Practice Essentials
Carcinoid tumors are of neuroendocrine origin and derived from primitive stem cells in the gut wall, especially the appendix. [1, 2, 3, 4] They can be seen in other organs, [5] including the lungs, [6] mediastinum, thymus, [7] liver, bile ducts, [8] pancreas, [9] bronchus, [10, 11] ovaries, [12] prostate, [13] and kidneys (see the image below). While carcinoid tumors have a tendency to grow slowly, they have a potential for metastasis.
 Distribution of carcinoid tumors.
Distribution of carcinoid tumors.
Signs and symptoms
Signs and symptoms of carcinoid tumors vary greatly. Carcinoid tumors can be "nonfunctioning" presenting as a tumor mass or "functioning" i.e. producing several biopeptides causing carcinoid syndrome. The sign and symptoms of a "nonfunctioning" tumor depend on the tumor location and size as well as on the presence of metastases. Therefore, findings range from no tumor-related symptoms (most carcinoid tumors) to full symptoms of carcinoid syndrome (primarily in adults). At times, the tumor is found as an incidental finding in a histopathologic examination. [14] Due to their vague and intermittent symptoms, diagnosis of carcinoid tumors may be delayed, especially in children, in whom the tumor is rare and the diagnosis is unexpected.
Signs and symptoms seen in larger tumors may include the following:
-
Periodic abdominal pain: Most common presentation for a small intestinal carcinoid; often associated with malignant carcinoid syndrome
-
Cutaneous flushing: Early and frequent (94%) symptom; typically affects head and neck; often associated with an unpleasant warm feeling, itching, rash, sweating, palpitation, upper-body erythema and edema, salivation, diaphoresis, lacrimation, and diarrhea
-
Diarrhea and malabsorption (84%): Watery, frothy, or bulky stools, gastrointestinal (GI) bleed or steatorrhea; may or may not be associated with abdominal pain, flushing, and cramps
-
Cardiac manifestations (60%): Valvular heart lesions, fibrosis of the endocardium; may lead to heart failure with tachycardia and hypertension
-
Pellagra with scale-like skin lesions, diarrhea and mental disturbances
-
Carcinoid crisis can be the most serious symptom of carcinoid tumors and can be life-threatening. It can occur suddenly, after stress, or following chemotherapy and anesthesia. [17]
Classification
Carcinoid tumors generally are classified based on the location in the primitive gut that gives rise to the tumor, as follows:
-
Foregut carcinoid tumors: Divided into sporadic primary tumors (lung, bronchus, stomach, proximal duodenum, pancreas) and tumors secondary to achlorhydria
-
Midgut carcinoid tumors: Derived from the second portion of the duodenum, the jejunum, the ileum, and the right colon
-
Hindgut carcinoid tumors: Includes the transverse colon, descending colon, and rectum
See Clinical Presentation for more detail.
Carcinoid tumors are divided into well-differentiated (i.e., low grade [ENETS G1] and intermediate grade [ENETS G2]) and poorly differentiated (i.e., high grade [ENETS G3]). Classification based on the extent of the tumor are local, regional and distant spread. (See grading and staging)
Diagnosis
The etiology of carcinoid tumors is not known, but genetic abnormalities are suspected. Reported chromosomal abnormalities include changes in chromosomes, [18, 19] such as loss of heterogeneity, and numerical imbalances. The diagnosis is sometimes made because of unrelated findings, such as anemia, endocrine disease, or autoimmune disorders.
Laboratory testing
Laboratory diagnosis of carcinoid tumors depends on the identification of the characteristic biomarkers of the disease. [20, 21, 22] Measurement of biogenic amine levels (eg, serotonin, 5-hydroxyindoleacetic acid [5-HIAA], chromographin-A, catecholamines, histamine) and its metabolites in the platelets, plasma, and urine of patients can be helpful in making the diagnosis.
Imaging studies
Depending on the location of the tumor and metastasis, a combination of the following imaging modalities may be used to evaluate suspected carcinoid tumors:
-
Plain radiography
-
Upper and lower GI radiography with oral contrast agents
-
Computed tomography scanning
-
Magnetic resonance imaging
-
Angiography
-
Ultrasound including endoscopic ultrasound
-
Positron emission tomography scanning
-
Radionuclide imaging with somatostatin analogs attached to the radioactive tracer
-
Technetium-99m bone scanning
Procedures
Endoscopic procedures, such as the following, may be used for biopsy and diagnosis:
-
Bronchoscopy
-
Esophagogastroscopy
-
Gastroscopy
-
Colonoscopy
See Workup for more detail.
Management
Surgery
If feasible, the treatment of choice for carcinoid tumors is surgical excision. The surgical technique may vary according to the type or location of the tumor. When total resection is not possible, debulking may provide symptomatic relief. In selected cases, cryotherapy can be effective.
Chemotherapy
If metastasis of carcinoid tumor has occurred and in cases where surgical excision is not suitable, consider treatment with currently recommended chemotherapeutic agents, individually or in combination, such as the following:
-
Alkylating agents
-
Doxorubicin
-
5-Fluorouracil
-
Dacarbazine
-
Actinomycin D
-
Cisplatin
-
Etoposide
-
Streptozotocin
-
Interferon alfa
-
Somatostatin analogs with a radioactive load
-
Experimental agents such as 177Lu-Dotatate [25]
See Treatment for more detail.
Background
Origin and general involvement and presentation
Carcinoid tumors are derived from primitive stem cells in the gut wall but can be seen in other organs, [5] including the lungs, [6] mediastinum, thymus, [7] liver, pancreas, bronchus, ovaries, [12] prostate, [13] and kidneys. [26] In children, most tumors occur in the appendix and are benign and asymptomatic. While very rare in children, bronchial carcinoid tumors are the most common primary pulmonary neoplasm in the pediatric age group. [9]
Most carcinoid tumors are slow growing and indolent without symptoms. Nevertheless, aggressive and metastatic disease (eg, to the brain) does occur. Even tumors in the appendix can metastasize. [27, 28] Depending on the size and location, carcinoid tumors can cause various symptoms, including carcinoid syndrome. [17] Carcinoid tumors of the ileum and jejunum, especially those larger than 1 cm, especially in adults, are most prone to produce this syndrome.
Classification
Carcinoid tumors generally are classified based on the location in the primitive gut (ie, foregut, midgut, hindgut) that gives rise to the tumor.
Foregut carcinoid tumors are divided into sporadic primary tumors and tumors secondary to achlorhydria. The term sporadic primary foregut tumor encompasses carcinoids of the lung, bronchus, stomach, proximal duodenum, and pancreas.
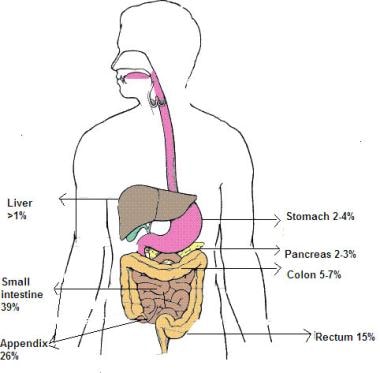
Midgut tumors are derived from the second portion of the duodenum, the jejunum, the ileum, and the right colon. The image below shows the distribution of carcinoid tumors in adults.
Distribution of carcinoid tumors.
These account for 60-80% of all carcinoid tumors (especially those of the appendix and distal ileum) in adults and are also seen in children. [29] Appendicular carcinoid tumors are most common. [30, 31] In children, more than 70% of these tumors occur at the tip of the appendix and are often an incidental finding in appendectomy specimens. In one study, carcinoid tumors were found in 0.169% of 4747 appendectomies. [32] Overall, based on retroactive studies, up to 0.35% of children undergoing appendectomy have appendiceal carcinoid tumors. [14, 33] Bulky tumors are relatively rare and require somewhat extensive cecectomy or, when tumor infiltration is beyond the cecum, ileocecal resection. [34, 35, 31]
Hindgut carcinoid tumors include those of the transverse colon, descending colon, and rectum.
Carcinoid tumors can also arise from the Meckel diverticulum, cystic duplications, and the mesentery. Each of these entities has distinctive clinical, histochemical, and secretory features. For example, foregut carcinoids are argentaffin negative and have low serotonin content but secrete 5-hydroxytryptophan (5-HTP), histamine, and several polypeptide hormones. These tumors can metastasize to bone and may be associated with atypical carcinoid syndrome, acromegaly, Cushing disease, other endocrine disorders, telangiectasia, or hypertrophy of the skin in the face and upper neck.
Midgut carcinoids are argentaffin positive and can produce high levels of serotonin 5-hydroxytryptamine (5-HT), kinins, prostaglandins, substance P (SP), and other vasoactive peptides. These tumors have a rare potential to produce corticotropic hormone (previously adrenocorticotropic hormone [ACTH]). Bone metastasis is uncommon.
Hindgut carcinoids are argentaffin negative and rarely secrete 5-HT, 5-HTP, or any other vasoactive peptides. Therefore, they do not produce related symptomatology. Bone metastases are not uncommon in these tumors.
Pathophysiology
Carcinoid tumors are of neuroendocrine origin and derived from primitive stem cells, which can give rise to multiple cell lineages. [36] In the intestinal tract, these tumors develop deep in the mucosa, growing slowly and extending into the underlying submucosa and mucosal surface. This results in the formation of small firm nodules, which bulge into the intestinal lumen. These tumors have a yellow, tan, or gray-brown appearance that can be observed through the intact mucosa. The yellow color is a result of cholesterol and lipid accumulation within the tumor. Tumors can have a polypoid appearance and occasionally become ulcerated. With expansion and infiltration through the submucosa into the muscularis propria and serosa, carcinoid tumors can involve the mesentery. Metastases to the mesenteric lymph node and liver, ovaries, peritoneum, and spleen can occur.
Upon histologic examination, carcinoid tumors have 5 distinctive patterns: (1) solid, nodular, and insular cords; (2) trabecular or ribbons with anastomosing features; (3) tubules and glands or rosettelike patterns; (4) poorly differentiated or atypical patterns; and (5) mixed patterns. A combination of these patterns is often observed. Tubules can contain mucinous secretions, and individual tumor cells can contain mucin-positive material, which includes the various acidic and neutral intestinal mucin. Tumors rarely have eosinophilic stroma. Capillaries are often prominent. Cells are uniformly round or polygonal with a central nucleus and punctate chromatin as well as small nucleoli and infrequent mitosis. The cytoplasm can be slightly acidophilic, basophilic, or amphophilic. Eosinophilic granules may be present. Immunohistochemically, these tumors have a strong positive reaction to keratin and neuroendocrine markers. These include chromogranin and synaptophysin.
In midgut carcinoids, cells are arranged in closely packed, round, regular, monomorphous masses. In the appendix, carcinoids appear as discrete yellow nodules in the lumen. Lesions associated with diffuse wall thickening are relatively uncommon. Carcinoid tumors commonly affect the tip of the appendix. Most carcinoid tumors invade the wall of the appendix, and lymphatic involvement is nearly universal. About 75% of patients have evidence of peritoneal involvement. However, only a few patients have regional or distant dissemination. The size of the tumor can be correlated with outcome of the disease; tumors smaller than 1.5 cm in diameter (after formalin fixation) rarely result in distant metastases or recurrences.
Carcinoid tumors can be associated with concentric and elastic vascular sclerosis that results in obliteration of vascular lumina and ischemia. A common finding is elastosis and fibrosis that surround nests of the tumor cells and that result in matting of the involved tissues and lymph nodes. Fibroblastic proliferation may result from the stimulation of fibroblast cells by growth factor. This stimulation may be as a result of a local release of tumor growth factor (TGF)-beta, beta–fibroblast growth factor (beta-FGF), and platelet-derived growth factor.
Other products of carcinoid tumors include the following:
-
Acid phosphatase
-
Alpha-1-antitrypsin
-
Amylin
-
Atrial natriuretic polypeptide
-
Calbindin-D28k
-
Catecholamines
-
Dopamine
-
Fibroblast growth factor
-
Gastrin
-
Gastrin-releasing peptide (bombesin)
-
Glucagon, glicentin
-
5-Hydroxyindoleacetic acid (5-HIAA)
-
5-Hydroxytryptamine (5-HT)
-
Histamine
-
Insulin
-
Kallikrein
-
Kinins
-
Motilin
-
Neuropeptide
-
Neurotensin
-
Pancreastatin
-
Pancreatic polypeptide
-
Platelet-dermal growth factor
-
Prostaglandins
-
Pyroglutamyl-glutamyl-prolinamide
-
Secretin
-
Serotonin
-
Somatostatin (ie, SRIF)
-
Tachykinins
-
Neuropeptide K
-
Neuropeptide A
-
Substance P (SP)
-
Transforming growth factor-beta
-
Vasoactive intestinal polypeptide (VIP)
Classic carcinoid tumor cells are argentaffinic and argyrophilic. At present, immunostain and hormonal markers are used for diagnosis. Carcinoid tumors of mediastinum can be misclassified as thymoma.
Carcinoids may have somatostatin receptors. Five identified somatostatin receptors are members of the G-protein receptor family. Five distinct genes on chromosomes 11, 14, 16, 17, and 20 encode somatostatin receptors. Somatostatin receptors are used to advantage for diagnosing and treating this disease.
Carcinoid tumors have high potential for metastasis. These cells produce a significant amount of beta-catenin, which enables the tumor cell adhesion, thus promoting metastasis. Induction of Raf1 results in decreased adhesion of carcinoid cells and may be important in the metastatic process. [37]
Etiology
The etiology of carcinoid tumors is not known, but genetic abnormalities, especially in pediatric pancreatic neuroendocrine tumors, [9] are suspected. Reported chromosomal abnormalities include changes in chromosomes, such as loss of heterogeneity, and numerical imbalances.
-
MEN 1 is an autosomal dominant disorder characterized by the occurrence of multiple tumors, particularly in the pancreatic islets, parathyroid and pituitary glands, and neuroendocrine tumors. [38]
Germline mutations in the MEN 1 gene can be identified in the general population.
Multiple carcinoid tumors occurring in association with MEN 1 have been reported. [39]
Although the MEN 1 gene locus is known to be involved in neuroendocrine tumors, the genetic events underlying the neoplastic process are basically unknown.
Familial cases other than those associated with MEN 1 are rare, but do occur. [40]
In several studies, loss of heterozygosity (LOH) at the MEN 1 locus has been reported. [41, 42, 43, 44, 45, 46]
Genetic abnormalities involving chromosome 11 are most common. These can be seen as a part of MEN 1 or independent of MEN 1 abnormalities. [45, 46] In 5 of 9 typical carcinoid tumors of the lung, 3 distinct regions of allelic loss were identified at bands 11q13.1 (D11S1883), 11q14.3-11q21 (D11S906), and 11q25 (D11S910).
Some atypical carcinoids have LOH at band 11q13 between markers PYGM and D11S937 and at bands 11q14.3-11q21 (D11S906), 11q23.2-23.3 (D11S939), and 11q25 (D11S910).
The region of band 11q13 bearing the MEN 1 gene can also be affected in some atypical carcinoid tumors more than it is in typical carcinoid tumors. Therefore, band 11q13 appears to be important in these tumors. Aggressive atypical carcinoid tumors, defined by high mitosis, vascular invasion and organ metastasis, also appear to have more allelic losses than other tumors.
The MEN 1 gene is located on band 11q13 and likely functions as a tumor-suppressor gene. In a study of 46 sporadically occurring tumors, 78% had LOH at this site, with almost the entire allele missing in 5 patients. In the remaining cases, genetic heterozygosity had a discontinuous pattern. Some have postulated that sporadically occurring carcinoid tumors evolve after inactivation of a tumor-suppressor gene on chromosome 11 as well as genetic mutations that affect DNA-mismatch repair.
-
Gastric neuroendocrine tumors are associated with a high incidence of LOH at chromosomal arm 8p and a lowered frequency of LOH at 7q. Chromosomal arm 8p is suspected to be the possible location of the tumor-suppressor gene associated with the genesis of gastric neuroendocrine tumors. In one study, two out of five patients with pancreatic neuroendocrine tumors had Von Hippel-Lindau disease and two others were diagnosed with multiple endocrine neoplasia type1. [47]
-
Numerical imbalances of chromosomes have been observed in carcinoid tumors.
In one study of midgut carcinoids, numerical changes were found in 16 of the 18 tumors.
The most common aberrations were losses of bands 18q22-qter (67%), 11q22-q23 (33%), and 16q21-qter (22%) with a gain of band 4p14-qter (22%). Rates of alterations were substantially more common in metastases than in primary tumors.
-
Losses of chromosomal arms 18q and 11q were found in the primary tumors and metastases, whereas loss of 16q and gain of 4p were present only in metastases.
-
HER2 expression has been reported in intestinal, but not gastric, tumors. [48]
-
Some studies have implicated homeobox gene Hoxc6 through activation of the oncogenic activator protein-1 signaling pathway and via interaction with JunD in carcinoid tumorigenesis. [49] Mutation in the home domain of Hoxc6, which blocks this interaction, results in inhibition of the carcinoid tumor cell proliferation in vitro.
-
One postulate is that loss of chromosomal arms 18q and 11q may represent an early event and that the loss of 16q and gain of 4p occur as a late event in midgut carcinoids.
Epidemiology
United States statistics
Carcinoids are the most common neuroendocrine tumors, with an estimated 1.5-1.9 clinical cases per 100,000 population. The incidence in autopsy cases is higher at 650 cases per 100,000 population. An estimated 8000 gastrointestinal (GI) tract–related carcinoid tumors are diagnosed each year in the United States. [50] A study by Zeineddin et al found that the prevalence of neuroendocrine tumors was 1:271 among children undergoing appendectomy for acute appendicitis. [51]
Evidence in adults suggests that overall incidence of carcinoid tumors has been steadily increasing. [52, 53] While not entirely clear, it is speculated that this increase is due to more universal utilization of proton pump inhibitors. The exact incidence in children is not known. Most tumors occur in adults and are rare in children.
Historically, prior to availability of improved diagnostic techniques, distant metastasis was reported in 12.9% range. A retrospective cohort study by Kasumova et al reported that out of 10,752 patients, 12.7% were diagnosed with carcinoid tumors, 84.7% with nonfunctional and 2.6% with functional pancreatic neuroendocrine tumors. The incidence of carcinoid tumors rose from 36 (5.7%) diagnosed in 2004 to 497 (27.7%) in 2013. Overall survival was significantly longer for carcinoid compared with functional and nonfunctional tumors, with 5-year survival rates of 63.1%, 58.3%, and 52.6%, respectively. Overall survival for patients having resection improved significantly for carcinoid tumors (89.2%) compared to functional and non-functional tumors (76.6%, and 78.7%, respectively). [54]
International statistics
In 1980-1989, the overall age-standardized incidence rate for male and female populations in England were estimated to be 0.71 (0.68-0.75 and 0.87 (0.83-0.91), respectively. In Scotland, the respective rates were 1.17 (0.91-1.44) per 100,000 population and 1.36 (1.09-1.63) per 100,000 population. [55]
A study by Duess et al in Germany reported that appendiceal carcinoid tumors were found incidentally in 0.11% of children who underwent appendectomy (44 out of 40,499 patients). [56]
Prognosis
No systematic data for survival of children with carcinoid tumors is currently available.
The prognosis for patients with completely resected localized disease is excellent. [57, 58, 59, 60] Tumors larger than 2 cm, positive lymph nodes, and atypical histologic features are often associated with a poor prognosis. [61] In patients with carcinoid tumors located in the appendix, age, primary tumor size, histologic features, lymph node involvement, and distant metastasis are significant factors in predicting survival. [62] In one retroactive study, survival of patients with sigmoid colon was only 33% while 99% of those with appendiceal tumor had survived. [58] Second primary malignancies of gastrointestinal tract which occurred in up to 33% of cases in adults,are unusual in children and adolescents. [59]
In adult patients, factors associated with poor survival include persistence of plasma neurokinin A (NKA), urinary 50-hydroxyindolacetic acid output, age, and 5 or more liver metastases. Rise in plasma NKA appears to be independent of other prognostic factors and constitutes the strongest indication. [63]
Overall, localized carcinoid tumor which is completely resected has an excellent prognosis; the outcome for patients with metastasis, however, remains poor.
Complications
The most serious complications of carcinoid tumors are carcinoid syndrome/crisis and metastasis, which is often observed in patients who have foregut tumors and high levels of 5-HIAA. [17]
-
Distribution of carcinoid tumors.
