Practice Essentials
Morton neuroma (interdigital neuroma), first described in 1876, is a perineural fibrosis and nerve degeneration of the common digital nerve. [1, 2] Morton neuroma, or Morton's neuroma, is not a true neuroma, although it results in neuropathic pain in the distribution of the interdigital nerve secondary to repetitive irritation of the nerve. The most frequent location is between the third and fourth metatarsals (third webspace). Other, less common locations are between the second and third metatarsals (second webspace) and, rarely, between the first and second (first webspace) or fourth and fifth (fourth webspace) metatarsals. [3] When conservative measures for Morton's neuroma are unsuccessful, surgical excision of the area of fibrosis in the common digital nerve may be curative.
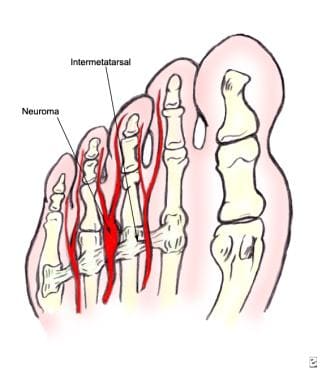 Plantar view showing the relationships between the metatarsal heads, the intermetatarsal ligament, and the neuroma.
Plantar view showing the relationships between the metatarsal heads, the intermetatarsal ligament, and the neuroma.

Episodes of pain are intermittent. Patients may experience 2 attacks in a week and then none for a year. Recurrences are variable and tend to become more frequent. Between attacks, no symptoms or physical signs occur. Two neuromas coexist on the same foot about 2-3% of the time. Other diagnoses should be considered when 2 or more areas of tenderness are present.
Symptoms of Morton’s neuroma
Symptoms of Morton’s neuroma include the following:
-
The most common presenting complaints include pain and dysesthesias in the forefoot and corresponding toes adjacent to the neuroma
-
Pain is described as sharp and burning and may be associated with cramping
-
Numbness often is observed in the toes adjacent to the neuroma and seems to occur along with episodes of pain
-
Pain typically is intermittent, as episodes often occur for minutes to hours at a time and have long intervals (ie, weeks to months) between a single or small group of multiple attacks
-
Some patients describe the sensation as "walking on a marble"
-
Massage of the affected area offers significant relief
-
Narrow, tight high-heeled shoes aggravate the symptoms
-
Night pain is reported but is rare
Workup in Morton’s neuroma
Magnetic resonance imaging (MRI), while not needed in most cases for establishing a diagnosis of Morton's neuroma, has been studied widely. [4, 5] A specificity as high as 100% has been reported.
Ultrasonography may be equivalent in sensitivity to MRI in detecting Morton's neuroma. [6, 7, 8] Indeed, a literature review by Bignotti et al indicated that ultrasonography and MRI are equally accurate for the diagnosis of Morton neuroma, with the modalities having sensitivities of 0.91 and 0.90, respectively. [9] Computed tomography (CT) scanning has been used but may not be as sensitive as MRI or ultrasonography.
Temporary elimination of pain and numbness in the associated webspace by a common digital nerve block with an anesthetic agent supports a diagnosis of Morton's neuroma.
Management of Morton’s neuroma
Treatment strategies for Morton's neuroma range from conservative to surgical management. The conservative approach to treating Morton's neuroma may benefit from the involvement of a physical therapist. The physical therapist can assist the physician in decisions regarding the modification of footwear, which is the first treatment step. The next step in conservative management is to alter alignment of the metatarsal heads.
Other possible physical therapy treatment ideas for patients with Morton's neuroma include the following:
-
Cryotherapy
-
Ultrasound
-
Deep tissue massage
-
Stretching exercises
-
Ice - To decrease associated inflammation
Phonophoresis also can be used, rather than just ultrasound, to further decrease pain and inflammation.
When conservative measures for Morton's neuroma are unsuccessful, surgical excision of the area of fibrosis in the common digital nerve may be curative. Another treatment approach involves corticosteroid injection of the Morton's neuroma. [10, 11]
Pathophysiology
Interdigital nerves are composed of communicating branches from the lateral and medial plantar nerves. At the level of the metatarsal heads, the interdigital nerve traverses inferior to the intermetatarsal ligament. At this site, the nerve may be compressed or stretched from repetitive toe flexion and extension. Other studies have shown perineural fibrosis and demyelination at the level of the metatarsal heads, indicating that the damage in Morton's neuroma may be more distal than the intermetatarsal ligament. [12]
Epidemiology
Frequency
United States
Morton's neuroma is a common disease entity of the foot.
International
The incidence of Morton's neuroma is presumed to be the same internationally as in United States.
Sex
The female-to-male ratio for Morton's neuroma is 5:1.
Age
The highest prevalence of Morton's neuroma is found in patients aged 15-50 years, but the condition may occur in any ambulatory patient.
-
Plantar view showing the relationships between the metatarsal heads, the intermetatarsal ligament, and the neuroma.
-
Neurectomy: typical incision location.
-
Neurectomy: superficial exposure.
-
Neurectomy: deeper dissection.
-
Neuroma and adherent fibrofatty tissue.
