1659 | 807 | 852 | 1413 | 2 | 0 |
| 2016 | 1582 | 677 | 905 | 1295 | 2† | - |
| 2017 | 1471 | 693 | 778 | 1240 | 2† | - |
| 2018 | 1512 | 613 | 899 | 1199 | 1† | |
| 2019 | 1370 | 570 | 800 |
1113 | 0 | |
| 2020 | 1189 | 482 | 707 | 957 | 1† | |
| 2021 | 1084 | 409 | 640 | 844 | 2† | |
| 2022 | 1098 | 416 | 649 | 840 | 2† | |
*Overall mortality includes adult and pediatric cases † Patient age not noted |
||||||
