Background
Pulmonary arteriovenous malformations (PAVMs) were first described in 1897. [1] They consist of abnormal communications between the pulmonary arteries and the pulmonary veins. These are also referred to as pulmonary arteriovenous fistulae.
Most patients with pulmonary arteriovenous malformations have the autosomal dominant disease hereditary hemorrhagic telangiectasia (HHT). [2] However, at least 15% of patients with pulmonary arteriovenous malformations do not meet criteria for the diagnosis of HHT and have no other systemic disease. [3] Pulmonary arteriovenous malformations may also be an acquired condition found in patients with liver disease, mainly liver cirrhosis. In these patients, absence of a "hepatic factor" may lead to the development of pulmonary arteriovenous malformations. Patients with congenital heart disease in whom the systemic venous return to the lungs does not include blood return from the hepatic veins also develop pulmonary arteriovenous malformations.
Pulmonary arteriovenous malformations may also be acquired rarely secondary to chronic infections such as schistosomiasis, actinomycosis, tuberculosis, and metastatic thyroid cancer. [2] These arteriovenous malformations may form a communication between pulmonary artery and pulmonary vein or between a bronchial artery and the pulmonary vein.
Hereditary hemorrhagic telangiectasia
Hereditary hemorrhagic telangiectasia (HHT) is an autosomal dominant disorder. The clinical manifestations are secondary to growth of vascular malformations in various organs, most commonly the skin, nasopharynx, GI tract, lungs, and brain. HHT is generally recognized as a classic triad of cutaneous telangiectasia, recurrent epistaxis, and a family history of this disorder [4, 5] (see the image below).
 Mucosal telangiectasias are shown in a patient with hereditary hemorrhagic telangiectasia (HHT).
Mucosal telangiectasias are shown in a patient with hereditary hemorrhagic telangiectasia (HHT).
Approximately 70% of pulmonary arteriovenous malformation cases are associated with HHT. Conversely, approximately 15-35% of persons with HHT have pulmonary arteriovenous malformations. [6]
Anatomy
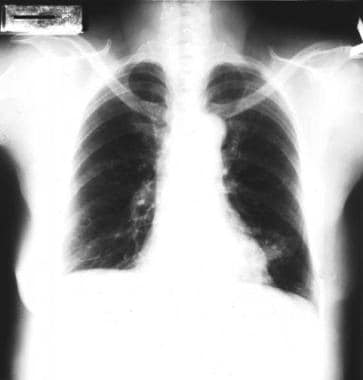
Approximately 53-70% of pulmonary arteriovenous malformations are found in the lower lobes. [7] See the images below.

Approximately 70% of patients have unilateral disease, 36% have multiple lesions, and 50% of those with multiple lesions have bilateral disease. [8] Pulmonary arteriovenous malformations may be microscopic (ie, telangiectasis), but they are typically 1-5 cm. Occasionally, pulmonary arteriovenous malformations as large as 10 cm are encountered. [7] Approximately 10% of patients may have diffuse microvascular pulmonary arteriovenous malformations in combination with larger, radiographically visible pulmonary arteriovenous malformations.
The vascular channels are thin walled and lined with a layer of endothelium. The connective tissue stroma is scant and has no communication with the surrounding lung. Most pulmonary arteriovenous malformations drain into the left atrium, but anomalous drainage to the inferior vena cava or innominate veins has been reported. The malformations may appear as one of the following: a large single sac, a plexiform mass of dilated vascular channels, or a dilated tortuous direct communication between artery and vein.
Anatomy of subtypes
Pulmonary arteriovenous malformations can be classified as simple or complex types on the basis of their architecture. Simple pulmonary arteriovenous malformations have a single feeding segmental artery leading to single draining pulmonary vein. Approximately 80% of pulmonary arteriovenous malformations are of the simple type; [9] most of the associated aneurysms are nonseptate and occur in the lower lobes. Approximately 20% of pulmonary arteriovenous malformations are complex, having two or more feeding arteries or draining veins. [10] They often occur in the lingula and right middle lobe distributions. See the image below.
 Large left lower lobe arteriovenous malformation (AVM) showing a feeding vessel to the left atrium.
Large left lower lobe arteriovenous malformation (AVM) showing a feeding vessel to the left atrium.
Patient Education
Thoroughly educate patients with pulmonary arteriovenous malformations and patients with hereditary hemorrhagic telangiectasia (HHT) about their diagnosis and its clinical implications, complications, and hereditary nature.
Pathophysiology
Physiology
In a pulmonary arteriovenous malformation, blood bypasses the normal oxygen-exchanging pulmonary capillary bed, returning desaturated to the pulmonary veins. When the return of desaturated blood to the pulmonary veins becomes significant, measurable arterial oxygen desaturation and cyanosis results. Because most pulmonary arteriovenous malformations are found in the lower lobes and, in the upright position, more blood is directed to the lower lobes because of gravity, the patient with significant pulmonary arteriovenous malformations demonstrates orthodeoxia, which is a fall in arterial oxygen saturation when in the upright position. If the patient becomes significantly desaturated in the upright position, the patient also demonstrates platypnea, which is dyspnea in the upright position, although this symptom is seen only in advanced cases.
The resultant cyanosis leads to a compensatory rise in hematocrit and hemoglobin concentration roughly proportional to the degree of chronic desaturation. However, bleeding from epistaxis and from gastrointestinal (GI) telangiectasias may reduce the hemoglobin concentrations in patients with HHT and lead to iron deficiency anemia.
Larger arteriovenous malformations allow particles of significant size to pass unfiltered from the systemic venous system to the left atrium and systemic arterial circulation. Stroke from paradoxical embolization is a risk in patients with macroscopic arteriovenous malformations.
Unlike systemic arteriovenous malformations, pulmonary arteriovenous malformations do not lead to high-output cardiac failure even when large. This is because the rate-limiting portion of the circulation is the systemic arterial resistance. Systemic arteriovenous malformations lower the overall total systemic venous resistance and increase venous return, which is a synonym for cardiac output. The pulmonary vascular resistance is normally low and is not rate-limiting. Lowering the total pulmonary vascular resistance further does not increase the cardiac output. See the Cardiac Output and the Pulmonary Vascular Resistance calculators.
A few caveats with this explanation are necessary. First, by causing cyanosis, pulmonary arteriovenous malformations cause the cardiac index to somewhat increase in order to maintain adequate oxygen delivery. Second, liver cirrhosis by itself causes systemic vasodilation and a hyperdynamic circulation, even in the absence of pulmonary arteriovenous malformations. Third, patients with HHT may have other systemic arteriovenous malformations, especially cerebral and hepatic, which may lead to reduced systemic vascular resistance and a high cardiac output state.
In HHT, mutations of two genes make up most cases. Endoglin gene mutations lead to the clinical subtype of HHT-1, and mutations in the activin A receptor type II-like 1 gene (ACVRL1) lead to the clinical subtype HHT-2. Most mutations described are family-specific without a "common mutation" pattern that is often seen in other inherited conditions.
Endoglin and ACVRL-1 bind tumor growth factor-beta (TGFβ), which is implicated in angiogenesis. Pulmonary arteriovenous malformations likely develop as a result of interplay of various factors among diverse cells and matrix during vascular insults. Changes in endoglin and ALK might cause endothelial cells to respond abnormally to TGFβ during the process of vascular remodeling, resulting in the formation of arteriovenous malformations.
The pathogenesis of pulmonary arteriovenous malformations in liver and congenital cardiac disease is not understood. A postulated absence of "hepatic factor" is made based on the following observations:
-
In congenital heart disease where the pulmonary circulation lacks any component from the hepatic veins (ie, following a Glenn-type palliation in which the superior vena cava is directly connected to the pulmonary arteries as the sole source of pulmonary blood flow), pulmonary arteriovenous malformations begin to develop after several years and enlarge further if no change is made to the circulation.
-
Some patients with liver disease, mainly cirrhosis, develop pulmonary arteriovenous malformations. Initially, these are microscopic and progress in the absence of intervention to larger macroscopic arteriovenous malformations.
-
Patients with congenital cardiac disease with a Glenn-type circulation have regression of small pulmonary arteriovenous malformations if venous return from the hepatic veins is provided to the pulmonary circulation. Larger pulmonary arteriovenous malformations may not regress, implying a threshold over which humoral control is no longer possible.
-
Patients with liver disease who develop pulmonary arteriovenous malformations have regression of the pulmonary arteriovenous malformations if they undergo liver transplantation. Patients with extensive pulmonary arteriovenous malformations due to liver disease and significant arterial desaturation at rest may not be candidates for liver transplantation because of the very high mortality in this setting.
-
In the early phases of progression of arteriovenous malformations seen in both congenital heart disease and liver disease, administration of 100% oxygen usually overcomes the A-a gradient, and the patient becomes fully saturated with a high PaO2. This implies that the pathophysiology of the arteriovenous malformations in these conditions is dilation of the normal capillary bed.
-
In the early phases, a normal PAO2 is insufficient to overcome the diffusion gradient to the center of these dilated beds, resulting in some desaturation and an A-a gradient. However, with administration of 100% FiO2, the A-a gradient may be overcome, and the PaO2 increases to near-expected levels, abolishing the A-a gradient. In later stages, when the arteriovenous malformations become macroscopic, even 100% FiO2 does not overcome the A-a gradient, and the patient remains desaturated. See the A-a Gradient calculator.
Pathogenesis
The exact pathogeneses of pulmonary arteriovenous malformations is unknown. In the terminal arterial loops, a defect that allows dilatation of the thin-walled capillary sacs may occur. Alternatively, pulmonary arteriovenous malformations are the result of incomplete resorption of the vascular septa that separate the arterial and venous plexus, which normally anastomose during fetal development. Some have also suggested that multiple small pulmonary arteriovenous malformations develop as a result of capillary development failure during fetal growth. The large saccular pulmonary arteriovenous malformations develop by means of progressive dilation of the smaller plexus, leading to the formation of tortuous loops and multiloculated sacs. With time, the intervening vascular walls may rupture, resulting in the formation of a single large saccular pulmonary arteriovenous malformation.
Natural history
The natural history of pulmonary arteriovenous malformations has not been studied carefully. The initial manifestation of HHT is the appearance of cutaneous telangiectases or epistaxis. Fewer than 10% of patients who have visceral involvement by arteriovenous malformations have visceral signs and symptoms (eg, dyspnea or GI bleeding) as the initial manifestation of HHT. The visceral manifestations occur in adults, reflecting the additional time needed for the enlargement of arteriovenous malformations.
In one study of 16 patients, serial chest radiographs obtained over a median observation period of 18.9 years demonstrated enlargement in 4 patients and near total regression in 1 patient. The growth rate tended to be slow, with an increase of approximately 5-10 mm every 5-15 years.
Etiology
Epidemiology
Great heterogeneity of symptoms is noted among different families and within single large families with HHT. Some families with HHT predominantly have pulmonary arteriovenous malformations and cerebral arteriovenous malformations, whereas other affected families predominantly have GI mucosal telangiectasis, which lead to GI bleeding and iron-deficiency anemia.
Inheritance
HHT is an autosomal dominant disorder; however, 20% of cases involve no family history of telangiectasia or recurrent bleeding. Penetrance is age related and nearly complete by age 40 years. Although the arteriovenous malformations in HHT are inherited and should be present at birth, they commonly manifest clinically during adult life, after the vessels have been subjected to pressure for several decades.
Associated syndromes
Communication between pulmonary arteries and pulmonary veins has been reported in cases of trauma and in hepatic cirrhosis, schistosomiasis, mitral stenosis, actinomycosis, Fanconi syndrome, and metastatic thyroid carcinoma. Communications between bronchial arteries and pulmonary arteries that cause a left-to-right shunt develop in chronic inflammatory conditions such as bronchiectasis. Most individuals with pulmonary arteriovenous malformations have HHT. The diagnostic criteria for a definite diagnosis of HHT include at least three of the following:
-
Recurrent and spontaneous epistaxis
-
Multiple mucocutaneous telangiectases
-
Visceral lesions (eg, GI arteriovenous malformations, pulmonary arteriovenous malformations)
-
First-degree relative with HHT by these criteria
Associated noncardiac conditions
The most frequently reported associated noncardiac conditions are CNS complications, which occur in 30% of patients. Strokes occur in 18% of patients with CNS complications, transient ischemic attacks occur in 37%, brain abscesses occur in 9%, migraine headaches occur in 43%, and seizures occur in 8%. Paradoxic embolism across pulmonary arteriovenous malformations is the most likely mechanism for major noninfectious strokes. Embolism of infected material accounts for solitary or recurrent brain abscesses. These complications most commonly occur when the feeding arteries are larger than 3 mm in diameter. Hemoptysis and hemothorax are other potentially life-threatening complications. Hemoptysis occurs from ruptured pulmonary arteriovenous malformations or endobronchial telangiectasia.
Idiopathic congenital pulmonary arteriovenous malformations
Idiopathic congenital pulmonary arteriovenous malformations are likely to be single. They are less likely to become enlarged, and the are associated with fewer physical findings than other pulmonary arteriovenous malformations. Idiopathic pulmonary arteriovenous malformations are diagnosed by using the same criteria as for other pulmonary arteriovenous malformations. Idiopathic congenital pulmonary arteriovenous malformations are successfully treated with embolotherapy.
Acquired arteriovenous malformations in hepatopulmonary syndrome
Hepatopulmonary syndrome (HPS), increased alveolar-arterial oxygen gradient (see the A-a Gradient calculator), and intrapulmonary right-to-left shunting (defined as the triad of liver disease) may occur in as many as 47% of patients with end-stage liver disease. All types of chronic liver disease may give rise to this syndrome. Approximately 80% of affected patients have signs and symptoms of end-stage liver disease before symptoms from pulmonary arteriovenous malformations develop. These patients have dyspnea, platypnea, clubbing, cyanosis, hypoxia, and orthodeoxia. Pulmonary function results indicate normal lung volumes and expiratory flow rates with low diffusing capacity.
In contrasts to patients with HHT, patients with HPS rarely have discrete arteriovenous malformations on chest radiographs. The calculation of the shunt fraction with the use of 100% oxygen, contrast echocardiography, and radionuclide scanning are diagnostic tests for HPS.
Results of HPS management have been disappointing. Liver transplantation may result in the resolution of HPS, and HPS is not a contraindication to liver transplantation. An improvement in HPS-related pulmonary shunting after therapeutic transjugular intrahepatic portosystemic shunting has been described.
Acquired arteriovenous malformations after surgery for congenital cyanotic heart disease
Pulmonary arteriovenous malformations may develop after Glenn or modified Fontan procedures for congenital cyanotic heart disease. Pulmonary arteriovenous malformations are a known late complication of Glenn anastomosis (ie, superior vena cava [SVC] to right pulmonary artery [RPA]), which occur in as many as 25% of cases. The Fontan operation (ie, SVC to right atrium and proximal RPA; hepatic veins to left pulmonary artery) was designed as a surgical repair for congenital tricuspid atresia. Contrast echocardiography and radionuclide shunt studies have been used to diagnose pulmonary arteriovenous malformations, and embolotherapy has been used successfully to occlude the pulmonary arteriovenous malformations in these cases.
Epidemiology
United States data
In a 1953 study from The Johns Hopkins Hospital, 3 cases of pulmonary arteriovenous malformations were detected in 15,000 consecutive autopsies. The Mayo Clinic encountered 63 cases during the 20 years ending in 1972, and 38 cases were encountered during the subsequent 9 years ending in 1981. Approximately 70% of the cases of pulmonary arteriovenous malformations are associated with HHT, which is an autosomal dominant disorder. Conversely, approximately 15-35% of persons with HHT have pulmonary arteriovenous malformations.
To screen for occult brain, lung, and liver arteriovenous malformations in pediatric patients with confirmed HHT, a study undertook molecular analysis and clinical assessment. [11] The molecular analysis demonstrated the mutation-carrier status in 22 of 35 children. Nasal telangiectases were found in 68%, mucocutaneous telangiectases (fingers, lips, oral cavity) in 79%, pulmonary arteriovenous malformations in 53%, hepatic arteriovenous malformations (HAVMs) in 47%, and cerebral arteriovenous malformations and/or cerebral ischemic changes secondary to pulmonary arteriovenous malformations in 12%.
Sex- and age-related demographics
Pulmonary arteriovenous malformations occur twice as often in women than in men, but a male predominance is observed among newborns.
Approximately 10% of the cases of pulmonary arteriovenous malformations are identified in infancy or childhood; however, the incidence gradually increases through the fifth and sixth decades of life.
Prognosis
Morbidity/mortality
Mortality of pulmonary arteriovenous malformations is somewhat difficult to determine because of the association in many with HHT. Patients with HHT may also have arteriovenous malformations in the liver and head, as well as intestinal telangiectasias that also put them at risk for premature mortality.
Mortality caused by pulmonary arteriovenous malformations is due to rupture, brain abscess, and stroke due to paradoxical embolization. In addition, therapeutic interventions for pulmonary arteriovenous malformations carry a low risk of mortality.
The risk of mortality appears to be significantly higher in patients with bilateral, diffuse pulmonary arteriovenous malformations. In study of 26 patients followed for 27 years with diffuse bilateral pulmonary arteriovenous malformations, 2 died of complications related to the pulmonary arteriovenous malformations directly: one due to hemoptysis from rupture, and the other from cerebral abscess. [12] Seven others died from other organ involvement with HHT.
Complications
The following complications may occur in patients with pulmonary arteriovenous fistulas:
-
Seizure
-
Migraine headaches
-
Transient ischemic attack
-
Cerebral vascular accident
-
Brain abscess
-
Hypoxemia, orthodeoxia
-
Hemothorax
-
Life-threatening hemoptysis
-
Pulmonary hypertension
-
Congestive heart failure
-
Polycythemia
-
Anemia
-
Infectious endocarditis
-
Mucosal telangiectasias are shown in a patient with hereditary hemorrhagic telangiectasia (HHT).
-
Left lower lobe arteriovenous malformation (AVM).
-
Lateral radiograph showing a left lower lobe arteriovenous malformation (AVM).
-
Large left lower lobe arteriovenous malformation (AVM) showing a feeding vessel to the left atrium.
-
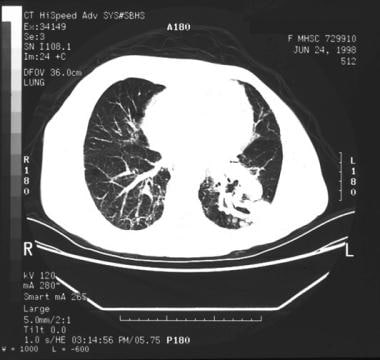
Another view of the infused CT scan of the left lower lobe arteriovenous malformation (AVM).
-
Pulmonary angiographic findings are required not only to confirm the diagnosis but also to plan therapeutic embolization.
-
Small arteriovenous malformations (AVMs) in the right and left lower lobes.
-
Lateral radiograph shows a left lower lobe arteriovenous malformation (AVM).
-
Contrast-enhanced CT scan showing a left lower lobe arteriovenous malformation (AVM).
-
Right lower lobe arteriovenous malformation (AVM).
-
CT scan obtained after coil embolotherapy.
-
Left lower lobe embolotherapy performed at the same sitting as the coil embolotherapy depicted in the previous image.
