Background
Posterior cerebral artery (PCA) stroke is less common than stroke involving the anterior circulation. An understanding of PCA stroke phenomenology and mechanisms requires knowledge of neurovascular anatomy and of the structure-function relationships of this region of the brain. Identifying mechanisms of stroke is essential so that appropriate preventive therapies may be instituted. This article provides an overview of PCA stroke and focuses exclusively on stroke of arterial origin involving the PCA territory (see the images below). (See Anatomy, Pathophysiology, Etiology, Treatment, and Medication.)
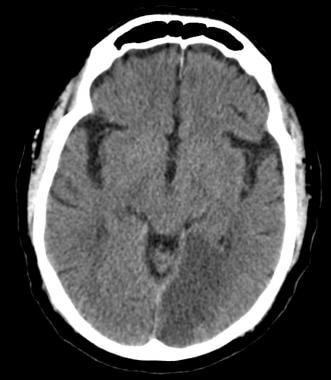 Unenhanced head computed tomography (CT) scan demonstrating a subacute L posterior cerebral artery (PCA) infarct.
Unenhanced head computed tomography (CT) scan demonstrating a subacute L posterior cerebral artery (PCA) infarct.
 Computed tomography (CT) scan of the brain showing hypodense areas in the right occipital lobe consistent with a recent posterior cerebral artery (PCA) ischemic infarct.
Computed tomography (CT) scan of the brain showing hypodense areas in the right occipital lobe consistent with a recent posterior cerebral artery (PCA) ischemic infarct.
Ischemic strokes occur when blood cannot flow to cerebral structures. Neuron metabolism tolerates a brief period of interrupted oxygen and glucose delivery. Cell death is imminent after approximately 6 minutes of halted blood circulation. Large cortical neurons are especially sensitive to ischemia. Infarcts include a central area, or umbra, of highly concentrated cell death, surrounded by a penumbra of tissue containing stunned cells that may recover, assuming circulation is reestablished or produced through nearby collaterals. (See Pathophysiology and Etiology.)
Patients who have sustained PCA strokes present with an interesting and diverse spectrum of neurologic symptoms. The most common long-term sequelae of PCA strokes are visual and sensory deficits. In general, patients with PCA distribution strokes exhibit less overall chronic disability than do those with anterior cerebral, middle cerebral, or basilar artery infarctions. (See Prognosis and Presentation.)
Active neurorehabilitation of patients following cerebrovascular accident is essential because evidence suggests that prolonged neural plasticity follows stroke. Active intervention, especially by a team of rehabilitation specialists, is beneficial, increasing the probability of the patient's achieving maximal independence in activities of daily living (ADL). The role of the physiatric clinician on the neurorehabilitation team is to avert medical complications and facilitate integration of the various therapeutic services. (See Treatment.)
Complications
Stroke complications include the following (see Prognosis, Presentation, and Workup):
-
Recurrent ischemic event [1]
-
Hemorrhage into infarcted brain tissue
-
Stroke-associated epilepsy
-
Anticoagulation-associated intracranial, gastrointestinal, or retroperitoneal hemorrhaging
-
Urinary tract and pulmonary infections
-
Skin breakdown
-
Depression
-
Chronic pain
-
Dyskinesia and dystonia
Anatomy
Common neurovascular anatomy
The posterior cerebral arteries (PCAs) are paired vessels, usually arising from the top of the basilar artery and curving laterally, posteriorly, and superiorly around the midbrain. The PCAs supply parts of the midbrain, subthalamic nucleus, basal nucleus, thalamus, mesial inferior temporal lobe, and occipital and occipitoparietal cortices. In addition, the PCAs, via the posterior communicating arteries (PCOM), may become important sources of collateral circulation for the middle cerebral artery (MCA) territory.
Various nomenclature methodologies have been used to describe PCA vascular anatomy. The PCA is divided into P1 and P2 segments by the PCOM. Penetrating branches to the mesencephalon, subthalamic, basal structures, and thalamus arise primarily from the P1 segment and the PCOM. These penetrating arteries include the thalamogeniculate, splenial (posterior pericallosal artery), and lateral and medial posterior choroidal arteries.
The P2 segment bifurcates into the posterior temporal artery and the internal occipital artery. The posterior temporal artery further divides into anterior, middle, posterior, and hippocampal branches. The internal occipital artery divides into calcarine and occipitoparietal branches.
Anatomic localization of the point of vascular occlusion in PCA infarcts may be simplified into the following 2 categories: (1) deep or proximal PCA strokes, causing ischemia in the thalamus and/or midbrain, as well as in the cortex; and (2) superficial or distal PCA strokes, involving only cortical structures. [2, 3]
Normal variants of neurovascular anatomy
The fetal PCA variant is seen in up to 30% of people, with incidence depending on how the variant is defined. The variant occurs when the P1 segment is congenitally absent or markedly hypoplastic and the PCA arises directly from the ipsilateral internal carotid artery (ICA). This can have diagnostic importance, in that PCA territory stroke may be caused by atheromatous disease of the anterior circulation (ie, ipsilateral carotid bulb atheroma).
The central artery of Percheron variant is uncommon and occurs when the bilateral medial thalamic/rostral midbrain perforators arise from a single trunk from one P1 segment. Occlusion may result in bilateral paramedian thalamic and rostral midbrain infarction. This is an example in which a single cerebral artery supplies bilateral structures.
Pathophysiology
Major PCA stroke syndromes
The major posterior cerebral artery (PCA) stroke syndromes (many of which occur concomitantly) include the following:
-
Paramedian thalamic infarction
-
Visual field loss
-
Visual agnosia
-
Balint syndrome
-
Prosopagnosia
-
Palinopsia, micropsia, and macropsia
-
Disorders of reading
-
Disorders of color vision
-
Memory impairment
-
Motor dysfunction
Paramedian thalamic infarction
This syndrome results from bilateral medial thalamic infarction. The presentation in these patients varies from lethargic to obtunded to comatose, but some patients may be agitated and may have associated hemiplegia or hemisensory loss. Occasionally, the cranial nerve III nucleus is involved, with resultant ophthalmoplegia.
Patients may take days to weeks to recover and seem to be in a sleeplike state. Although alertness generally returns, prognosis for good functional recovery is poor because of severe memory dysfunction.
The syndrome may result from a “top of the basilar” artery embolus. The artery of Percheron may be involved.
Visual field loss
Unilateral infarction produces homonymous hemianopia. Sparing of the macula is encountered frequently in infarction of the occipital lobes due to PCA occlusion. Macular sparing may be caused by collateral vascular supply to the macular region or by the very large macular representation in the occipital cortex; additionally, bilateral representation of macular vision has been suspected.
Bilateral infarctions of the occipital lobes produce varying degrees of cortical blindness depending on the extent of the lesion. Patients often exhibit Anton syndrome, a state in which they fervently believe they can see when they cannot. Patients may describe objects that they have not seen previously in exquisite detail, completely in error and oblivious to that error.
Another intriguing phenomenon is blindsight. Although cortically blind, patients can respond to movement or sudden lightening or darkening of their environment.
Infarction of the lateral geniculate nucleus may produce hemianopia, quadrantanopia, or sectoranopia. The vascular supply is dual; the anterior choroidal artery supplies the anterior hilum and anterolateral areas, and the posterior choroidal artery supplies the rest. Occlusion of the posterior choroidal artery may produce a distinct syndrome of hemianopia, hemidysesthesia, and memory disturbance due to infarction of the lateral geniculate, fornix, dorsomedial thalamic nucleus, and posterior pulvinar.
Visual agnosia
This refers to a lack of recognition or understanding of visual objects or constructs. It is a disorder of higher cortical function.
The strict diagnosis of visual agnosia requires intact visual acuity and language function. Most patients have bilateral lesions, sparing the visual cortex but disrupting or disconnecting visual information; this interferes with the information’s ability to reach parts of the visual association cortex, for reference to visual memories. The patient with visual agnosia can recognize objects presented to a nonvisual sensory system; for example, the patient can identify keys by palpating them or hearing them jingle.
True visual agnosia has been divided into apperceptive and associative subtypes. In apperceptive visual agnosia, patients cannot name objects presented to them, draw objects from memory, or identify or match objects, yet they can see and avoid obstacles when ambulating and detect subtle changes in light intensity.
In associative agnosia, patients can draw objects to command and can match them or point to them, but they cannot name them. Patients can see shapes and reproduce them in drawings, yet they do not recognize the identity of objects.
Balint syndrome
This may occur with bilateral parieto-occipital infarction, most often in the watershed between the PCA and middle cerebral artery (MCA) territories. It is a triad of visual simultanagnosia, optic ataxia, and apraxia of gaze, which are characterized as follows:
-
Visual simultanagnosia - Implies an inability to examine a scene and integrate its parts into a cohesive interpretation; a patient can identify specific parts of a scene but cannot describe the entire picture
-
Optic ataxia - Implies a loss of hand-eye coordination such that reaching or performing a motor task under visual guidance is clumsy and uncoordinated
-
Apraxia of gaze - A misnomer describing a supranuclear deficit in the ability to initiate a saccade on command
Prosopagnosia
Prosopagnosia refers to an inability to recognize faces. Typically, this deficit results from bilateral lesions of the lingual and fusiform gyri; however, cases of unilateral nondominant-hemisphere lesions resulting in prosopagnosia have been reported.
Palinopsia, micropsia, and macropsia
These are illusory phenomena that are of uncertain pathophysiology. Palinopsia describes the persistence of a visual image for several seconds to days in a partially blind hemifield. Micropsia and macropsia describe situations where objects appear smaller or larger than expected.
Disorders of reading
Pure alexia may result from infarction of the dominant occipital cortex. Words are treated as if they are from a foreign language. Patients may retain the ability to formulate a word and its meaning if spelled out to them orally or if they trace the letters with their hand. Patients may then learn to read, albeit terribly slowly, in a letter-by-letter fashion, being unable to integrate multiple letter groups.
Classic alexia without agraphia was described by Dejerine in the late 19th century. In his case study, he emphasized a left occipital cortex lesion and also infarction of the splenium of the corpus callosum, which disconnected fibers from the right occipital lobe, preventing them from reaching the angular gyrus.
Rarely, the dominant-hemisphere posterior temporal lobe is supplied by the PCA. Damage to this area results in a Wernicke-type aphasia with associated dyslexia and right hemianopia due to concomitant left occipital infarction.
Disorders of color vision
Lesions of the lingual gyrus in the inferior occipital lobe may produce disorders of color perception. Testing with Ishihara plates reveals a deficit. Colors may be described as washed out or gray. This deficit usually occurs only in the contralateral visual field and is called hemiachromatopsia.
A related problem is color anomia, also called color agnosia, in which patients can perceive and match colors but cannot associate them with the proper color names.
Memory impairment
Infarction of the medial temporal lobe, fornices, or medial thalamic nuclei may result in permanent anterograde amnesia. Although traditionally, bilateral infarction has been thought to be required for amnesia, memory functions may be lateralized such that infarction of left-sided structures may have a more lasting impact on verbal function.
Older patients frequently have lasting short-term memory impairment from unilateral PCA territory infarction. In addition, diffusion-weighted Imaging in patients with transient global amnesia has demonstrated lesions in unilateral temporal lobes resulting in temporary amnesia.
Motor dysfunction
When the blood supply to the cerebral peduncles arises from perforators of the P1 segment, infarction may occur, resulting in hemiplegia or hemiparesis. The clinical syndrome is no different from capsular infarction but often includes concomitant hemianopia because of occipital lobe involvement. The syndrome may mimic a large middle cerebral artery (MCA) infarction.
Etiology
Ischemic stroke occurs when a region of cerebral blood flow is suddenly limited. This may occur by vessel occlusion or by relatively low flow. The rate of neuronal death varies with blood flow, variability in individual anatomy and collateralization, and inherent cerebral capacities (ie, some cerebral regions are more resistant than others).
Cerebral blood flow (CBF) rates of less than 20 mL/100 g/min may produce infarction depending on these individual differences plus the duration of oligemia, with lower CBF rates (< 10 mL/100 g/min) requiring less time to produce irreversible injury. Rapid restoration of blood flow is the most effective means of preserving brain tissue.
The mechanism of stroke involving the posterior cerebral artery (PCA) territory is variable. Common etiologic considerations for PCA stroke include the following:
-
Cardiogenic embolization
-
Atheromatous disease of proximal vessels - Results in occlusion and/or artery-to-artery embolization
-
Dissection of proximal vessels - Results in occlusion and/or artery-to-artery embolization
-
Intrinsic PCA atheromatous disease
Less common etiologies include migrainous cerebral infarction (which preferentially affects the PCA distribution), anterior circulation disease (when fetal PCA variant is present), hypercoagulable disorders, illicit substance use, vasculitides, and fibromuscular dysplasia.
Cardioembolism
Cardioembolism, which may arise from a number of different mechanisms, is the most common cause of PCA stroke. The most common cause of cardioembolism is atrial fibrillation, in which emboli form due to vascular stasis, frequently within the atrial appendage. Atrial fibrillation often represents a high-risk etiology for PCA stroke recurrence, particularly if the patient has other identified risk factors, including congestive heart failure, hypertension, age older than 75 years, diabetes mellitus, and prior stroke or transient ischemic attack. These risk factors are the basis of the CHADS2 score, which estimates the risk of recurrent stroke and suggests the benefit of oral anticoagulation based on score. [4]
Other sources of cardiogenic embolism include a mural thrombus on a hypokinetic wall segment (eg, postmyocardial infarction, dilated cardiomyopathy, ventricular aneurysm), endocarditis (bacterial, marantic, Libman-Sacks), prosthetic heart valve thrombosis, rheumatic heart disease, and paradoxical embolism via a patent foramen ovale or atrial septal defect.
Embolism may also arise from aortic arch atheroma. This entity has been elucidated by transesophageal echocardiography, which is more effective than transthoracic echocardiography in examining the aortic arch. Thickness of plaque greater than 4 mm or the presence of a mobile thrombus is strongly associated with stroke.
Proximal vertebrobasilar artery disease
Atheromatous disease may be found within the vertebral artery in patients with posterior circulation ischemia and may result in stenosis or occlusion of that proximal vessel. This may result in hypoperfusion or artery-to-artery embolism involving the PCAs.
Dissection of the vertebral arteries may result from trauma or occur spontaneously and result in arterial embolization. The vertebral arteries are uniquely prone to dissection due to their intracanalicular course within the vertebral bodies. (Some authorities have expressed concern that chiropractic manipulation of the neck may cause vertebral artery dissection.) PCA stroke secondary to vertebral artery dissection may occur when thrombus forms at an intimal tear and embolizes distally or when the dissection results in vessel stenosis/occlusion, with subsequent vascular stasis and embolism.
Intrinsic basilar atheromatous disease may result in misery perfusion or artery-to-artery embolization in the PCA distribution.
Intrinsic PCA stenosis from atherosclerosis is a less common, but recognized, cause of stroke.
Migrainous cerebral infarction
Migraine represents a particular challenge in stroke medicine. Migraine typically affects the posterior circulation, although the mechanisms by which stroke occurs are not known. However, numerous postulated mechanisms exist.
Migraine alone commonly results in focal neurologic deficits, which may include visual loss, language disturbances, vertigo, nausea/vomiting, and other symptoms suggestive of posterior circulation disease (frequently known as complicated or basilar migraine). Furthermore, stroke in the posterior circulation distribution is more commonly associated with headache, occurring in approximately 30% of patients. Therefore, distinguishing between complicated migraine, migrainous cerebral infarction, and stroke with headache may be challenging.
Epidemiology
An estimated 5-10% of ischemic strokes in the United States involve the posterior cerebral artery (PCA) or its branches. While stroke is the third leading cause of death in the United States and the leading cause of adult disability, death from PCA stroke is uncommon and would more likely occur in the setting of concomitant brainstem infarction.
Race-, sex-, and age-related demographics
Stroke is more common in African Americans than in white or Hispanic populations in the United States.
Published data from the Tufts New England Medical Center posterior circulation stroke registry document that 58% of patients are male and 42% are female, with the mean age of stroke being 61.5 years. [5] Stroke incidence dramatically increases in the elderly population secondary to cardiovascular disease.
Prognosis
Mortality associated with isolated posterior cerebral artery (PCA) stroke is low; therefore, the prognosis is generally good. Visual field deficits improve to varying degrees; however, they may be permanent and associated with morbidity. Some neuropsychological deficits may improve with time but are also associated with morbidity.
On average, patients with posterior cerebral artery (PCA) stroke sustain minimal or no chronic motor disability. These patients are usually able to adapt to their visual deficit so that many ADL tasks are manageable.
Among young stroke victims, 30-70% return to work, with the higher fraction being men and those educated beyond high school.
In a single-blind cluster, randomized, controlled trial of stroke patients in acute stroke units, there was a decreased likelihood of death or dependence by 90 days after hospital admission in patients who received a multidisciplinary intervention focusing on evidence-based management of fever, hyperglycemia, and swallowing dysfunction, despite the severity of the stroke. [6]
Morbidity and mortality
Overall, the risk of death in patients with posterior cerebral artery (PCA) stroke is approximately 5% in the acute hospital setting. Most deaths occur in patients with deep or proximal PCA infarctions, particularly those involving bilateral midbrain and thalamic structures. Otherwise, most PCA infarctions result in chronic visual deficits (84%), sensory abnormalities (17%), and motor weakness (6%), as documented in the Brandt et al series of 127 patients. [7]
Recovery of visual field deficits may be limited; patients may be unable to drive or read, resulting in major limitations in their quality of life, despite normal motor function.
Other neuropsychological deficits may include prosopagnosia (inability to recognize faces), visual agnosia, amnesia, and alexia without agraphia. Rarely, PCA stroke results in infarction of the ipsilateral cerebral peduncle with resultant hemiplegia. Thalamic involvement can also produce contralateral sensory loss or chronic pain syndromes.
Patient Education
At discharge, all patients who have had a stroke should be counseled about the symptoms and signs of acute stroke. They should know that the major symptoms of stroke include the following:
-
Sudden loss of vision
-
Sudden loss of ability to speak or understand speech
-
Sudden weakness on 1 side of the body
-
Sudden loss of sensation on 1 side of body
-
Sudden onset of incoordination
Since a delay in receiving emergency care is the major reason why patients cannot be treated with thrombolytic therapy, patients and their caregivers must be taught what to do if a stroke occurs. Patients should be instructed to call an ambulance (ie, call 911) if they or their friends/relatives suffer from any of the above symptoms.
For patient education information, see the Brain and Nervous System Center and the Cholesterol Center, as well as Stroke, High Cholesterol, and Cholesterol FAQs.
-
Unenhanced head computed tomography (CT) scan demonstrating a subacute L posterior cerebral artery (PCA) infarct.
-
Unenhanced head computed tomography (CT) scan demonstrating hemorrhagic conversion of an ischemic stroke, approximately 72 hours after symptom onset.
-
Brain magnetic resonance imaging (MRI) scan demonstrating acute stroke. Diffusion restriction is seen on diffusion-weighted imaging.
-
Magnetic resonance (MR) angiogram demonstrating bilateral fetal posterior cerebral artery (PCA) variants (black arrows) with the basilar artery terminating in bilateral superior cerebellar arteries (blue arrows).
-
Digital subtraction angiogram demonstrating an acute L posterior cerebral artery (PCA) occlusion (red arrow) following balloon-assisted coiling of a basilar tip aneurysm.
-
Digital subtraction angiogram demonstrating revascularization of acute L posterior cerebral artery (PCA) occlusion (red arrow) during a balloon-assisted basilar tip aneurysm revascularization with use of balloon angioplasty.
-
Computed tomography (CT) scan of the brain showing hypodense areas in the right occipital lobe consistent with a recent posterior cerebral artery (PCA) ischemic infarct.
