Practice Essentials
Cerebrospinal fluid (CSF) leak may occur from the nose (rhinorrhea), from the external auditory canal (otorrhea), or from a traumatic or operative defect in the skull or spine. [1] CSF leaks occur when there is a tear or hole in the dura mater, which is the outermost layer of the meninges that protects the central nervous system. This leak of fluid can cause low-pressure headaches, neck pain, ringing in the ear, and, occasionally, loss of smell or taste. According to Ommaya et al, 80% of CSF leaks are due to nonsurgical trauma, 16% are iatrogenic, and 4% are spontaneous. The most common locations of a CSF leak are the upper thoracic level (T1-T6) and the lower thoracic level (T7-T12). [2, 3, 4, 5, 6]
The fluid leak is a result of meningeal dural and arachnoid laceration with fistula formation. Blunt trauma is the most common cause. Traumatic CSF leak is reported in approximately 10-30% of skull base fractures in adults. More than half of these present within 48 hours. The most common fracture sites leading to CSF leaks are the frontal sinus (30.8%), sphenoid sinus (11.4-30.8%), ethmoid (15.4-19.1%), cribriform plate (7.7%), frontoethmoid (7.7%), and sphenoethmoid (7.7%). [7]
(See the images below.)
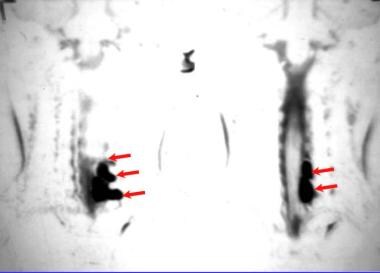
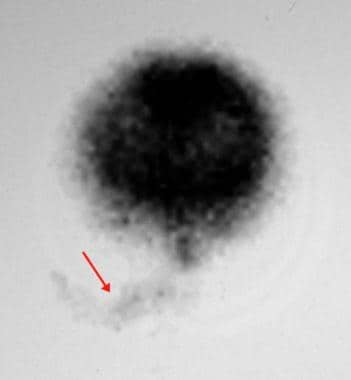
 Lateral 24-hour cranial scintigraphic image from a nuclear medicine cisternographic study in a patient with clinically evident right-sided cerebrospinal fluid rhinorrhea. Image demonstrates increased tracer accumulation in the nasal region (arrow).
Lateral 24-hour cranial scintigraphic image from a nuclear medicine cisternographic study in a patient with clinically evident right-sided cerebrospinal fluid rhinorrhea. Image demonstrates increased tracer accumulation in the nasal region (arrow).
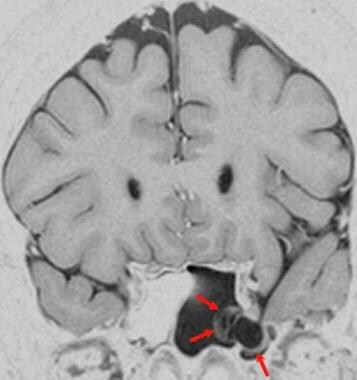
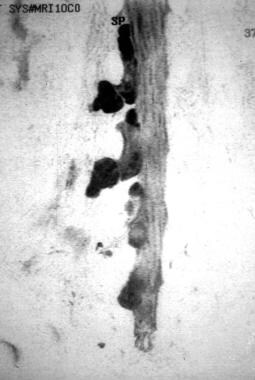
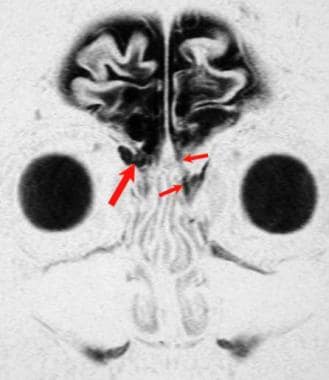 Acute posttraumatic cerebrospinal fluid rhinorrhea. This coronal magnetic resonance cisternogram demonstrates a left-sided cerebrospinal fluid leak through the cribriform plate (small arrows), which was clinically suspected. The image also shows a right-sided meningocele (large arrow) protruding through the cribriform plate, which was not suspected but was surgically repaired at the same time as the left cribriform cerebrospinal fluid leak site.
Acute posttraumatic cerebrospinal fluid rhinorrhea. This coronal magnetic resonance cisternogram demonstrates a left-sided cerebrospinal fluid leak through the cribriform plate (small arrows), which was clinically suspected. The image also shows a right-sided meningocele (large arrow) protruding through the cribriform plate, which was not suspected but was surgically repaired at the same time as the left cribriform cerebrospinal fluid leak site.
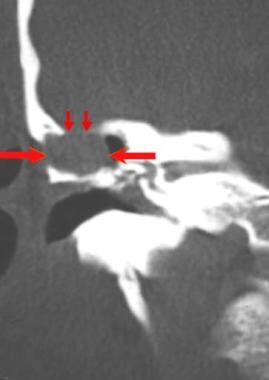 Coronal CT image of the temporal bone demonstrates a bone defect (small arrows) in the tegmen tympani with a protruding soft-tissue meningoencephalocele (large arrows). This patient had cerebrospinal fluid otorrhea after mastoidectomy.
Coronal CT image of the temporal bone demonstrates a bone defect (small arrows) in the tegmen tympani with a protruding soft-tissue meningoencephalocele (large arrows). This patient had cerebrospinal fluid otorrhea after mastoidectomy.
 Coronal fast spin-echo T2-weighted image demonstrates herniation of meninges and brain tissue (arrows) with adjacent cerebrospinal fluid into the postmastoidectomy tegmen tympani defect. This finding is consistent with a meningoencephalocele of the temporal bone.
Coronal fast spin-echo T2-weighted image demonstrates herniation of meninges and brain tissue (arrows) with adjacent cerebrospinal fluid into the postmastoidectomy tegmen tympani defect. This finding is consistent with a meningoencephalocele of the temporal bone.
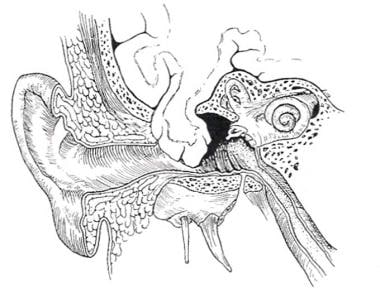 Artist's rendering of a tegmen tympani bone defect with a herniated meningoencephalocele.
Artist's rendering of a tegmen tympani bone defect with a herniated meningoencephalocele.
Leakage of CSF into the epidural space through a defect in the thecal sac has been found to be the underlying cause of almost all cases of spontaneous intracranial hypotension (SIH). Typically, the leak is caused by either spontaneous dural dehiscence or dural tears caused by degenerative causes. Generally, the goal of imaging is confirmation of the diagnosis of SIH through the visualization of a leak, as well as localization of the leak, to facilitate targeted treatment with either epidural patching or surgery. [8]
Imaging modalities
First-line imaging techniques of the spine include CT myelography (CTM) and MRI, which may be followed by dynamic myelography, digital subtraction myelography, [9, 10] and dynamic CTM to identify the site of a high-flow leak. [2, 11, 12, 13, 14]
A suggested algorithm for the diagnosis of a CSF fistula follows:
-
Fluid leaking from the nose or external auditory canal must first be positively identified as CSF. Drops of fluid from a CSF leak placed on absorbent filter paper may result in the double-ring sign: a central circle of blood and an outer clear ring of CSF. Serum glucose, chloride, and total protein tests of the fluid are not specific or conclusive for CSF.
-
Confirm or exclude the presence of CSF in leaking fluid by means of an immunoelectrophoretic study of the fluid for beta-2 transferrin (B2Tr) or, where available, beta-trace protein. [15] For this specialized laboratory study, 0.5-1.0 mL of the fluid may be required. An absorptive sponge pad placed at or near the presumed site of fluid leak can facilitate the collection of the fluid. The enzyme B2Tr is produced in the brain by neuraminidase activity and is present in CSF, perilymph, and ocular aqueous humor but not in sinonasal mucous secretions and tears. This feature is the basis for a specific test for CSF based on immunoelectrophoresis. B2Tr may be found in blood serum in liver disease, such as in chronic alcoholism and in patients with inborn errors of glycoprotein metabolism or genetic variants of transferrin [16]
-
Beta-trace protein is prostaglandin D2 synthase. It is produced in epithelial cells of the choroid plexus and meninges and is found in CSF, perilymph, seminal fluid, and urine. It is approximately 35 times more concentrated in CSF than in blood serum. Immunoelectrophoretic assay of beta-trace protein has been reported to have high specificity and sensitivity for CSF detection.
-
Perform magnetic resonance (MR) cisternography. This study may also be useful for detecting inactive fistulas, intermittent leaks, or suspected meningoencephaloceles. [15]
-
CT cisternography or radionuclide cisternography may be useful if CT and MR cisternography do not show the CSF fistula. Radionuclide cisternography may be useful to detect an intermittently active CSF fistula. Cisternography with an intrathecal injection of radioisotope or nonionic iodinated myelographic contrast medium or MRI cisternography usually localizes the CSF leak. [18]
-
On occasion, the methods listed above do not localize the CSF fistula, and surgical exploration may be necessary.
-
All methods of cisternography—radionuclide, CT, and MR—provide improved or optimal CSF fistula detection when the fistula is active and when a Valsalva maneuver or jugular venous compression is added to the imaging protocol. CSF fistula can usually be demonstrated by using some method of cisternography. Localization of the leak to the right or left nasal cavity may be difficult because of the tendency of the fluid to cross sides and flow from both nostrils. In a study of 4 patients who underwent radionuclide cisternography, as well as MRI and/or CT, for suspected CSF leaks, Thomas et al found that radionuclide cisternography accurately detected and localized the leaks in all patients. Each patient subsequently underwent a procedure for an epidural blood patch, and all patients experienced symptomatic relief. [22, 23, 16, 18, 24]
-
Methods for detecting CSF fistulas with intrathecal injections of dye pose a risk of chemical meningitis. Methylene blue, indigo carmine, and phenolsulfonphthalein (PSP) dyes are no longer in use. Some otolaryngologists use a dilute solution of fluorescein to localize CSF fistulas both preoperatively and during surgery. Typically, 0.5 mL of a 10% fluorescein solution is injected into the lumbar subarachnoid space over more than 1 minute. Cotton pledgets are placed in the nose, as for radionuclide cisternography. The dye reaches the skull base in 6 hours and is present over the cerebral convexities in 24 hours. The pledgets are examined for green fluorescence in a dark room with ultraviolet light 6 hours after the intrathecal PSP injection. [25]
-
Skull radiographs are of limited diagnostic use in CSF leaks, but they may show a relevant skull fracture or the presence of empty sella.
-
Diagnostic ultrasound has not been useful in cranial CSF leak. Paraspinal fluid collections can be localized for needle aspiration with ultrasound guidance.
-
Cerebral arteriography is not used in the diagnostic imaging workup to localize the site of a CSF leak. Arterial injury may occur with skull trauma that causes CSF leakage. CTA, MRA, or digital subtraction cerebral and cervical arteriography may then be necessary.
Computed Tomography
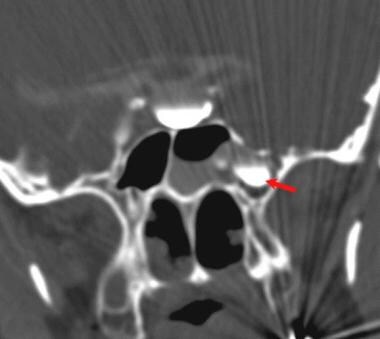
CT findings associated with cerebrospinal fluid leaks include fractures or other bone defects; meningocele; focal fluid accumulation in the ethmoid air cells; frontal, sphenoid, or maxillary sinuses or mastoid air cells; and, sometimes, pneumocephalus.
(See the images below.)
 This patient presented with a spontaneous onset of cerebrospinal fluid rhinorrhea 10 years after a head injury. This coronal CT cisternogram was obtained after an intrathecal injection of contrast material (Omnipaque 300, 8 mL) into the lumbar thecal sac and subsequent positioning of the contrast agent in the head. The image demonstrates dense contrast medium layering in the empty sella and contained within the meningocele (arrow).
This patient presented with a spontaneous onset of cerebrospinal fluid rhinorrhea 10 years after a head injury. This coronal CT cisternogram was obtained after an intrathecal injection of contrast material (Omnipaque 300, 8 mL) into the lumbar thecal sac and subsequent positioning of the contrast agent in the head. The image demonstrates dense contrast medium layering in the empty sella and contained within the meningocele (arrow).
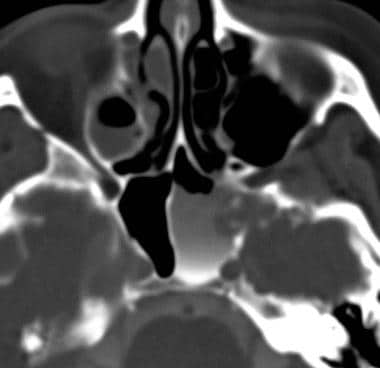 Axial CT image was obtained with the patient in the supine position. Contrast medium has drained out of the meningocele, but a small amount remains in the sphenoid sinus around the meningocele.
Axial CT image was obtained with the patient in the supine position. Contrast medium has drained out of the meningocele, but a small amount remains in the sphenoid sinus around the meningocele.
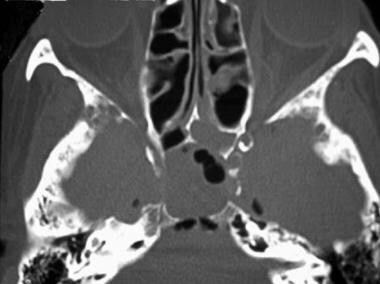 Axial CT image demonstrates pneumocephalus in association with the spontaneous cerebrospinal fluid rhinorrhea and a septal bone defect in the left posterior ethmoid air cell.
Coronal CT image of the temporal bone demonstrates a bone defect (small arrows) in the tegmen tympani with a protruding soft-tissue meningoencephalocele (large arrows). This patient had cerebrospinal fluid otorrhea after mastoidectomy.
Axial CT image demonstrates pneumocephalus in association with the spontaneous cerebrospinal fluid rhinorrhea and a septal bone defect in the left posterior ethmoid air cell.
Coronal CT image of the temporal bone demonstrates a bone defect (small arrows) in the tegmen tympani with a protruding soft-tissue meningoencephalocele (large arrows). This patient had cerebrospinal fluid otorrhea after mastoidectomy.
CT cranial cisternography is performed with injection of 5-7 mL of nonionic myelographic contrast medium into the lumbar subarachnoid space. The patient is maintained in the prone position until a CT scan is performed. Ideally, the contrast medium is concentrated in the intracranial anterior and posterior skull base regions under fluoroscopic guidance by tilting the prone patient head downward on a fluoroscopic tilt table. Alternatively, with the patient lying prone on a stretcher, the patient's hips can be raised above the level of the head for 1-2 minutes to concentrate the contrast medium over the anterior and posterior regions of the skull base. Coronal CT images of 2-3 mm thickness are then obtained through the face and cranium, including all of the paranasal sinuses and the mastoid air cells.
CT myelography is used in the detection of spinal CSF leak. Slow CSF leaks may be detected by postmyelogram CT scan in which there is a time delay between the contrast medium intrathecal injection in the fluoroscopic room and subsequent transfer to the CT scan room. Fast CSF leaks have rapid contrast diffusion and may not be localized to a 2-vertebral segment of the spinal canal (suitable for local treatment by extradural blood patch or alternate therapy) by routine postmyelogram CT spine scan. A high percentage of fast leaks have spinal extradural fluid collections on preliminary MRI spine scans. Dynamic CT myelography is recommended in these patients, with the injection of the iodinated contrast medium intrathecal on the CT scan table with immediate spine CT scan. [26, 27]
CT cisternographic findings in CSF leak include the concentration of contrast medium in portions of a paranasal sinus or within ethmoid or mastoid air cells. Occasionally, a stream of contrast medium is demonstrated at the fistula site.
Digital subtraction radiographic cisternography can be similarly performed with a spinal subarachnoid injection of nonionic iodinated contrast medium. The images may demonstrate a CSF fistula, but this technique is used less frequently than other cisternographic methods.
Degree of confidence
The incidence of CSF fistula detection varies from 22 to 100% in clinical studies. The fistula detection rate is lowest for intermittent CSF leaks. The accuracy of active fistula detection with CT cisternography is 65-85%. In one study of 45 patients, CT of the skull and facial bones with high-resolution, thin-section axial and coronal images had an accuracy of 92%, a sensitivity of 92%, and a specificity of 100% in depicting the presence or absence of CSF fistula. [28] Contemporary computer-reconstructed coronal images are usually of diagnostic quality, and direct CT coronal images may not be necessary.
Magnetic Resonance Imaging
Brain tissue herniation is best seen on MRI. Herniation of the inferior frontal gyrus may occur in frontal head injuries or in ethmoid developmental defects of the cribriform plate. Temporal lobe gyral herniation may occur through a petrous temporal bone tegmen tympani defect. [29, 30] (See images below.)
 Fast spin-echo T2-weighted coronal image of a patient with a spontaneous onset of cerebrospinal fluid rhinorrhea demonstrates an empty-sella configuration.
Fast spin-echo T2-weighted coronal image of a patient with a spontaneous onset of cerebrospinal fluid rhinorrhea demonstrates an empty-sella configuration.
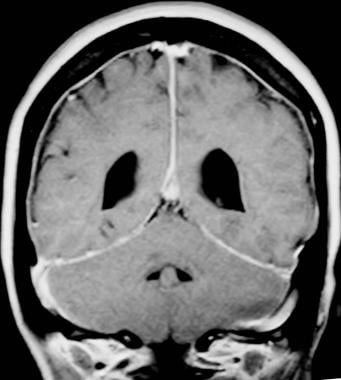
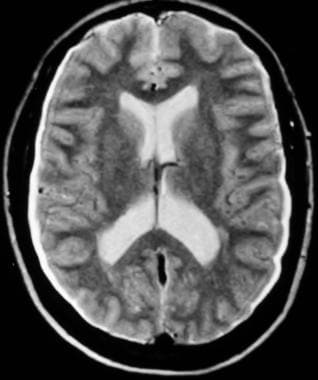 Spontaneous intracranial hypotension syndrome in a patient with chronic headaches, which began after lumbar puncture. Axial fast spin-echo T2-weighted MRI demonstrates widened extra-axial fluid spaces but no focal extra-axial fluid collection.
Spontaneous intracranial hypotension syndrome in a patient with chronic headaches, which began after lumbar puncture. Axial fast spin-echo T2-weighted MRI demonstrates widened extra-axial fluid spaces but no focal extra-axial fluid collection.
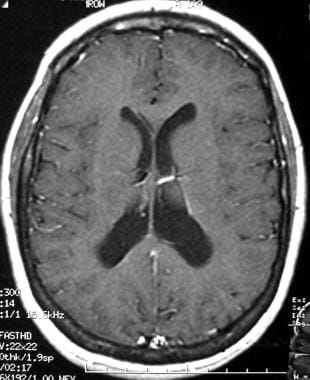
 Gadolinium-enhanced T1-weighted axial MRI shows diffuse moderate dural thickening with contrast enhancement.
Gadolinium-enhanced T1-weighted axial MRI shows diffuse moderate dural thickening with contrast enhancement.
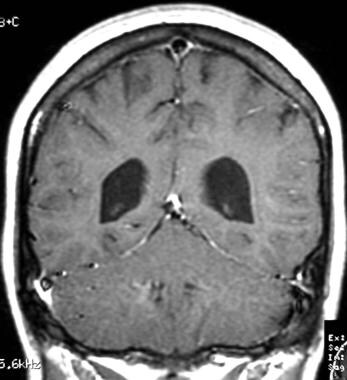
 Gadolinium-enhanced, coronal, T1-weighted MRI shows dural and tentorial thickening with contrast enhancement.
Gadolinium-enhanced, coronal, T1-weighted MRI shows dural and tentorial thickening with contrast enhancement.
 Gadolinium-enhanced, T1-weighted axial MRI obtained 2 weeks after a 7-mL extradural blood patch was applied to the midlumbar region. This image shows complete resolution of the previous dural thickening and contrast enhancement. The patient's severe postural headaches were markedly decreased in intensity.
Gadolinium-enhanced, T1-weighted axial MRI obtained 2 weeks after a 7-mL extradural blood patch was applied to the midlumbar region. This image shows complete resolution of the previous dural thickening and contrast enhancement. The patient's severe postural headaches were markedly decreased in intensity.
In spontaneous intracranial hypotension syndrome (SIHS), brain MRI shows thickening and contrast enhancement in the cranial pachymeninges. Subdural hygroma or hematoma on the cerebral convexities is common. The brain is noted to sink downward in the cranium with development of a pseudo-Chiari I malformation. The cerebral dural venous sinuses may be engorged. The cerebral ventricles may be reduced in size, and the pituitary gland may appear enlarged. There may be apparent downward displacement of the optic chiasm. The upper cervical epidural veins are congested. All of these changes are reversible with ablation of the cause of CSF leak, which is usually in the spine.
Spinal MRI in patients with SIHS may show some irregularity of the thecal sac due to partial dural collapse. Extradural fluid collections are common in spinal CSF leak. Intense extradural contrast enhancement is noted in congested epidural veins. One or more CSF fistulas may originate from spinal nerve root sleeves in the case of spontaneous spinal CSF leak.
The localization of one or multiple leaks can make possible and facilitate therapeutic CT-guided epidural blood patching. [31]
A variety of cisternographic studies may be necessary to localize some spinal CSF fistulas. Spinal MRI findings are also potentially reversible after successful ablation of a CSF fistula.
MR cisternography and myelography
MR cisternography and myelography can accurately localize CSF leaks in the cranium and spine. [32, 33, 34, 35] This technique is based on the intrinsic T2 contrast between CSF and adjacent structures. A positive diagnosis of CSF fistula is made by finding direct continuity of the CSF fistula with the subarachnoid space. Coronal and sagittal imaging is necessary.
(See images below.)
Acute posttraumatic cerebrospinal fluid rhinorrhea. This coronal magnetic resonance cisternogram demonstrates a left-sided cerebrospinal fluid leak through the cribriform plate (small arrows), which was clinically suspected. The image also shows a right-sided meningocele (large arrow) protruding through the cribriform plate, which was not suspected but was surgically repaired at the same time as the left cribriform cerebrospinal fluid leak site.
 Magnetic resonance cisternogram with cerebrospinal fluid rhinorrhea demonstrates a meningocele extending into the left lateral recess of the sphenoid sinus (arrows).
Magnetic resonance cisternogram with cerebrospinal fluid rhinorrhea demonstrates a meningocele extending into the left lateral recess of the sphenoid sinus (arrows).
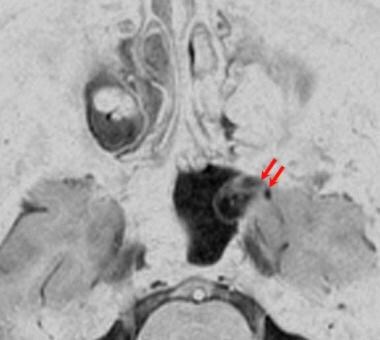 Axial magnetic resonance cisternogram demonstrates the connection of the meningocele to the middle cranial fossa (arrows). Fluid contained in the meningocele and leaked fluid in the sphenoid sinus outline the meningocele membrane.
Axial magnetic resonance cisternogram demonstrates the connection of the meningocele to the middle cranial fossa (arrows). Fluid contained in the meningocele and leaked fluid in the sphenoid sinus outline the meningocele membrane.
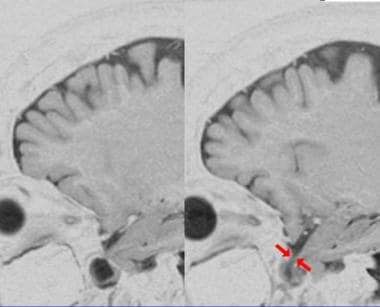 Sagittal magnetic resonance cisternogram demonstrates the connection of the meningocele to the middle cranial fossa; this finding facilitated surgical planning.
Sagittal magnetic resonance cisternogram demonstrates the connection of the meningocele to the middle cranial fossa; this finding facilitated surgical planning.
The high T2 signal from CSF fistula may be difficult to differentiate from that of sinusitis on axial images. A high rate of fistula detection may be possible with imaging in the prone position, but this may be uncomfortable for the patient. Therefore, imaging is usually done with the patient in the supine position. Rapid echo-planar imaging with the patient in the prone position and performing a Valsalva maneuver may allow for limited coronal imaging and increase the accuracy of MR cisternography.
MR cisternography is performed with heavily T2-weighted, fast spin-echo, fat-saturated sequences with thin sections and minimal or no gap. Typical imaging parameters include a repetition time of 10,000 ms, an effective echo time of 200 ms, 4 signals acquired, an echo train length of 16, a matrix of 512 X 192, no phase-wrap option, 3-mm sections interleaved contiguously (0-mm gap), and a 16-cm field of view.
A short repetition time can be used to achieve a result similar to that of the technique above, with slightly faster imaging times. The gray scale is reversed for optimal viewing. With one method, the average total time for coronal and sagittal imaging is 48 minutes. [36] Most MRI machines offer fat suppression and image gray-scale reversal. Additional hardware or software is not required to perform MR myelography or cisternography.
MR cisternography may demonstrate inactive CSF fistulas. MR T2 myelography may demonstrate spinal CSF fistulas (see the images below). The intrathecal injection of 0.5 mL of gadopentetate dimeglumine diluted in 3-5 mL of CSF for MR cisternography has been reported to have high sensitivity and specificity for detection of active CSF fistula, exceeding the rate of fistula demonstration by CT, nuclear medicine, or noncontrasted MR cisternography.
Small series of patients had no apparent adverse effect from the gadolinium contrast medium. [34, 37] Gadolinium-based contrast media are approved for intravenous injection for MRI but have not been approved for intrathecal use in humans by the Food and Drug Administration (FDA). The intrathecal injection of gadolinium-based contrast media has been shown in several off-label studies to be effective and safe in selected patients in whom other cisternographic or myelographic studies have failed to demonstrate the CSF leak site. [38, 39] Severe brain injury has been reported in a patient who received, erroneously, 30 times the intended dose of gadolinium in an MRI myelogram. [40]
In a small series of patients with spontaneous intracranial hypotension (SIH), instillation of preservative-free normal saline into the thecal sac followed by intrathecal gadolinium infusion was found to be a safe technique that increased the detection of a CSF leak on MR myelography images. [41]
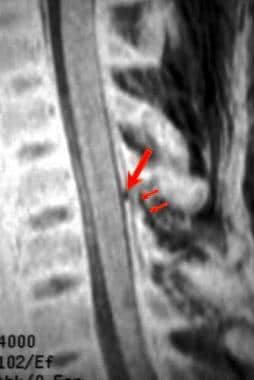 Sagittal magnetic resonance myelogram demonstrates a traumatic cerebrospinal fluid leak (small arrows) with disruption of the ligamentum flavum posteriorly (large arrow).
Sagittal magnetic resonance myelogram demonstrates a traumatic cerebrospinal fluid leak (small arrows) with disruption of the ligamentum flavum posteriorly (large arrow).
 Magnetic resonance myelogram in a patient with a brachial plexus injury and pseudomeningoceles (arrows).
Magnetic resonance myelogram in a patient with a brachial plexus injury and pseudomeningoceles (arrows).
 Magnetic resonance myelogram demonstrates pseudomeningoceles secondary to a stretch injury of the lumbosacral nerve roots.
Magnetic resonance myelogram demonstrates pseudomeningoceles secondary to a stretch injury of the lumbosacral nerve roots.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). NSF/NFD has occurred in patients with moderate to end-stage renal disease who have been given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the sclera of the eyes; joint stiffness with difficulty moving or straightening the arms, hands, legs, or feet; pain deep in the hips or ribs; and muscle weakness.
Nuclear Imaging
Radionuclide cisternography is performed by administering a lumbar subarachnoid intrathecal injection of Indium-111 (111In) diethylenetriamine pentaacetic acid (DTPA) in a 500 µCi dose. In-111 has minimal background activity and does not accumulate in the brain. Technetium as 99mTc DTPA is a less frequently used isotope. [42] The sensitivity for CSF leaks is in the range of 50-100%. The specificity is almost 100% for contemporary radionuclide cisternography.
(See images below.)
Lateral 24-hour cranial scintigraphic image from a nuclear medicine cisternographic study in a patient with clinically evident right-sided cerebrospinal fluid rhinorrhea. Image demonstrates increased tracer accumulation in the nasal region (arrow).
 Anterior 48-hour scintigraphic image demonstrates tracer accumulation in the right nasal region. Imaging findings were correlated with both the clinical findings and nasal pledget counts obtained as part of this study.
Anterior 48-hour scintigraphic image demonstrates tracer accumulation in the right nasal region. Imaging findings were correlated with both the clinical findings and nasal pledget counts obtained as part of this study.
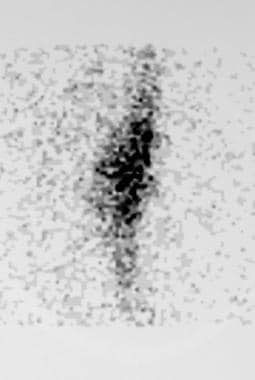 Nuclear cisternogram obtained at 24 hours demonstrates diffuse epidural accumulation of the tracer in the midlumbar region. This finding is suggestive of a site of cerebrospinal fluid leak.
Nuclear cisternogram obtained at 24 hours demonstrates diffuse epidural accumulation of the tracer in the midlumbar region. This finding is suggestive of a site of cerebrospinal fluid leak.
Head images are acquired 2, 6, 12, and 24 hours after injection of the isotope. Follow-up 48- or 72-hour scans are possible with 111In and may be useful in the detection of intermittent CSF fluid leaks.
The entire spine is scanned up to 24 hours in cases of spontaneous intracranial hypotension, spinal trauma, or postoperative CSF leaks. [43] Cotton pledgets labeled for the placement site are positioned in the nose before the lumbar subarachnoid space injection of the isotope. Pledgets are placed close to the cribriform plate, in the middle meatus, and in the sphenoethmoidal recess of the right and left nasal cavities. A control pledget for lacrimal secretions is placed under one inferior nasal turbinate.
Pledgets are scanned in a glass tube at intervals of 2-24 hours, with the highest count rate indicating a possible leak site. Alternatively, radioactivity of the nasal pledgets is compared to that of known plasma radioactivity.
For otorrhea, 1 cotton pledget is placed in each external auditory canal.
-
Lateral 24-hour cranial scintigraphic image from a nuclear medicine cisternographic study in a patient with clinically evident right-sided cerebrospinal fluid rhinorrhea. Image demonstrates increased tracer accumulation in the nasal region (arrow).
-
Anterior 48-hour scintigraphic image demonstrates tracer accumulation in the right nasal region. Imaging findings were correlated with both the clinical findings and nasal pledget counts obtained as part of this study.
-
Acute posttraumatic cerebrospinal fluid rhinorrhea. This coronal magnetic resonance cisternogram demonstrates a left-sided cerebrospinal fluid leak through the cribriform plate (small arrows), which was clinically suspected. The image also shows a right-sided meningocele (large arrow) protruding through the cribriform plate, which was not suspected but was surgically repaired at the same time as the left cribriform cerebrospinal fluid leak site.
-
This patient presented with a spontaneous onset of cerebrospinal fluid rhinorrhea 10 years after a head injury. This coronal CT cisternogram was obtained after an intrathecal injection of contrast material (Omnipaque 300, 8 mL) into the lumbar thecal sac and subsequent positioning of the contrast agent in the head. The image demonstrates dense contrast medium layering in the empty sella and contained within the meningocele (arrow).
-
Axial CT image was obtained with the patient in the supine position. Contrast medium has drained out of the meningocele, but a small amount remains in the sphenoid sinus around the meningocele.
-
Magnetic resonance cisternogram with cerebrospinal fluid rhinorrhea demonstrates a meningocele extending into the left lateral recess of the sphenoid sinus (arrows).
-
Axial magnetic resonance cisternogram demonstrates the connection of the meningocele to the middle cranial fossa (arrows). Fluid contained in the meningocele and leaked fluid in the sphenoid sinus outline the meningocele membrane.
-
Sagittal magnetic resonance cisternogram demonstrates the connection of the meningocele to the middle cranial fossa; this finding facilitated surgical planning.
-
Fast spin-echo T2-weighted coronal image of a patient with a spontaneous onset of cerebrospinal fluid rhinorrhea demonstrates an empty-sella configuration.
-
Axial CT image demonstrates pneumocephalus in association with the spontaneous cerebrospinal fluid rhinorrhea and a septal bone defect in the left posterior ethmoid air cell.
-
Coronal CT image of the temporal bone demonstrates a bone defect (small arrows) in the tegmen tympani with a protruding soft-tissue meningoencephalocele (large arrows). This patient had cerebrospinal fluid otorrhea after mastoidectomy.
-
Coronal fast spin-echo T2-weighted image demonstrates herniation of meninges and brain tissue (arrows) with adjacent cerebrospinal fluid into the postmastoidectomy tegmen tympani defect. This finding is consistent with a meningoencephalocele of the temporal bone.
-
Artist's rendering of a tegmen tympani bone defect with a herniated meningoencephalocele.
-
Sagittal magnetic resonance myelogram demonstrates a traumatic cerebrospinal fluid leak (small arrows) with disruption of the ligamentum flavum posteriorly (large arrow).
-
Magnetic resonance myelogram in a patient with a brachial plexus injury and pseudomeningoceles (arrows).
-
Magnetic resonance myelogram demonstrates pseudomeningoceles secondary to a stretch injury of the lumbosacral nerve roots.
-
Spontaneous intracranial hypotension syndrome in a patient with chronic headaches, which began after lumbar puncture. Axial fast spin-echo T2-weighted MRI demonstrates widened extra-axial fluid spaces but no focal extra-axial fluid collection.
-
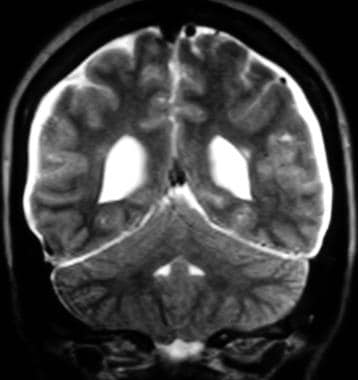
Coronal fast spin-echo T2-weighted MRI.
-
Gadolinium-enhanced T1-weighted axial MRI shows diffuse moderate dural thickening with contrast enhancement.
-
Gadolinium-enhanced, coronal, T1-weighted MRI shows dural and tentorial thickening with contrast enhancement.
-
Nuclear cisternogram obtained at 24 hours demonstrates diffuse epidural accumulation of the tracer in the midlumbar region. This finding is suggestive of a site of cerebrospinal fluid leak.
-
Gadolinium-enhanced, T1-weighted axial MRI obtained 2 weeks after a 7-mL extradural blood patch was applied to the midlumbar region. This image shows complete resolution of the previous dural thickening and contrast enhancement. The patient's severe postural headaches were markedly decreased in intensity.
-
Gadolinium-enhanced, coronal, T1-weighted MRI.
Tables

What would you like to print?
- Fauci Denies Suppressing COVID Lab Leak Theory Before US House Panel
- Fluid Restriction May Prevent MDMA-Related Hyponatremia
- SARS-CoV-2 Origin: Lab Leak Hypothesis Gains Momentum
- Otolaryngology Considerations of Pituitary Surgery
- Updates in the Early Management of Acute Spinal Cord Injury
-
 What's the Most Likely Cause of This Man's Severe Headaches?
What's the Most Likely Cause of This Man's Severe Headaches?
