Background
Partial anomalous pulmonary venous connection (PAPVC) is a rare congenital cardiac defect. As the name suggests, in PAPVC, the blood flow from a few of the pulmonary veins return to the right atrium instead of the left atrium. Usually, a single pulmonary vein is anomalous. Rarely, all the veins from one lung are anomalous. Thus, some of the pulmonary venous flow enters the systemic venous circulation.
Embryologically, PAPVC is similar to total anomalous pulmonary venous connection (TAPVC); however, TAPVC differs in that all or most pulmonary venous vessels connect to the right side of the heart in TAPVC (see the image below). Knowledge of the variation patterns of normal pulmonary venous drainage is necessary in order to diagnose PAPVC.
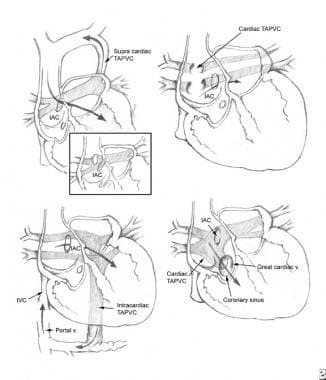 Anomalous pulmonary venous return (APVR). Types of total anomalous pulmonary venous connection.
Anomalous pulmonary venous return (APVR). Types of total anomalous pulmonary venous connection.
PAPVC from the right lung is twice as common as PAPVC from the left lung. The most common form of PAPVC is one in which a right upper pulmonary vein connects to the right atrium or the superior vena cava. This form is almost always associated with a sinus venosus type of atrial septal defect (ASD).
The right pulmonary veins can also drain into the inferior vena cava. The left pulmonary veins can drain into the innominate vein, the coronary sinus, and, rarely, the cavae, right atrium, or left subclavian vein.
Anatomically, PAPVC can involve a wide variety of connections, and can be subdivided into several categories.
PAPVC with ASD (80-90% cases)
This is the most common type of PAPVC. The ASD is usually the sinus venosus type. Approximately 10% have a secundum ASD associated with this anomaly. The anomalous pulmonary vein, usually the right upper or middle pulmonary vein can either override the intra atrial septum (anomalous drainage) or can drain separately into the superior vena cava (true anomalous connection). Usually, the connection is unobstructed.
PAPVC with intact atrial septum (isolated PAPVC)
This is a very rare finding and mostly involves the anomalous drainage of the right upper pulmonary vein into the superior vena cava. [1] Only 3% of patients had PAPVC from the left lung to the innominate vein.
PAPVC with complex congenital heart disease (heterotaxia)
This is usually seen with heterotaxia syndromes (polysplenia). Left atrial isomerism with a common atrium is observed. Because of the abnormal positioning of the intra-atrial septum, the right-sided pulmonary veins anastomose to the anatomically right-sided atrium, which is the atrium that also receives the inferior vena cava. About half of the cases may involve some degree of obstruction, either due to narrowing of a discrete area or due to diffuse hypoplasia of that vein. This condition is associated with presence of ipsilateral pulmonary arterial hypoplasia.
Scimitar syndrome (right pulmonary vein to inferior vena cava with lung sequestration)
This syndrome is also known as Halasz syndrome, mirror-image lung syndrome, hypogenetic lung syndrome, epibronchial right pulmonary artery syndrome, vena cava bronchovascular syndrome, or congenital pulmonary venolobar syndrome. It is more common in females and can be familial.
Usually, the anomaly involves the right lung; the left lung is very rarely involved. In this syndrome, a venous anomaly, an arterial anomaly, and pulmonary anomaly are all observed.
The pulmonary abnormality includes a sequestered lobe of the lung that is separated from the bronchial tree and has nonfunctioning lung tissue. It is associated with hypoplastic or aplastic right pulmonary artery segments, hypoplastic or absent bronchi, hypoplasia of the right lung, horseshoe lung, and eventration of the hemidiaphragm.
The venous anomaly is PAPVC, usually with the right pulmonary veins draining into the inferior vena cava. The arterial anomaly is a collateral arterial vessel (aberrant vessel) with blood supply of the right lower lobe from the abdominal aorta. Dextropositioning of the heart due to right lung hypoplasia may be observed. Usually, the atrial septum is intact. About 25% cases have other associated congenital heart defects.
Pathophysiology
Numerous factors determine the ratio of pulmonary blood flow (Qp) to systemic flow (Qs). The shunt magnitude, expressed as the Qp:Qs ratio, and other factors determine development of symptoms and complications in partial anomalous pulmonary venous connection (PAPVC).
The most important factor is the number of pulmonary veins that drain into the systemic circulation. The more veins that anomalously drain, the more blood returns to the right side of the heart. Some authors have suggested that this defect becomes clinically significant when 50% or more of the pulmonary veins anomalously return.
In addition, the source of the returning blood plays a role in determining the clinical effect of the defect. In an individual who is upright, blood flow to the lungs is primarily directed to the lower and middle lobes. Therefore, more blood returns to the systemic venous circulation in individuals in whom the anomalous connection drains into either the right middle and lower lobes or the left lower lobe of the lung.
An associated cardiac defect, such as an ASD, may add to the left-to-right shunting.
In scimitar syndrome, the flow from the PAPVC causes a left-to-right shunt. Again, the number of anomalous veins involved determines the symptoms and signs. The aberrant artery may cause additional left-to-right shunt.
Over many years, excessive pulmonary venous return to the right side of the heart causes right atrial and ventricular dilation. This has numerous consequences, including risk of arrhythmia development, right-sided heart failure, and development of pulmonary hypertension.
A native PAPVC usually does not have any associated obstruction to venous drainage. However, obstruction may occur postoperatively due to baffle obstruction.
Etiology
Partial anomalous pulmonary venous connection (PAPVC) is a congenital cardiac defect with no known cause and possibly has a multifactorial origin, including a genetic component. It is also seen with Turner syndrome.
No causes of this condition are known. No evidence has implicated common teratogens (eg, drugs, infections) in the genesis of PAPVC. No evidence for a genetic predisposition has been reported.
Epidemiology
United States data
Most data regarding the prevalence of partial anomalous pulmonary venous connection (PAPVC) have been garnered from autopsy series that estimate an incidence of 0.4-0.7%. However, autopsy series may overestimate the clinical significance of this condition because many of these cases were asymptomatic; thus, the true incidence of patients who present antemortem with this condition is lower. Clinical diagnosis of isolated PAPVC is quite rare. PAPVC occurs in approximately 10% of patients with a proven ASD.
Race-, sex-, and age-related demographics
No data regarding racial predilection are available.
The incidence is higher in the female population.
PAPVC is a congenital defect. Clinical evidence of this congenital defect may not be apparent until the patient reaches middle age.
Prognosis
Prognosis is excellent for patients with partial anomalous pulmonary venous connection (PAPVC). The perioperative mortality rate is comparable to that for ASD repair (< 0.1%).
Prognosis becomes more guarded if the lesion is undetected for a long period and if complications, particularly pulmonary hypertension, develop.
The only postoperative death in the series by Gustafson et al involved a woman with pulmonary hypertension. [2]
Morbidity/mortality
Few data are available regarding mortality due to this lesion because mortality attributed to the defect occurs only in adults and the diagnosis has historically been made at autopsy. Major morbidity, including arrhythmias, right-sided cardiac failure, and, rarely, pulmonary vascular disease, also primarily occurs in adults.
Complications
No significant complications develop in pediatric patients who do not undergo surgery for a sinus venosus atrial septal defect (ASD) repair with internal patch technique to include the right upper pulmonary vein in the left atrium. However, other types of repair may be associated with complications such as SVC syndrome, pulmonary venous obstruction, atrial arrhythmias, and sick sinus syndrome.
Arrhythmias may occur in adults with unrepaired PAPVC secondary to chronic right atrial enlargement due to volume overload.
Cardiac failure and, very rarely, pulmonary hypertension may develop in adults.
Patients with scimitar syndrome may be asymptomatic or may have symptoms related to lung pathology, including recurrent pneumonias.
-
Anomalous pulmonary venous return (APVR). Types of total anomalous pulmonary venous connection.
-
Partial anomalous pulmonary venous return of the left lower pulmonary vein seen entering the innominate vein as demonstrated via echocardiogram (A) and angiogram (B).
