Practice Essentials
Dandy-Walker malformation (DWM) is a rare congenital malformation that involves the cerebellum and fourth ventricle. Dandy-Walker malformation and related variants have a prevalence of 1 in 35,000 live births in the United States. [1, 2, 3, 4] Dandy-Walker malformation is characterized by agenesis or hypoplasia of the cerebellar vermis, cystic dilatation of the fourth ventricle, and enlargement of the posterior fossa. A large number of concomitant problems may be present, but Dandy-Walker malformation is recognized whenever these 3 features are found. Approximately 70-90% of patients have hydrocephalus, which often develops postnatally. Dandy-Walker malformation may be associated with atresia of the foramen of Magendie and, possibly, the foramen of Luschka. [5, 6, 7, 8, 9]
(See the images of Dandy-Walker malformation below.)
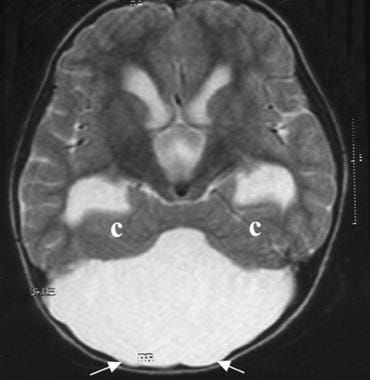 Dandy-Walker malformation. An axial T2-weighted MRI scan that shows hydrocephalus, a large cerebrospinal fluid cyst in the posterior fossa, thinned occipital bone (arrows), and hypoplastic cerebellar hemispheres with a winged appearance (c).
Dandy-Walker malformation. An axial T2-weighted MRI scan that shows hydrocephalus, a large cerebrospinal fluid cyst in the posterior fossa, thinned occipital bone (arrows), and hypoplastic cerebellar hemispheres with a winged appearance (c).
 Dandy-Walker malformation. An axial T1-weighted MRI scan showing ventriculomegaly and a superiorly displaced posterior fossa cyst.
Dandy-Walker malformation. An axial T1-weighted MRI scan showing ventriculomegaly and a superiorly displaced posterior fossa cyst.
Dandy-Walker complex
Classically, posterior fossa cystic malformations have been divided into Dandy-Walker malformation, Dandy-Walker variant, mega cisterna magna, and posterior fossa arachnoid cyst. Precisely differentiating the malformations may not be possible using imaging studies. Dandy-Walker malformation, variant, and mega cisterna magna are currently believed to represent a continuum of developmental anomalies on a spectrum that has been termed the Dandy-Walker complex. [10, 11, 12, 8]
Dandy-Walker complex is characterized by an enlarged posterior fossa; a high position of the tentorium, with upward displacement of the lateral sinuses; torcular herophili associated with varying degrees of vermian aplasia or hypoplasia; and a cystic dilatation of the fourth ventricle that nearly fills the entire posterior fossa.
Radiography
Plain radiographs have diagnostic importance in imaging bony abnormalities and in the evaluation of ventriculoperitoneal shunt malfunction. On conventional radiographs, the posterior fossa is disproportionately enlarged, with characteristic thinning and bulging of the occiput. Increased pressure from the massively dilated fourth ventricle, along with prominent CSF pulsations through the cyst fluid, causes widening of the diastatic lambdoid sutures and erosive scalloping of the occiput. Torcular herophili and lateral sinus grooves are located high above the lambdoid angle (torcular-lambdoid angle inversion). [11]
Computed Tomography
CT is used to diagnose Dandy-Walker malformation and to follow ventricular shunt function in shunted patients. Nonenhanced CT examination successfully delineates multiple components of Dandy-Walker malformation, which includes partial or complete absence of the cerebellar vermis; posterior fossa cyst contiguous with the fourth ventricle; small and widely separated cerebellar hemispheres; anterior and lateral displacement of hypoplastic cerebellar hemispheres; anterior displacement of pons; elevated imprint of the transverse sinuses, with thinning and bulging of the bones of the posterior fossa; scalloping of petrous pyramids; and hydrocephalus.
Three-dimensional (3D) CT and CT angiography studies can be used to evaluate osseous malformation and the relationships between vascular and bony structures. For these studies, 1-mm thickness, an axial plane, and 3D reconstruction are used.
CT scans can depict the malformation relatively well, but a slice may miss the relevant presence of the vermis. Clearly distinguishing Dandy-Walker complex subtypes using axial CT images is difficult. [34]
(See the CT images of Dandy-Walker malformation below.)
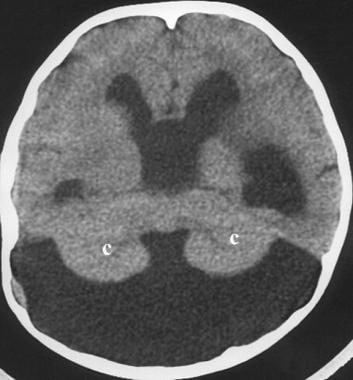 Dandy-Walker malformation. An axial computed tomography (CT) scan in a 7-year-old girl with hydrocephalus showing a large cerebrospinal fluid cyst in the posterior fossa and hypoplastic cerebellar hemispheres with a winged appearance (c).
Dandy-Walker malformation. An axial computed tomography (CT) scan in a 7-year-old girl with hydrocephalus showing a large cerebrospinal fluid cyst in the posterior fossa and hypoplastic cerebellar hemispheres with a winged appearance (c).
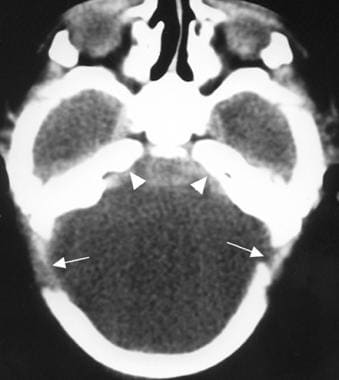 Dandy-Walker malformation. An axial CT scan in a 1-day-old boy that shows a large posterior fossa cyst, separation of the lambdoid sutures (large arrows), and concavity of the petrous ridges (small arrows).
Dandy-Walker malformation. An axial CT scan in a 1-day-old boy that shows a large posterior fossa cyst, separation of the lambdoid sutures (large arrows), and concavity of the petrous ridges (small arrows).
 Dandy-Walker malformation. Joubert syndrome in an 8-month-old boy. The axial CT scan obtained near the pontomesencephalic junction shows a batwing configuration of the fourth ventricle and unusual definition of the superior cerebellar peduncles at this level (arrows). The vermis is dysgenetic, and the 2 cerebellar hemispheres appose each other in the midline.
Dandy-Walker malformation. Joubert syndrome in an 8-month-old boy. The axial CT scan obtained near the pontomesencephalic junction shows a batwing configuration of the fourth ventricle and unusual definition of the superior cerebellar peduncles at this level (arrows). The vermis is dysgenetic, and the 2 cerebellar hemispheres appose each other in the midline.
 Dandy-Walker malformation. An axial CT scan showing the sinus confluence (large arrow) and sinus transversus (small arrows) displaced superiorly in Dandy-Walker malformation (lambdoid-torcular inversion).
Dandy-Walker malformation. An axial CT scan showing the sinus confluence (large arrow) and sinus transversus (small arrows) displaced superiorly in Dandy-Walker malformation (lambdoid-torcular inversion).
Magnetic Resonance Imaging
Malformations of the CNS are best delineated using MRI. The diagnosis is straightforward when typical MRI findings are present. MRI is usually required for better anatomic resolution prior to surgical intervention. [25, 35, 36]
(See the MRI images of Dandy-Walker malformation below.)
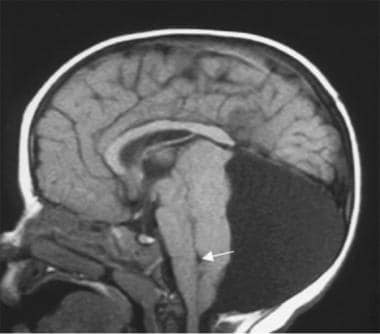
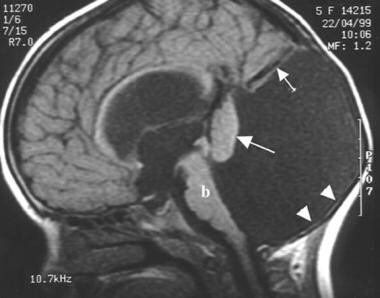 Dandy-Walker malformation. A sagittal T1-weighted magnetic resonance imaging (MRI) scan in a 5-year-old girl (also see the following 2 images) shows a large posterior fossa cyst elevating the torcular herophili and sinus rectus (short arrow). The hypoplastic vermis is everted over the posterior fossa cyst (long arrow). The cerebellar hemispheres and brainstem (b) are hypoplastic. Thinned occipital squama is seen (arrowheads).
Dandy-Walker malformation. An axial T2-weighted MRI scan that shows hydrocephalus, a large cerebrospinal fluid cyst in the posterior fossa, thinned occipital bone (arrows), and hypoplastic cerebellar hemispheres with a winged appearance (c).
Dandy-Walker malformation. An axial T1-weighted MRI scan showing ventriculomegaly and a superiorly displaced posterior fossa cyst.
Dandy-Walker malformation. A sagittal T1-weighted magnetic resonance imaging (MRI) scan in a 5-year-old girl (also see the following 2 images) shows a large posterior fossa cyst elevating the torcular herophili and sinus rectus (short arrow). The hypoplastic vermis is everted over the posterior fossa cyst (long arrow). The cerebellar hemispheres and brainstem (b) are hypoplastic. Thinned occipital squama is seen (arrowheads).
Dandy-Walker malformation. An axial T2-weighted MRI scan that shows hydrocephalus, a large cerebrospinal fluid cyst in the posterior fossa, thinned occipital bone (arrows), and hypoplastic cerebellar hemispheres with a winged appearance (c).
Dandy-Walker malformation. An axial T1-weighted MRI scan showing ventriculomegaly and a superiorly displaced posterior fossa cyst.
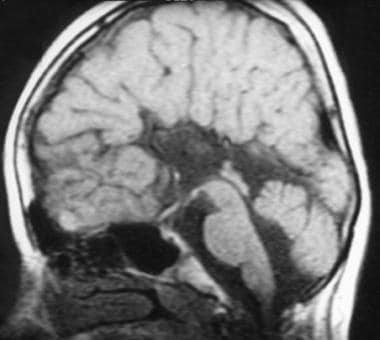
 Dandy-Walker malformation. This sagittal T1-weighted MRI scan in an 11-day-old boy (also see the following image) shows agenesis of the corpus callosum, a hypoplastic brainstem (b), elevation of the torcular herophili (lambdoid-torcular inversion, large arrow), a large fourth ventricle, and a markedly hypoplastic vermis that is rotated superiorly (small arrow).
Dandy-Walker malformation. This sagittal T1-weighted MRI scan in an 11-day-old boy (also see the following image) shows agenesis of the corpus callosum, a hypoplastic brainstem (b), elevation of the torcular herophili (lambdoid-torcular inversion, large arrow), a large fourth ventricle, and a markedly hypoplastic vermis that is rotated superiorly (small arrow).
 Dandy-Walker malformation. An axial T1-weighted MRI showing an elevated, anteriorly displaced torcular herophili (arrow) and a superiorly displaced posterior fossa cyst.
Dandy-Walker malformation. An axial T1-weighted MRI showing an elevated, anteriorly displaced torcular herophili (arrow) and a superiorly displaced posterior fossa cyst.
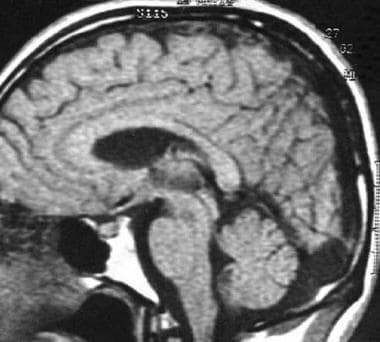
 Dandy-Walker malformation. This sagittal T1-weighted MRI shows agenesis of the corpus callosum and a hypoplastic inferior vermis in a 13-year-old girl with thoracal scoliosis and Dandy-Walker variant. The fourth ventricle is slightly enlarged, but the posterior fossa typically is normal in size.
Dandy-Walker malformation. This sagittal T1-weighted MRI shows agenesis of the corpus callosum and a hypoplastic inferior vermis in a 13-year-old girl with thoracal scoliosis and Dandy-Walker variant. The fourth ventricle is slightly enlarged, but the posterior fossa typically is normal in size.
 Dandy-Walker malformation. This sagittal T1-weighted MRI shows a large retrocerebellar cerebrospinal fluid collection and a normal fourth ventricle and vermis in a patient with mega cisterna magna in Dandy-Walker malformation.
Dandy-Walker malformation. This sagittal T1-weighted MRI shows a large retrocerebellar cerebrospinal fluid collection and a normal fourth ventricle and vermis in a patient with mega cisterna magna in Dandy-Walker malformation.
 Dandy-Walker malformation. A posterior fossa arachnoid cyst in a 15-month-old girl with a lumbar pilonidal sinus. The sagittal T1-weighted MRI shows a large posterior fossa cyst that is compressing the cerebellar hemispheres, vermis, fourth ventricle (arrow), and brainstem.
Dandy-Walker malformation. A posterior fossa arachnoid cyst in a 15-month-old girl with a lumbar pilonidal sinus. The sagittal T1-weighted MRI shows a large posterior fossa cyst that is compressing the cerebellar hemispheres, vermis, fourth ventricle (arrow), and brainstem.
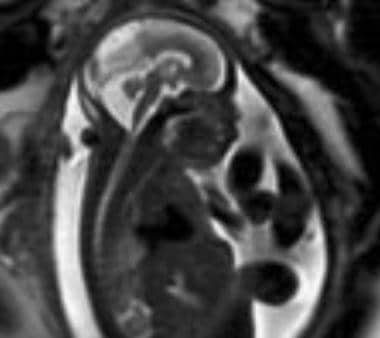 Dandy-Walker malformation. An antenatal MRI showing Dandy-Walker malformation in a fetus. Courtesy of Umit Aksoy, MD, Uludag University, Bursa, Turkey.
Dandy-Walker malformation. An antenatal MRI showing Dandy-Walker malformation in a fetus. Courtesy of Umit Aksoy, MD, Uludag University, Bursa, Turkey.
Nonenhanced routine cranial MRI can image the altered anatomy and provide excellent images in all projections (sagittal, axial, coronal), of which the sagittal view is one of the most useful.
Hypoplasia or absence of the cerebellar vermis is best detected using thin-sectioned midline sagittal T1-weighted images. Wide separation of the cerebellar hemispheres without intervening vermis can be seen in axial or coronal images. In some patients, the inferior lobules of the vermis appear to be hypoplastic, while in others, they appear to be intact. Remnants of the dysplastic upper vermis are rotated anterosuperiorly, compressed, and attached to the tentorium. Axial images alone may be misleading in revealing the upwardly rotated vermis.
An enlarged posterior fossa, cyst formation in the posterior fossa, anterolaterally winged cerebellar hemispheres (winged outward), absence of falx cerebelli, and scalloping of petrous pyramids are well-demonstrated on T1-weighted images.
Sagittal MRI can help evaluate an abnormally high position of the straight sinus, torcular herophili, tentorium, high tentorial insertion (lambdoid-torcular inversion), hypoplastic and compressed brainstem, and obstructive hydrocephalus secondary to cystic dilatation of the fourth ventricle in patients with Dandy-Walker malformation. [18]
CSF flow and cine MRI techniques are valuable imaging methods for demonstrating patency of the CSF pathways at the level of the incisura or aqueduct of Sylvius. Shunting of the cyst alone in the presence of aqueductal obstruction may result in downward transincisural herniation of the cerebrum and atria of the lateral ventricles; however, shunting of the lateral ventricles alone when the aqueduct is obstructed may lead to an upward herniation of the posterior fossa cyst, resulting in a characteristic "snowman" appearance in the sagittal plane in the absence of communication. The hydrocephalus in patients with Dandy-Walker malformation is frequently communicating in type with patency of the aqueduct. [37]
Assessing the presence of associated supratentorial anomalies is important, since the prognosis for patients is much better in the absence of the anomalies. MRI affords an accurate, objective, and detailed identification of supratentorial anomalies.
MRI and US have been used as diagnostic tools in the antenatal period. Fetal MRI at younger gestational age (such as < 20 wk) may have a reduced specificity. This may be related to small size, fetal motion, volume averaging, and difficulty in obtaining a true mid-sagittal image. Follow-up MR imaging, either at a later gestational age or postnatally, is recommended. [30]
Use of a novel 3D MRI technique to image the fetal posterior fossa has been reported. In a comparison of standard 2D MRI images to 3D reconstructed MRI images, lengths of the transcerebellar diameter measured within a 3D reconstruction were more concordant between imaging planes, as they correct for fetal motion and orthogonal slice acquisition. [38]
A systematic review of 217 fetuses diagnosed with Dandy-Walker malformation found that the prenatal diagnosis was not confirmed after birth in 28.2% (95% CI, 8.5-53.9%) of cases. [39]
In a study by Akiyama et al, volumetric analysis of fetal MRI showed that regardless of heterogeneous etiologies, fetuses with Dandy-Walker malformation had a larger cortical plate volume than control fetuses. In addition, after excluding fetuses with agenesis of the corpus callosum (ACC), fetuses with Dandy-Walker malformation were shown to have larger subcortical parenchyma, whole cerebrum, and cerebellar hemispheres than control fetuses. [40]
Ultrasonography
Classic abnormal findings described on cranial CT and MRI scans can also be demonstrated on cranial sonography. Commercially available equipment is used, with transducers of 3-7.5 MHz (depending on the size of the patient's head). Transducers of 5-7.5 MHz are used for newborns, and transducers of 3-5 MHz are used for older infants.
(See the US images of Dandy-Walker malformation below.)
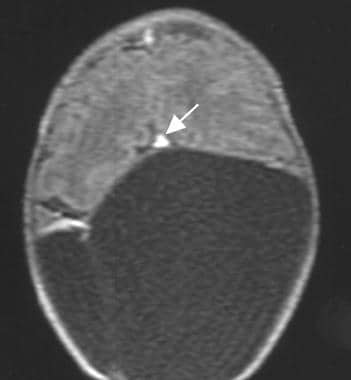
 Dandy-Walker malformation. An in utero sonogram of Dandy-Walker malformation; note the abnormal cerebellar vermis in association with a posterior fossa cyst (arrow) and splaying of the cerebellar hemispheres. Image courtesy of Ecker et al.
Dandy-Walker malformation. An in utero sonogram of Dandy-Walker malformation; note the abnormal cerebellar vermis in association with a posterior fossa cyst (arrow) and splaying of the cerebellar hemispheres. Image courtesy of Ecker et al.
 Dandy-Walker malformation. An antenatal sonogram that shows Dandy-Walker malformation (arrow) in a fetus. Courtesy of Umit Aksoy, MD, Uludag University, Bursa, Turkey.
Dandy-Walker malformation. An antenatal sonogram that shows Dandy-Walker malformation (arrow) in a fetus. Courtesy of Umit Aksoy, MD, Uludag University, Bursa, Turkey.
On US, a large posterior fossa midline cyst that communicates with the fourth ventricle is best demonstrated on midline sagittal sections. The anterolaterally displaced hypoplastic cerebellar hemispheres are best seen in the coronal projection. Sagittal and coronal sections can demonstrate enlargement of the posterior fossa, high position of the tentorium, and dilated third and lateral ventricles.
Scans performed with the transducer can show a large posterior fossa cyst and hypoplastic cerebellar hemispheres. This is accomplished by using the transfontanel approach, as well as by placing the transducer directly over the posterior or posterolateral fontanelle.
In these patients, it is important to assess the supratentorial compartment for associated anomalies, such as callosal agenesis.
Using US, Dandy-Walker malformation is usually discovered before birth, although prominence of the cisterna magna is often confused with Dandy-Walker malformation in utero.
Prenatal diagnosis of Dandy-Walker malformation should not be made before the 18th week of gestation, because development of the cerebellar vermis may be incomplete at that time. Although great variability exists in intracranial findings in fetuses, sagittal measurements exceeding 10 mm help confirm the presence of a Dandy-Walker cyst.
However, a study of the feasiblity of US visualization and measurement of the fetal posterior fossa anatomy at 11-14 weeks' gestation found that a large brainstem‐to‐occipital bone (BSOB) diameter and a decreased brainstem:BSOB ratio, particularly in combination with the presence of only 2 brain spaces, is an important risk factor for cystic posterior fossa malformations, most frequently Dandy-Walker malformation. [41]
US examination, including fetal echocardiography, should be directed toward identifying additional supratentorial and extracranial anomalies. Follow-up sonograms are useful for monitoring cyst size and ventriculomegaly. Three-dimensional US reportedly proved most helpful in delineating the exact nature and anatomic level of the anomaly in utero. [24, 21, 42, 43, 44]
US is heavily operator-dependent. Associated findings of Dandy-Walker malformation, such as pachygyria, polymicrogyria, heterotopias, and dural abnormalities, may be missed. Fetal US can demonstrate Dandy-Walker malformation and variant, but caution should be exercised because the normal developing cerebellum can mimic hypoplasia.
Angiography
Radiographic angiography can demonstrate angiographic features of Dandy-Walker malformation. In the arterial phase, the posterior cerebral vessels are elevated. The superior cerebellar arteries are displaced anterosuperiorly above the posterior cerebral arteries. The posterior inferior cerebellar arteries (PICAs) are shortened, with high tonsillar loop. The inferior vermian branches of the PICA are absent. In some patients, the entire PICA is absent or hypoplastic. In the venous phase, arteriography shows absence of the inferior vermian veins, elevation of the great vein of Galen, and high position of the transverse sinuses. [45]
-
Dandy-Walker malformation. A sagittal T1-weighted magnetic resonance imaging (MRI) scan in a 5-year-old girl (also see the following 2 images) shows a large posterior fossa cyst elevating the torcular herophili and sinus rectus (short arrow). The hypoplastic vermis is everted over the posterior fossa cyst (long arrow). The cerebellar hemispheres and brainstem (b) are hypoplastic. Thinned occipital squama is seen (arrowheads).
-
Dandy-Walker malformation. An axial T2-weighted MRI scan that shows hydrocephalus, a large cerebrospinal fluid cyst in the posterior fossa, thinned occipital bone (arrows), and hypoplastic cerebellar hemispheres with a winged appearance (c).
-
Dandy-Walker malformation. An axial T1-weighted MRI scan showing ventriculomegaly and a superiorly displaced posterior fossa cyst.
-
Dandy-Walker malformation. This sagittal T1-weighted MRI scan in an 11-day-old boy (also see the following image) shows agenesis of the corpus callosum, a hypoplastic brainstem (b), elevation of the torcular herophili (lambdoid-torcular inversion, large arrow), a large fourth ventricle, and a markedly hypoplastic vermis that is rotated superiorly (small arrow).
-
Dandy-Walker malformation. An axial T1-weighted MRI showing an elevated, anteriorly displaced torcular herophili (arrow) and a superiorly displaced posterior fossa cyst.
-
Dandy-Walker malformation. An axial computed tomography (CT) scan in a 7-year-old girl with hydrocephalus showing a large cerebrospinal fluid cyst in the posterior fossa and hypoplastic cerebellar hemispheres with a winged appearance (c).
-
Dandy-Walker malformation. An axial CT scan in a 1-day-old boy that shows a large posterior fossa cyst, separation of the lambdoid sutures (large arrows), and concavity of the petrous ridges (small arrows).
-
Dandy-Walker malformation. This sagittal T1-weighted MRI shows agenesis of the corpus callosum and a hypoplastic inferior vermis in a 13-year-old girl with thoracal scoliosis and Dandy-Walker variant. The fourth ventricle is slightly enlarged, but the posterior fossa typically is normal in size.
-
Dandy-Walker malformation. This sagittal T1-weighted MRI shows a large retrocerebellar cerebrospinal fluid collection and a normal fourth ventricle and vermis in a patient with mega cisterna magna in Dandy-Walker malformation.
-
Dandy-Walker malformation. A posterior fossa arachnoid cyst in a 15-month-old girl with a lumbar pilonidal sinus. The sagittal T1-weighted MRI shows a large posterior fossa cyst that is compressing the cerebellar hemispheres, vermis, fourth ventricle (arrow), and brainstem.
-
Dandy-Walker malformation. Joubert syndrome in an 8-month-old boy. The axial CT scan obtained near the pontomesencephalic junction shows a batwing configuration of the fourth ventricle and unusual definition of the superior cerebellar peduncles at this level (arrows). The vermis is dysgenetic, and the 2 cerebellar hemispheres appose each other in the midline.
-
Dandy-Walker malformation. An in utero sonogram of Dandy-Walker malformation; note the abnormal cerebellar vermis in association with a posterior fossa cyst (arrow) and splaying of the cerebellar hemispheres. Image courtesy of Ecker et al.
-
Dandy-Walker malformation. An antenatal sonogram that shows Dandy-Walker malformation (arrow) in a fetus. Courtesy of Umit Aksoy, MD, Uludag University, Bursa, Turkey.
-
Dandy-Walker malformation. An antenatal MRI showing Dandy-Walker malformation in a fetus. Courtesy of Umit Aksoy, MD, Uludag University, Bursa, Turkey.
-
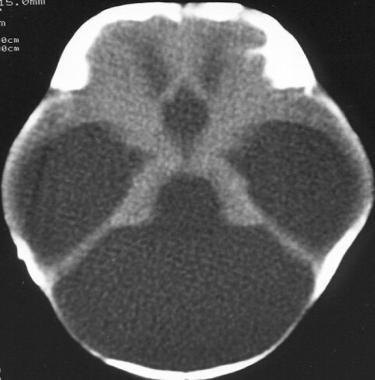
A CT scan depicting Dandy-Walker malformation.
-
Dandy-Walker malformation. An axial CT scan showing the sinus confluence (large arrow) and sinus transversus (small arrows) displaced superiorly in Dandy-Walker malformation (lambdoid-torcular inversion).
