Practice Essentials
Hepatitis B infection is a worldwide healthcare problem, especially in developing areas. The hepatitis B virus (HBV) is commonly transmitted via body fluids such as blood, semen, and vaginal secretions. [1]
The hematoxylin and eosin (H&E) stain below depicts "ground-glass" cells seen in approximately 50-75% of livers affected by chronic HBV infection.
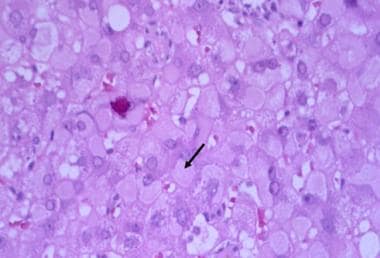 Hepatitis B. Under higher-power magnification, ground-glass cells may be visible in chronic hepatitis B virus (HBV) infection. Ground-glass cells are present in 50% to 75% of livers with chronic HBV infection. Immunohistochemical staining is positive for hepatitis B surface antigen (HBsAg.)
Hepatitis B. Under higher-power magnification, ground-glass cells may be visible in chronic hepatitis B virus (HBV) infection. Ground-glass cells are present in 50% to 75% of livers with chronic HBV infection. Immunohistochemical staining is positive for hepatitis B surface antigen (HBsAg.)
Signs and symptoms
The pathogenesis and clinical manifestations of hepatitis B are due to the interaction of the virus and the host immune system, which leads to liver injury and, potentially, cirrhosis and hepatocellular carcinoma. Patients can have either an acute symptomatic disease or an asymptomatic disease.
Icteric hepatitis is associated with a prodromal period, during which a serum sickness–like syndrome can occur. The symptomatology is more constitutional and includes the following:
-
Anorexia
-
Nausea
-
Vomiting
-
Low-grade fever
-
Myalgia
-
Fatigability
-
Disordered gustatory acuity and smell sensations (aversion to food and cigarettes)
-
Right upper quadrant and epigastric pain (intermittent, mild to moderate)
Patients with fulminant and subfulminant hepatitis may present with the following:
-
Hepatic encephalopathy
-
Somnolence
-
Disturbances in sleep pattern
-
Mental confusion
-
Coma
-
Ascites
-
Gastrointestinal bleeding
-
Coagulopathy
Patients with chronic hepatitis B infection can be immune tolerant or have an inactive chronic infection without any evidence of active disease, and they are also asymptomatic. Patients with chronic active hepatitis, especially during the replicative state, may have symptoms similar to those of acute hepatitis.
See Clinical Presentation for more detail.
Diagnosis
The physical examination findings in hepatitis B disease vary from minimal to impressive (in patients with hepatic decompensation), according to the stage of the disease.
Examination in patients with acute hepatitis may demonstrate the following:
-
Low-grade fever
-
Jaundice (10 days after appearance of constitutional symptomatology; lasts 1-3 mo)
-
Hepatomegaly (mildly enlarged, soft liver)
-
Splenomegaly (5-15%)
-
Palmar erythema (rarely)
-
Spider nevi (rarely)
Signs of chronic liver disease include the following:
-
Hepatomegaly
-
Splenomegaly
-
Muscle wasting
-
Palmar erythema
-
Spider angiomas
-
Vasculitis (rarely)
Patients with cirrhosis may have the following findings:
-
Ascites
-
Jaundice
-
History of variceal bleeding
-
Peripheral edema
-
Gynecomastia
-
Testicular atrophy
-
Abdominal collateral veins (caput medusa)
Laboratory studies
The following laboratory tests may be used to assess the various stages of hepatitis B disease:
-
Alanine aminotransferase and/or aspartate aminotransferase levels
-
Alkaline phosphatase levels
-
Gamma-glutamyl transpeptidase levels
-
Total and direct serum bilirubin levels
-
Albumin level
-
Hematologic and coagulation studies (eg, platelet count, complete blood count [CBC], international normalized ratio)
-
Ammonia levels
-
Erythrocyte sedimentation rate
-
Serologic tests
The serologic tests should include the following laboratory studies:
-
Hepatitis B surface antigen (HBsAg)
-
Hepatitis B e antigen (HBeAg)
-
Hepatitis B core antibody (anti-HBc) immunoglobulin M (IgM)
-
anti-HBc IgG
-
Hepatitis B e antibody (anti-HBe)
-
hepatitis B virus (HBV) deoxyribonucleic acid (DNA)
Imaging studies
The following radiologic studies may be used to evaluate patients with hepatitis B disease:
-
Abdominal ultrasonography
-
Abdominal computed tomography (CT) scanning
-
Abdominal magnetic resonance imaging (MRI)
Procedures
Liver biopsy, percutaneous or laparoscopic, is the standard procedure to assess the severity of disease in patients with features of chronic active liver disease (ie, abnormal aminotransferase levels and detectable levels of HBV DNA).
See Workup for more detail.
Management
The primary treatment goals for patients with hepatitis B infection are to prevent progression of the disease, particularly to cirrhosis, liver failure, or hepatocellular carcinoma (HCC). [2] Pegylated interferon alfa (PEG-IFN-a), entecavir, and tenofovir disoproxil fumarate are the FDA-approved agents in the treatment of hepatitis B disease.
Pharmacotherapy
The following medications are used in the treatment of hepatitis B:
-
Nucleos(t)ide reverse transcriptase inhibitors (eg, tenofovir disoproxil fumarate, tenofovir alafenamide, lamivudine)
-
Hepatitis B/hepatitis C agents (eg, adefovir dipivoxil, entecavir, PEG-IFN-a 2a, interferon alfa-2b)
Dietary changes
For individuals with decompensated cirrhosis (prominent signs of portal hypertension or encephalopathy), the following dietary limitations are indicated:
-
A low-sodium diet (1.5 g/day)
-
High-protein diet (ie, white-meat protein [eg, chicken, turkey, fish])
-
Fluid restriction (1.5 L/day) in cases of hyponatremia
Liver transplantation
Orthotopic liver transplantation is the treatment of choice for patients with fulminant hepatic failure who do not recover and for patients with end-stage liver disease due to hepatitis B disease.
See Treatment and Medication for more detail.
Background
Hepatitis B is a worldwide healthcare problem, especially in developing areas. An estimated one third of the global population is infected with the hepatitis B virus (HBV). Approximately 250-350 million people have lifelong chronic infection, [3] with approximately 1.5 million new cases every year. [4] Approximately 0.5% of patients spontaneously seroconvert annually from having the hepatitis B surface antigen (HBsAg) to having the hepatitis B surface antibody (anti-HBs). [5] (See Pathophysiology, Etiology, and Epidemiology.)
Complications from hepatitis B include progression to hepatocellular carcinoma (HCC) and, rarely, cirrhosis. Extrahepatic disease can involve glomerulonephritis and polyarteritis nodosa, as well as various dermatologic, cardiopulmonary, joint, neurologic, hematologic, and gastrointestinal (GI) manifestations. (See Pathophysiology.)
Since the 1970s, considerable progress has also been made regarding the knowledge of the epidemiology, virology, natural history, and treatment of the hepatitis B virion, a hepatotropic virus particle (see the image below). In addition, ongoing vaccination programs have been successful in many countries and territories in decreasing the prevalence of HBV disease (eg, Taiwan). [6] (See Etiology, Epidemiology, Workup, Treatment, and Medication.)
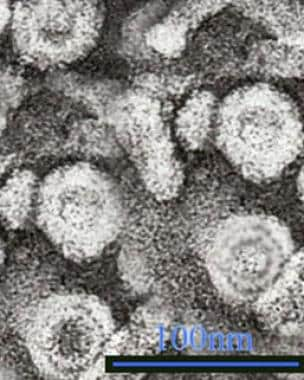 Hepatitis B. Hepatitis B virus (HBV) is a hepadnavirus, highly resistant to extremes of temperature and humidity, that invades the hepatocytes. The viral genome is a partially double-stranded, circular DNA linked to a DNA polymerase that is surrounded by an icosahedral nucleocapsid and then by a lipid envelope. Embedded within these layers are numerous antigens that are important in disease identification and progression. Within the nucleocapsid are the hepatitis B core antigen (HBcAg) and precore hepatitis B e antigen (HBeAg), and on the envelope is the hepatitis B surface antigen (HBsAg). Transmission electron micrograph (TEM) from Graham Colm and Wikipedia, licensed under the Creative Commons Attribution 3.0 Unported license.
Hepatitis B. Hepatitis B virus (HBV) is a hepadnavirus, highly resistant to extremes of temperature and humidity, that invades the hepatocytes. The viral genome is a partially double-stranded, circular DNA linked to a DNA polymerase that is surrounded by an icosahedral nucleocapsid and then by a lipid envelope. Embedded within these layers are numerous antigens that are important in disease identification and progression. Within the nucleocapsid are the hepatitis B core antigen (HBcAg) and precore hepatitis B e antigen (HBeAg), and on the envelope is the hepatitis B surface antigen (HBsAg). Transmission electron micrograph (TEM) from Graham Colm and Wikipedia, licensed under the Creative Commons Attribution 3.0 Unported license.
HBV is transmitted vertically from mother to fetus, hematogenously, and sexually. The outcome of this infection is a complicated viral-host interaction that results in either an acute symptomatic disease or an asymptomatic disease. Some patients clear HBV and develop anti-HBs; however, as long as the individual has antibody to hepatitis B core antigen (HBcAg), he or she is at risk for reactivation because HBV infection remains an incurable disease, similar to Epstein-Barr virus (EBV), cytomegalovirus (CMV), and Herpes simplex virus (HSV) infections. Alternatively, a patient may develop a chronic infection state with positivity for HBsAg. Late consequences are cirrhosis and the development of HCC in 15-30% of individuals. [6, 7, 8, 9]
In immunocompetent adults, less than approximately 4% of HBV infections become chronic, whereas up to 90% of perinatally infected infants will have chronic disease. [10] Among children who acquire HBV infection between ages 1 and 5 years, 30-50% become chronically infected.
Taiwan launched a nationwide HBV vaccination program in 1984. The prevalence of HCC in children younger than 20 years has been reported to be 0.5% or less. [6]
According to the World Health Organization (WHO), by the end of 2010, the HBV vaccine had been routinely introduced in 179 countries, with a global coverage of 75%. Coverage in the Americas was at 89%; in Europe, 78%; in Africa, 76%; and in Southeast Asia, 52%. [11]
Antiviral treatment may be effective in approximately 95% of the patients who are treated with first-line oral therapy, as defined by undetectable HBV DNA. For those who are treated with interferon, about 17% have persistent HBV DNA suppression. For selected candidates, liver transplantation currently seems to be the only viable treatment for the later stages of hepatitis B infection, with a posttransplantation viral suppression of greater than 90-95%. (See Treatment and Medication.)
See also Liver Disease in Pregnancy, Hepatitis A, Hepatitis C, Hepatitis D, and Hepatitis E.
Pathophysiology
Hepatitis B virus (HBV) is a hepadnavirus (see the following image), with the virion consisting of a 42-nm spherical, double-shelled particle composed of small spheres and rods and with an average width of 22 nm. [12, 13, 14, 15, 16] It is an exceedingly resistant virus, capable of withstanding extreme temperatures and humidity. HBV can survive when stored for 15 years at –20°C, for 24 months at –80°C, for 6 months at room temperature, and for 7 days at 44°C. Indeed, the approximately 400-year-old mummified remains of a child found on a mountain top in Korea had HBV in the liver that could be sequenced, and a viral genotype C was identified. [17]
Hepatitis B. Hepatitis B virus (HBV) is a hepadnavirus, highly resistant to extremes of temperature and humidity, that invades the hepatocytes. The viral genome is a partially double-stranded, circular DNA linked to a DNA polymerase that is surrounded by an icosahedral nucleocapsid and then by a lipid envelope. Embedded within these layers are numerous antigens that are important in disease identification and progression. Within the nucleocapsid are the hepatitis B core antigen (HBcAg) and precore hepatitis B e antigen (HBeAg), and on the envelope is the hepatitis B surface antigen (HBsAg). Transmission electron micrograph (TEM) from Graham Colm and Wikipedia, licensed under the Creative Commons Attribution 3.0 Unported license.
Viral genome
The viral genome of hepatitis B consists of a partially double-stranded, circular DNA molecule of 3.2 kilobase (kb) pairs that encodes the following 4 overlapping open reading frames:
-
S (the surface, or envelope, gene): Encodes the pre-S1, pre-S2, and S proteins
-
C (the core gene): Encodes the core nucleocapsid protein and the e antigen; an upstream region for the S (pre-S) and C (pre-C) genes has been found
-
X (the X gene): Encodes the X protein
-
P (the polymerase gene): Encodes a large protein promoting priming ribonucleic acid (RNA) ̶ dependent and DNA-dependent DNA polymerase and ribonuclease H (RNase H) activities
Surface gene
The S gene encodes the viral envelope. There are five main antigenic determinants: (1) a, common to all hepatitis B surface antigens (HBsAg), and (2-5) d, y, w, and r, which are all epidemiologically important and identify the serotypes.
Core gene
The core antigen, HBcAg, is the protein that encloses the viral DNA. It can also be expressed on the surface of the hepatocytes, initiating a cellular immune response.
The e antigen, HBeAg, which is also produced from the region in and near the core gene, is a marker of active viral replication. It serves as an immune decoy and directly manipulates the immune system; it is thus involved in maintaining viral persistence. HBeAg can be detected in patients with circulating serum HBV DNA who have “wild type” infection. As the virus evolves over time under immune pressure, core promotor and precore mutations emerge, and HBeAg levels fall until the level is not measurable by standard assays.
Individuals who are infected with the wild type virus often have mixed infections, with core and precore mutants in up to 50% of individuals. They often relapse with HBeAg-negative disease after treatment.
X gene
The role of the X gene is to encode proteins that act as transcriptional transactivators that aid viral replication. Evidence strongly suggests that these transactivators may be involved in carcinogenesis.
Antibody production
The production of antibodies against HBsAg (anti-HBs) confers protective immunity and can be detected in patients who have recovered from HBV infection or in those who have been vaccinated.
Antibody to HBcAg (anti-HBc) is detected in almost every patient with previous exposure to HBV and indicates that there is a minute level of persistent virus, as demonstrated by the risk of reactivation in individuals who undergo immune suppression regardless of their anti-HBs status.
The immunoglobulin M (IgM) subtype of anti-HBc is indicative of acute infection or reactivation, whereas the IgG subtype is indicative of chronic infection. The activity of the disease cannot be understood using this marker alone, however.
Antibody to HBeAg may be suggestive of a nonreplicative state if there is undetectable HBV DNA or the emergence of the core/precore variants and of chronic HBV HBeAg-negative disease.
Variants of HBV
With the newest polymerase chain reaction (PCR) assay techniques, scientists are able to identify variations in the HBV genome (variants) as far back as 1995, even in patients who are positive for HBeAg. Mutations of various nucleotides such as the 1896, 1764, and 1768 (precore/core region) processing the production of the HBeAg have been identified (HBeAg-negative strain). [18]
These variants are generally less efficient at viral replication without HBeAg and tend to have lower viral loads, although with a suspected higher risk of development of cirrhosis and hepatocellular carcinoma (HCC). [19]
The prevalence of the HBeAg-negative virus varies from one region to another. Estimates indicate that among patients with chronic HBV infection, 50-60% of those from Southern Europe, the Middle East, Asia, and Africa, as well as 10-30% of patients in the United States and Europe, have been infected with this strain.
Immune response
The pathogenesis and clinical manifestations of hepatitis B infection are due to the interaction of the virus and the host immune system. The immune system attacks HBV and causes liver injury, the result of an immunologic reaction when activated CD4+ and CD8+ lymphocytes recognize various HBV-derived peptides on the surface of the hepatocytes. Impaired immune reactions (eg, cytokine release, antibody production) or a relatively tolerant immune status result in chronic hepatitis. In particular, a restricted T-cell–mediated lymphocytic response occurs against the HBV-infected hepatocytes. [20, 21]
The final state of HBV disease is cirrhosis. With or without cirrhosis, however, patients with HBV infection are at risk of developing HCC. [6, 7, 8] In the United States, hepatitis B–associated HCC cases most often occur in the setting of vertical transmission (mother to fetus) in patients of Asian descent.
Viral life cycle
The five stages that have been identified in the viral life cycle of hepatitis B infection are briefly discussed below. Different factors have been postulated to influence the development of these stages, including age, sex, immunosuppression, and coinfection with other viruses.
Stage 1: Immune tolerance
This stage, which lasts approximately 2-4 weeks in healthy adults, represents the incubation period. For newborns, the duration of this period is often decades. Active viral replication is known to continue despite little or no elevation in the aminotransferase levels and no symptoms of illness.
Stage 2: Immune active/immune clearance
In the immune active stage, also known as the immune clearance stage, an inflammatory reaction with a cytopathic effect occurs. Serum HBeAg can be identified, and a decline in the levels of HBV DNA is seen in some patients who are clearing the infection. The duration of this stage for patients with acute infection is approximately 3-4 weeks (symptomatic period). For patients with chronic infection, 10 years or more may elapse before cirrhosis develops, immune clearance takes place, HCC develops, or the chronic HBeAg-negative variant emerges.
Stage 3: Inactive chronic infection
In the third stage, the inactive chronic infection stage, the host can target the infected hepatocytes and HBV. Viral replication is low or no longer measurable in the serum, and anti-HBe can be detected. Aminotransferase levels are within the reference range. It is likely that at this stage, an integration of the viral genome into the host's hepatocyte genome takes place. HBsAg still is present in the serum.
Stage 4: Chronic disease
The emergence of chronic HBeAg-negative disease can occur from the inactive chronic infection stage (stage 3) or directly from the immune active/clearance stage (stage 2).
Stage5: Recovery
In the fifth stage, the virus cannot be detected in the blood by DNA or HBsAg assays, and antibodies to various viral antigens have been produced. The image below depicts the serologic course of HBV infection.
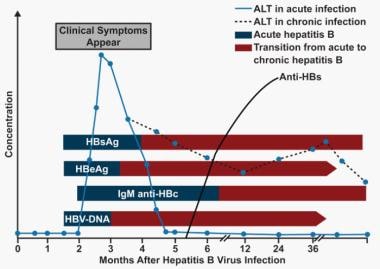 Hepatitis B. Serologic course of hepatitis B virus (HBV) infection. The flat bars show the duration of seropositivity in self-limited acute HBV infection. The pointed bars show that HBV DNA and e antigen (HBeAg) can become undetectable during chronic infection. Only immunoglobulin G (IgG) antibodies to the HBV core antigen (anti-HBc) are predictably detectable after resolution of acute hepatitis or during chronic infection. Antibody to hepatitis B surface antigen (anti-HBs) is generally detectable after resolution of acute HBV infection but may disappear with time. It is only rarely found in patients with chronic infection and does not indicate that immunologic recovery will occur or that the patient has a better prognosis. ALT = alanine transaminase. (Adapted from Liaw YF, Chu CM. Hepatitis B virus infection. Lancet. 2009;373(9663):582-92.)
Hepatitis B. Serologic course of hepatitis B virus (HBV) infection. The flat bars show the duration of seropositivity in self-limited acute HBV infection. The pointed bars show that HBV DNA and e antigen (HBeAg) can become undetectable during chronic infection. Only immunoglobulin G (IgG) antibodies to the HBV core antigen (anti-HBc) are predictably detectable after resolution of acute hepatitis or during chronic infection. Antibody to hepatitis B surface antigen (anti-HBs) is generally detectable after resolution of acute HBV infection but may disappear with time. It is only rarely found in patients with chronic infection and does not indicate that immunologic recovery will occur or that the patient has a better prognosis. ALT = alanine transaminase. (Adapted from Liaw YF, Chu CM. Hepatitis B virus infection. Lancet. 2009;373(9663):582-92.)
Genotypes and disease progression
Ten different genotypes (A through J), representing a divergence of the viral DNA of about 8%, have been identified. [22] The prevalence of the genotypes varies in different countries. The progression of the disease seems to be more accelerated and the response to treatment with antiviral agents is less favorable for patients infected by genotype C, compared with those infected by genotype B. However, much of this can be explained by the presence of core and precore mutations found in multivariate analysis. [23, 24]
It has been confirmed that the risk of HCC is related to higher serum HBV DNA levels and the duration of HBV DNA presence, with an even higher risk if there is an increasing level of hepatitis B viral load, the presence of genotype C, and the presence of mutations in the precore and basal core promoter regions.
Hepatocellular carcinoma
Even the presence of hepatitis B core antibody (anti-HBc) in the absence of hepatitis B surface antigen (HBsAg) and hepatitis B virus (HBV) DNA is significantly related to an increased risk for HCC, although surveillance for HCC is not recommended in the affected group unless cirrhosis is present. In the United States, the estimated annual incidence of HCC in patients infected with hepatitis B is 818 cases per 100,000 persons. In Taiwan, the annual incidence of this malignancy in patients with hepatitis B and cirrhosis is 2.8%. Familial clustering of HCC has been described among families with hepatitis B in Africa, the Far East, and Alaska.
HBV and HCV coinfection
The prevalence of HCC among patients with HBV and hepatitis C virus (HCV) coinfection is higher than in those with a single infection. The rate of development of HCC per 100 person years of follow-up is 2% in patients with cirrhosis and HBV infection, 3.7% in patients with HCV infection, and 6.4% in patients with dual HBV and HCV infection. These findings point to a probable synergistic effect on the risk of HCC.
HBV and HDV coinfection
Individuals coinfected with hepatitis D (delta) virus (HDV) are thought to have a higher rate of HCC and cirrhosis, with the virus reportedly increasing the risk of HCC 3-fold and mortality rates 2-fold in patients with HBV cirrhosis. [25]
Worldwide, the prevalence of HDV coinfection among patients infected with HBV is 0-30%, with the highest prevalence in Mongolia, Southeast Turkey, and the Orinoco River in South America. The speculation that HDV may promote hepatocarcinogenesis in these patients has been investigated with varying results. The prevalence of anti-delta antibody among patients with cirrhosis with and without HCC was not significantly different in one study, whereas most other investigations show the delta virus to be more aggressive, with higher rates of cirrhosis and cancer. [25, 26, 27]
Possible pathogenic mechanisms
The mechanism by which chronic hepatitis B infection predisposes to the development of HCC is not clear. Cirrhosis is a cardinal factor in carcinogenesis. Hepatocyte inflammation, necrosis, mitosis, and features of chronic hepatitis are major factors in nodular regeneration, fibrosis, and carcinoma. Liver cell dysplasia, defined as cellular enlargement, nuclear pleomorphism, and multinucleated cells affecting groups or whole nodules, may be an intermediate step. The high cell-proliferation rate increases the risk of HCC.
The fact that the facultative liver stem cells are capable of bipotent differentiation into hepatocytes or biliary epithelium, termed oval cells, may play an important role in the pathogenesis. These cells are small, with oval nuclei and scant pale cytoplasm.
Oval cells are prominent in actively regenerating nodules and in liver tissue surrounding the cancer. They appear to be the principal producers of alpha-fetoprotein (AFP). Although the cellular targets of carcinogenesis have not been identified, some evidence from experimental animal models suggests that oval cell proliferation is associated with an increased risk for the development of HCC.
Although cirrhosis is found in the majority of patients with HCC, it is not obligatory, because individuals with chronic infection may develop HCC even without the evidence of cirrhosis.
HBV has been speculated to have intrinsic hepatocarcinogenic activity, interacting with host DNA in different ways. After entering the hepatocyte, viral DNA is integrated within the genome. The site of integration is not constant but usually involves the terminal repeat sequences. Chromosomal deletions, translocations, rearrangements, inversions, or even duplications of normal DNA sequencing accompany integration.
Transactivation of the function of genes controlling transcriptional factors (ie, insulinlike growth factor II [IGF-2], transforming growth factor-alpha [TGF-a], TGF-beta, cyclin-a [a protein that controls cell division], epidermal growth factor-r [EGFR], retinoic acid receptor [RAR]), and oncogenes such as c-myc, fos, ras (activating the internal signal transduction cascade upregulating ras/mitogen–activated kinase, c-Jun N terminal kinase, nuclear factor–kB [NF-kB], Jak-1-STAT, src- dependent pathways) influence normal hepatocyte differentiation or cell cycle progression.
Furthermore, the integrated part of HBV controlling the production of the HBxAg (antigen for the X gene of HBV) is overexpressed. These observations suggest that the site of viral genomic integration into the host's DNA is not the only factor.
Most likely, the HBxAg produced by these sequences is the transactivating factor, because it has been found to bind to a variety of transcription factors such as CREB (cyclic adenosine monophosphate [cAMP]–response element-binding protein) and ATF-2 (activating transcription factor 2), altering their DNA-binding specificity. Thus, the ability of the HBV pX protein to interact with cellular factors broadens the DNA-binding specificity of these regulatory proteins and provides a mechanism for pX to participate in transcriptional regulation. This shifts the pattern of host gene expression relevant to the development of HCC.
Additionally, HBxAg has been postulated to bind to the C-terminus and inactivate the product of the tumor suppressor gene TP53, as well as to do the following:
-
Sequester TP53 in the cytoplasm, resulting in the abrogation of TP53 -induced apoptosis (although controversy exists regarding this concept)
-
Reduce the ability for nucleotide excision repair by directly acting with proteins associated with DNA transcription and repair such as XPB and XPD
-
Reduce p21WAF1 expression, which is a cell cycle regulator
-
Bind to protein p55sen, which is involved in the cell fate during embryogenesis and is found in the liver of patients with hepatitis B, thus altering its function
The levels of tumor necrosis factor-alpha (TNF-a), a proinflammatory cytokine, are also upregulated. The transcriptional transactivation of nitric oxide (NO) synthetase II by pX and the elevated levels of TNF-a are responsible for the high levels of NO found in these patients. NO is a putative mutagen that develops through several mechanisms of functional modifications of TP53, DNA oxidation, deamination, and formation of the carcinogenic N-nitroso compounds. A second transactivator is encoded in the pre-S/S region of the HBV genome, stimulating the expression of the human proto-oncogenes c-fos and c-myc; this upregulates the expression of TGF-a by transactivation.
Glomerulonephritis
The most common type of glomerulonephritis described in association with hepatitis B is membranous glomerulonephritis (MGN), found mainly in children. However, membranoproliferative glomerulonephritis (MPGN) and, even more rarely, immunoglobulin (Ig) A nephropathy, have also been identified.
The prevalence rate of glomerulonephritis among patients with chronic hepatitis B is not well known, although observations have been made in children that suggest a range of 11-56.2%. However, such a high prevalence is not recognized in the United States; this may be because of the differences in epidemiology of HBV, which may be predominantly perinatal in other geographic areas of the world (see Epidemiology).
A previous history of chronic liver disease is not present in the majority of patients with chronic hepatitis B at presentation, and most of them have no clinical or biochemical findings to suggest acute or chronic liver disease. However, liver biopsies often demonstrate features of chronic hepatitis. In addition, serologic markers of an HBV replicative state are often evident, and complement activation is suggested by low levels of C3 and C4.
Generally, the most prominent finding among affected children is MGN, primarily with capillary wall deposits of hepatitis B e antigen (HBeAg). In contrast, adults present with features of MPGN with mesangial and capillary wall deposits of HBsAg. A rare overlap between membranous nephropathy and IgA nephropathy has also been described.
Possible pathogenic mechanisms
The mechanism by which patients with chronic hepatitis B develop glomerulonephritis is not completely understood. One possible explanation is that HBV antigens (ie, HBsAg, HBeAg) act as triggering factors, eliciting immunoglobulins and thus forming immune complexes, which are dense, irregular deposits in the glomerular capillary basement membranes. HBV DNA has been identified by in situ hybridization in kidney specimens, distributed generally in the nucleus and cytoplasm of epithelial cells and mesangial cells of glomeruli and in the epithelial cells of renal tubules.
Polyarteritis nodosa
An association between hepatitis B and arteritis has been described when HBsAg is present in serum and in vascular lesions. Evidence for a cause-and-effect relationship is further supported by a high prevalence (36-69%) of HBsAg in patients with polyarteritis nodosa (PAN). This very serious complication presents early during the course of hepatitis B, and the incidence is high among certain populations, such as Alaskan Eskimos.
The pathogenesis of PAN is not clear. Circulating immune complexes containing HBsAg, immunoglobulins (IgG and IgM), and complement have been demonstrated by immunofluorescence in the walls of the affected vessels and may trigger the onset of PAN. However, whether these represent the primary etiology of the disease remains unclear.
The clinical manifestations of PAN include the following:
-
Cardiovascular (eg, hypertension [sometimes severe], pericarditis, heart failure)
-
Renal (eg, hematuria, proteinuria, renal insufficiency)
-
Gastrointestinal (GI) (eg, abdominal pain, mesenteric vasculitis)
-
Musculoskeletal (eg, arthralgias, arthritis)
-
Neurologic (eg, mononeuritis)
-
Dermatologic (eg, rashes)
Significant proteinuria (>1 g/day), renal insufficiency (serum creatinine >1.58 mg/dL), GI and central nervous system involvement, and cardiomyopathy are associated with increased mortality.
The course of PAN is independent of the severity and progression of the liver disease. Among patients with PAN, 20-45% die as a consequence of vasculitis in 5 years, despite treatment, with the mortality rate being similar whether patients are HBsAg seropositive or seronegative.
Etiology
Hepatitis B infection, caused by the hepatitis B virus (HBV), is commonly transmitted via body fluids such as blood, semen, and vaginal secretions. [1] Consequently, sexual contact, accidental needle sticks or sharing of needles, blood transfusions, and organ transplantation are routes for HBV infection. Infected mothers can also pass the infection to their newborns during the delivery period (vertical transmission). [1]
Genetics of infection with hepatitis B
Several genes, many having to do with the host immune response, have been implicated in the susceptibility to chronic hepatitis B infection. The TNFSF9 gene encodes the CD137L protein, and its expression was found to be significantly higher in patients with chronic hepatitis B infection than in healthy controls. Its expression was also found to be higher in patients who had chronic hepatitis B with cirrhosis, in contrast to those without cirrhosis. [28]
Research done in West Africa, where 90% of the population is infected with hepatitis B, shows that certain human leukocyte antigen (HLA) class II haplotypes influence the likelihood of chronic infection. For reasons that are not completely clear, patients in the study who were heterozygous for the HLA-DRA and HLA-DQA1 genes were found to be less likely to develop a chronic infection. [29]
IFNGR1 gene
Several additional genes are associated with susceptibility to hepatitis B infection. The IFNGR1 gene is located at 6q23.3 and encodes the interferon gamma (IFN-γ) receptor 1, which has an important role in cell-to-cell communications and can be activated in response to infection, but it is not specific to hepatitis B. [30] Patients with significant dysfunction in this gene have a particular immune deficiency that leaves them extremely susceptible to mycobacterial infections. [30]
A more subtle change in the promoter region at location -56 in this gene has shown significant association with the natural history of hepatitis B infection. Individuals with the C allele at this location were found in a study to be more likely to clear the virus, whereas individuals with the T allele at this location were more likely to have persistent viral infection. [31]
IFNAR2 gene
The IFNAR2 gene is located at 21q22.1 and encodes the IFN-alpha, -beta, and -omega receptor 2. Although it presumably is like the previous gene, with multiple functions in the immune system, at the present time it is known only to be associated with susceptibility to hepatitis B.
A study looking at this gene found that a single nucleotide polymorphism, resulting in a phenylalanine-to-serine substitution at position 8, was associated with an increased risk for chronic hepatitis B infection. [32]
IL1OR2 gene
The same study also found that a polymorphism in the IL10R2 gene (or the CRFB4 gene), also located at 21q22.11, is associated with an increased risk of chronic hepatitis B infection. This particular polymorphism results in a lysine-to-glutamic acid substitution at position 47. [32]
Variations in vaccine response
It is also known that certain patients have different responses to the hepatitis B vaccine. One study found that 14% of patients who received the vaccine were low responders. [33] A greater-than-expected number of these patients were homozygotes for the HLA-B8, -SC01, and -DR3 haplotypes. It was hypothesized that because HLA II binds antigens, different haplotypes may alter the way in which vaccine peptides activate the immune system. [33]
Another study, which looked at 914 immune candidates in over 1600 patients who were given the HBV vaccine, found numerous single-nucleotide polymorphisms (SNPs) that were associated with inadequate levels of antibody response after vaccination, [34] with most found in the HLA genes.
However, one SNP was found in the 3 prime (3’) downstream region of the FOXP1 gene. This gene is a transcriptional repressor that plays a role in the differentiation of monocytes and the function of macrophages. [34]
Epidemiology
US statistics
Because of the implementation of routine vaccination of infants in 1992 and of adolescents in 1995, the prevalence of HBV infection has significantly declined in individuals born in the United States.
It is estimated that there are around 60,000 new cases annually. Two million or more people in the United States have chronic HBV infection; it is estimated that foreign-born persons from high endemic areas represent more than half of the total cases. [35] The prevalence of the disease is higher among Black individuals and persons of Hispanic or Asian origin.
HBV disease not only accounts for 5-10% of cases of chronic end-stage liver disease and 10-15% of cases of hepatocellular carcinoma (HCC) in the United States, it is also the dominant cause of cirrhosis and HCC worldwide.
HBV is responsible for at least 5000 US deaths annually. The prevalence is low in persons younger than 12 years born in the United States, with the subsequent increase being associated with the initiation of sexual contact (the major mode of transmission in adults, along with intravenous drug abuse [IVDA]). It is also associated with the occurrence of first intercourse at an early age. Additional risk factors, as identified in the National Health and Nutrition Examination Survey (NHANES) III, are as follows:
-
Non-Hispanic Black ethnicity
-
Cocaine use
-
High number of sexual partners
-
Divorced or separated marital status
-
Foreign birth
-
Low educational level
International statistics
Globally, chronic HBV infection affects 250-350 million people, [34, 36] with disease prevalence varying among geographic regions, from 1-20%. A higher rate exists, for example, among Alaskan Eskimos, Asian Pacific islanders, Australian aborigines, and populations from the Indian subcontinent, sub-Saharan Africa, and Central Asia. In some locations, such as Vietnam, the rate is as high as 30%. Such variation is related to differences in the mode of transmission, including iatrogenic transmission, and the patient's age at infection.
Occult hepatitis B infection appears to have an overall prevalence of 4% in Asia (3% each in East and South Asia; 9% each in West and Souteast Asia) and is associated with disease progression. [37] There is a 1% prevalence of occult infection in the general population but a 5% prevalence in high-risk groups, 9% in HIV patients; and 18% in hepatopathy patients.
The lifetime risk of HBV infection is less than 20% in low prevalence areas (generally 0.1-2%), [10] and sexual transmission and percutaneous transmission during adulthood are the main modes through which it spreads. About 12% of HBV-infected individuals live in low-prevalence areas, which include the United States, Canada, western Europe, Australia, and New Zealand. [10]
Sexual and percutaneous transmission and transmission during delivery are the major transmission routes in areas of intermediate prevalence (rate of 3-5%). These regions include Eastern and Northern Europe, Japan, the Mediterranean basin, the Middle East, Latin and South America, and Central Asia. One study reported approximately 43% of HBV-infected individuals live in South Central and West Asia, Eastern Europe, Russia, and Central and South America, with a prevalence rate of 2-7% and a lifetime HBV risk of 20-60%. [10]
In areas of high prevalence (≥8%, generally 10-20%), the predominant mode of transmission is perinatal, and the disease is transmitted vertically during early childhood from the mother to the infant. Approximately 45% of individuals infected with HBV live in high-prevalence areas, with a lifetime infection risk of over 60%, as demonstrated by the presence of hepatitis B core antibodies (anti-HBc) to hepatitis B core antigen (HBcAg) in serum. [10] Such regions include China, Southeast Asia, Indonesia, sub-Saharan Africa, Pacific Islands, parts of the Middle East, and the Amazon Basin.
Vaccination programs implemented in highly endemic areas seem to have reduced the prevalence of HBV infection. In Taiwan, for example, HBV seroprevalence declined from 10% in 1984 (before vaccination programs) to less than 1% in 1994 after the implementation of vaccination programs, and the incidence of HCC declined from 0.52% to 0.13% during the same period. [6]
The 10 genotypes of HBV (A-J) also correspond to specific geographic distributions. [22] Genotype A is more frequently found in North America, northwestern Europe, India, and Africa, whereas genotypes B and C are endemic to Asia, and genotype D predominates in Eastern Europe and the Mediterranean. Type E is found in western Africa; type F, in South America; and type G, in France, Germany, Central America, Mexico, and the United States. Type H is prevalent in Central America [10] ; type I, in Vietnam; and type J, in Japan. [22]
Race-, sex-, and age-related demographics
In the United States, Black persons have a higher prevalence of HBV disease than do Hispanics or whites. In addition, more cases of chronic HBV disease occur in males than in females.
The earlier the disease is acquired, the greater the chance a patient has of developing chronic hepatitis B infection. Infants (mainly infected through vertical transmission) have a 90% chance, children have a 25-50% chance, adults have an approximately 5% chance, and elderly persons have an approximately 20-30% chance of developing chronic disease.
Prognosis
The prognosis of patients who contract hepatitis B depends on several factors. Those with an acute hepatitis B virus (HBV) infection may spontaneously clear the virus, while others may progress to chronic infection, ultimately leading to cirrhosis and to hepatocellular carcinoma (HCC), the risk of which depends on the mode of infection, viral genotype, and presence of coinfection, among other factors. An estimated 1 million persons per year globally, including at least 5000 persons annually in the United States, die from chronic hepatitis B disease. [35]
Positive prognostic factors
Patients who have lost the hepatitis B e antigen (HBeAg) and in whom hepatitis B virus (HBV) DNA is undetectable have an improved clinical outcome, as characterized by the following:
-
Slower rate of disease progression
-
Prolonged survival without complications
-
Reduced rate of HCC and cirrhosis
-
Clinical and biochemical improvement after decompensation
Hepatocellular carcinoma
Chronic hepatitis B infection is the major contributor to the development of approximately 50% of cases of hepatocellular carcinoma (HCC) worldwide. [38] Studies indicate that the level of hepatitis B virus (HBV) DNA, which indicates viral replication, is a strong predictor for cirrhosis and HCC regardless of other viral factors. [38] Approximately 9% of patients in western Europe who have cirrhosis develop HCC due to hepatitis B infection at a mean follow-up of 73 months. The probability of HCC developing 5 years after the diagnosis of cirrhosis has been established at 6%, and the probability of decompensation is 23%.
Significant risk factors for carcinogenesis include the following:
-
Older age
-
Exposure to aflatoxins
-
Alcohol
-
Coinfection with HCV and HDV
-
Immune status
-
Genotype
-
Core and precore mutations
-
Cirrhosis
-
Thrombocytopenia
High serum viral load (ie, viral replication) that is persistently elevated over time is the most reliable indicator in predicting the development of HCC. [39]
Even the presence of hepatitis B core antibody (anti-HBc) in the absence of hepatitis B surface antigen (HBsAg) or HBV DNA is significantly related to an increased risk for HCC, although there are no recommendations for HCC surveillance in such cases unless cirrhosis is present.
The annual incidence of HCC reported in Taiwan in patients with hepatitis B infection and cirrhosis is 2.8%. The US estimates for the annual incidence of HCC in patients infected with HBV is 818 cases per 100,000 persons.
Distinct mutations associated with different HBV genotypes have been linked to an increased risk of developing advanced fibrosis and HCC. Genotype C is closely associated with HCC; this appears to be related to a higher incidence of core and precore mutations in patients older than 50 years with cirrhosis and genotype C, [22] whereas genotype B is associated with HCC development in young, noncirrhotic patients and in postsurgical relapse. [39] Various international studies additionally demonstrated a greater association of genotypes C, D, and F with cirrhosis and HCC compared to genotypes A and B.
Mortality
Familial clustering of HCC has been described among families with hepatitis B infection in Africa, the Far East, and Alaska. The cumulative probability of survival is 84% at 5 years and 68% at 10 years.
Cox regression analysis has identified 6 variables that independently correlate with overall survival for individuals with cirrhosis or HCC. These include age, albumin level, platelet count, splenomegaly, bilirubin level, and positivity for hepatitis B e antigen (HBeAg) at the time of the hepatitis B diagnosis. Based on the contribution of each of these factors to the final model, a prognostic index has been constructed that allows calculation of the estimated survival probability.
Expression of inflammatory molecules in HBV-related HCC tissues is associated with poor prognosis. [39] Imbalance between intratumoral CD8* T cells and regulatory T cells or type 1 helper T cells (Th1), and type 2 helper T-cell (Th2) cytokines in peritumoral tissues can predict the prognosis of HBV-related HCC. These molecules are also important for developing active prevention and surveillance of HBV-infected patients. [39]
Glomerulonephritis
The prognosis of renal disease in hepatitis B is related to several factors, such as age and the response to therapy. Children with membranous glomerulonephritis (MGN) have a more favorable response than adults. White persons have a better response than Asian and Black patients.
Approximately 30-60% of cases with MGN undergo spontaneous remission. However, the course of HBV-related membranous nephropathy in adults in areas in which the virus is endemic is not benign. Regardless of treatment, hepatitis B disease has a slow, but relentlessly progressive, clinical course in approximately one third of patients, resulting in progressive renal failure and necessitating maintenance dialysis therapy.
Patient Education
Patients with acute and chronic hepatitis B virus (HBV) infections should be advised that this is a blood-borne disease that can be transmitted during sexual intercourse or at the time of childbirth. Prophylaxis is strongly advised. Family members borne by the same parents should also be checked for HBV infection. The best preventative measurement is vaccination. [1]
For patient education information, see Hepatitis A (HAV, Hep A); Hepatitis B (HBV, Hep B); Hepatitis C (HCV, Hep C); Cirrhosis of the Liver; Liver Cancer; Immunization Schedule, Adults; and Childhood Immunization Schedule and Chart.
-
Hepatitis B. Under higher-power magnification, ground-glass cells may be visible in chronic hepatitis B virus (HBV) infection. Ground-glass cells are present in 50% to 75% of livers with chronic HBV infection. Immunohistochemical staining is positive for hepatitis B surface antigen (HBsAg.)
-
Hepatitis B. Liver biopsy with hematoxylin stain showing stage 4 fibrosis (ie, cirrhosis) in a patient with hepatitis B.
-
Hepatitis B. Hepatitis B virus (HBV) is a hepadnavirus, highly resistant to extremes of temperature and humidity, that invades the hepatocytes. The viral genome is a partially double-stranded, circular DNA linked to a DNA polymerase that is surrounded by an icosahedral nucleocapsid and then by a lipid envelope. Embedded within these layers are numerous antigens that are important in disease identification and progression. Within the nucleocapsid are the hepatitis B core antigen (HBcAg) and precore hepatitis B e antigen (HBeAg), and on the envelope is the hepatitis B surface antigen (HBsAg). Transmission electron micrograph (TEM) from Graham Colm and Wikipedia, licensed under the Creative Commons Attribution 3.0 Unported license.
-
Hepatitis B. Serologic course of hepatitis B virus (HBV) infection. The flat bars show the duration of seropositivity in self-limited acute HBV infection. The pointed bars show that HBV DNA and e antigen (HBeAg) can become undetectable during chronic infection. Only immunoglobulin G (IgG) antibodies to the HBV core antigen (anti-HBc) are predictably detectable after resolution of acute hepatitis or during chronic infection. Antibody to hepatitis B surface antigen (anti-HBs) is generally detectable after resolution of acute HBV infection but may disappear with time. It is only rarely found in patients with chronic infection and does not indicate that immunologic recovery will occur or that the patient has a better prognosis. ALT = alanine transaminase. (Adapted from Liaw YF, Chu CM. Hepatitis B virus infection. Lancet. 2009;373(9663):582-92.)
-
Hepatitis B. Radiologic studies may be useful in all stages of hepatitis B infection. Ultrasonography, computed tomography (CT) scanning, or magnetic resonance imaging (MRI) may exclude biliary obstruction in acute infection. In chronic disease, ultrasonograms may show nonspecific increased echogenicity of the liver parenchyma. In patients with long-standing disease, CT imaging may be used to detect cirrhosis or hepatocellular carcinoma (as shown).
-
Hepatitis B. Long-standing cirrhosis leads to progressive replacement of liver parenchyma with fibrotic tissue. Over time, the liver contracts and develops a lobulated contour. These changes are readily apparent on cross-sectional imaging. This contrast-enhanced computed tomography (CT) scan demonstrates extensive cirrhosis, as well as malignant hepatocellular lesions (arrow).
-
Hepatitis B. Liver biopsy with hematoxylin stain showing stage 4 fibrosis (ie, cirrhosis) in a patient with hepatitis B.
