Practice Essentials
Ankylosing spondylitis is a distinct disease entity characterized by inflammation of multiple articular and para-articular structures, frequently resulting in bony ankylosis. The term ankylosing is derived from the Greek word ankylos, meaning stiffening of a joint; the term spondylos means vertebra. Spondylitis refers to inflammation of one or more vertebrae. Ankylosing spondylitis (see the radiograph below) usually is classified as a chronic and progressive form of seronegative arthritis. Ankylosing spondylitis has a predilection for the axial skeleton, affecting particularly the sacroiliac and spinal facet joints and the paravertebral soft tissues. Patients with ankylosing spondylitis have a twofold increased incidence of vertebral fragility fractures and are at increased risk for atlantoaxial subluxation, spinal cord injury, and, rarely, cauda equina syndrome. Extraspinal manifestations of the disease include inflammatory bowel disease, acute anterior uveitis, psoriasis, cardiovascular disease, peripheral arthritis, iritis, and pulmonary involvement. [1, 2, 3, 4]
 Bilateral sacroiliitis. Frontal radiograph shows bilateral sacroiliac joint erosions and iliac side subchondral sclerosis.
Bilateral sacroiliitis. Frontal radiograph shows bilateral sacroiliac joint erosions and iliac side subchondral sclerosis.
Preferred examination
Radiographs are the single most important imaging technique for the detection, diagnosis, and follow-up monitoring of patients with ankylosing spondylitis. Overall bony morphology and subtle calcifications and ossifications may be demonstrated well radiographically. The diagnosis may be reliably made if the typical radiographic features of ankylosing spondylitis are present. [5, 6, 7, 8] Radiographs are limited in detecting early sacroiliitis and in demonstrating subtle changes in the posterior elements of the vertebrae. [9, 4]
The European League Against Rheumatism (EULAR) recommends conventional radiography of the sacroiliac joints as the first imaging method to diagnose sacroiliitis as part of axial spondyloarthritis in the majority of cases. MRI of the SI joints is considered an alternative in some cases, such as in young patients and in those with a short duration of symptoms. [3, 4]
Computed tomography (CT) scanning is useful in selected situations (eg, in equivocal cases of sacroiliitis and in cases in which subtle radiographic changes are present) and in the evaluation of complications. Although CT scanning is useful in evaluating sacroiliitis, normal variations of the sacroiliac joints may simulate the findings of inflammation. Because of its high radiation dose, CT scanning is not ideal for imaging long segments of the spine. In patients with advanced ankylosing spondylitis, multidetector CT (MDCT) scanning is the imaging modality of choice for the evaluation of fractures of the cervical spine. [3, 9, 4]
Magnetic resonance imaging (MRI) is useful in assessing early cartilage abnormalities and bone marrow edema. MRI has revealed a very early clinical phase of the disease in which there is symptomatic axial involvement but no structural changes. [10, 11, 12, 9, 13]
Ultrasound helps identify the anatomic landmarks in patients with ankylosing spondylitis before regional anesthesia and makes it easier to perform the blockade with minimal number of attempts. [14] It may also be used for assessing spinal mobility. [15]
European League Against Rheumatism (EULAR) guidelines
EULAR guidelines recommend conventional radiography of the sacroiliac joints as the first imaging method to diagnose sacroiliitis as part of axial spondyloarthritis in the majority of cases. MRI of the SI joints is considered an alternative in some cases, such as in young patients and in those with a short duration of symptoms. EULAR also recommends MRI of the SI joints for patients in whom clinical features and conventional radiography findings are not diagnostic but axial spondyloarthritis is still suspected. On MRI, findings to consider include both active inflammatory lesions (primarily bone marrow edema) and structural lesions (eg, bone erosion, new bone formation, sclerosis and fat infiltration). CT may provide additional information on structural damage if conventional radiography is negative and MRI cannot be performed. Scintigraphy and ultrasound are not recommended for diagnosis of sacroiliitis as part of axial spondyloarthropathy. [3, 9]
Radiography
Sacroiliitis occurs early in the course of ankylosing spondylitis and is regarded as a hallmark of the disease. In patients with ankylosing spondylitis (not non-radiographic axial SpA), initial conventional radiography of the lumbar and cervical spine can detect syndesmophytes, which are predictive of development of new syndesmophytes. MRI (vertebral corner inflammatory or fatty lesions) may also be used to predict development of new radiographic syndesmophytes. [3]
Protrusio acetabuli develops in as many as one third of patients. Bony ankylosis eventually may occur. At the glenohumeral joint, the joint space narrows uniformly, and a large erosion may be present in the upper greater tuberosity.
Knee changes consist of uniform joint space narrowing and surrounding bony proliferation. In the hands, the joints usually are involved asymmetrically. Erosions are smaller and shallower. Marginal periostitis is seen, and bony density usually is preserved.
Lung manifestations of ankylosing spondylitis are seen as progressive fibrosis and bullous changes at the apices. On radiographs, chest lesions may resemble tuberculous infection. Lung bullae may be complicated by infection by Aspergillus species and other opportunistic infections. Lung changes usually are seen several years after joint disease develops.
Radiographically, the earliest sign of sacroiliitis is indistinctness of the joint. The joints initially widen before they narrow.
Subchondral bony erosions on the iliac side of the joint are seen; these are followed by subchondral sclerosis and bony proliferation (see the image below).
Bilateral sacroiliitis. Frontal radiograph shows bilateral sacroiliac joint erosions and iliac side subchondral sclerosis.
With eventual bony fusion (seen in the image below), the sclerosis resolves.
 Bilateral chronic sacroiliitis. Frontal radiograph shows complete fusion of both sacroiliac joints.
Bilateral chronic sacroiliitis. Frontal radiograph shows complete fusion of both sacroiliac joints.
At the end stage, the sacroiliac joint may be seen as a thin, dense line, or it may not be visible at all.
Sacroiliitis typically is symmetrical, although it may be asymmetrical in the early stages of the disease.
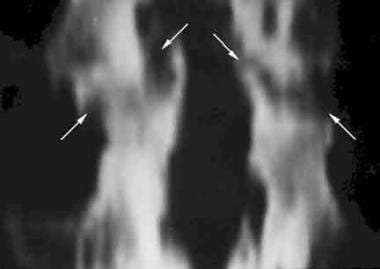
In the spine, the early stages of spondylitis are manifested as small erosions at the corners of the vertebral bodies. The areas are surrounded by reactive sclerosis and have been termed the shiny corner sign, or Romanus lesion (see the image below).
 Lateral radiograph shows anterior corner erosions at the T12 and L1 vertebral bodies. The typical shiny corner sign (or Romanus lesion) is present (arrows).
Lateral radiograph shows anterior corner erosions at the T12 and L1 vertebral bodies. The typical shiny corner sign (or Romanus lesion) is present (arrows).
Squaring of the vertebral body is another characteristic feature of ankylosing spondylitis; it is caused by a combination of corner erosions and periosteal new bone formation along the anterior aspect of the vertebral body. This is best seen in the lumbar spine, in which the anterior cortex of the vertebral body normally is concave.
This is followed by syndesmophyte formation, in which ossification of the outer fibers of the annulus fibrosis leads to bridging of the corners of one vertebra to another (see the image below).
 Vertebral body squaring. Lateral radiograph shows squaring of L3 and L4 vertebral bodies, L3-L4 anterior syndesmophyte, and lumbar facet joint fusion.
Vertebral body squaring. Lateral radiograph shows squaring of L3 and L4 vertebral bodies, L3-L4 anterior syndesmophyte, and lumbar facet joint fusion.
Ossification of the adjacent paravertebral connective tissue fibers also occurs. Posterior interspinous ligament ossification, combined with linking of the spinous process, produces an appearance of a solid midline, vertical, dense line on frontal radiographs (see the image below).
 Interspinous ossification. Frontal radiograph shows T12-L2 lateral syndesmophytes and interspinous ligament ossification extending from the T12 to L1 and L2 to L4 levels.
Interspinous ossification. Frontal radiograph shows T12-L2 lateral syndesmophytes and interspinous ligament ossification extending from the T12 to L1 and L2 to L4 levels.
The apophyseal and costovertebral joints frequently are affected by erosions and eventually undergo fusion (see the image below).
 Vertebral fusion. Lateral radiograph shows solid ankylosis of all cervical facet joints from C2 downwards. Extensive anterior and posterior syndesmophytes are noted.
Vertebral fusion. Lateral radiograph shows solid ankylosis of all cervical facet joints from C2 downwards. Extensive anterior and posterior syndesmophytes are noted.
Complete fusion of the vertebral bodies by syndesmophytes and other related ossified areas produces bamboo spine (see the image below).
 Bamboo spine. Frontal radiograph shows complete fusion of the vertebral bodies. Extensive facet joint ankylosis and posterior ligamentous ossification produce the trolley track appearance.
Bamboo spine. Frontal radiograph shows complete fusion of the vertebral bodies. Extensive facet joint ankylosis and posterior ligamentous ossification produce the trolley track appearance.
Calcifications of the disk may occur at single or multiple levels; they are usually associated with apophyseal joint ankylosis and adjacent syndesmophytes (see the image below).
 Disk calcification. Lateral radiograph shows L2-L3 and L3-L4 disk calcifications, as well as L2-L4 anterior syndesmophytes.
Disk calcification. Lateral radiograph shows L2-L3 and L3-L4 disk calcifications, as well as L2-L4 anterior syndesmophytes.
For patients with established ankylosing spondylitis, fractures usually occur at the thoracolumbar (see the first image below) and cervicothoracic junctions. Upper cervical spine fractures and atlantoaxial subluxation rarely are seen. Fractures typically are transverse, extend from anterior to posterior, and frequently pass through the ossified disk. They have been termed chalk stick fractures (see the second image below).
 Thoracolumbar junction fracture. Lateral radiograph shows features of established ankylosing spondylitis. A T12 vertebral body fracture is noted, with disruption of the ossified anterior longitudinal ligament (arrow). An old L1 compression fracture is present.
Thoracolumbar junction fracture. Lateral radiograph shows features of established ankylosing spondylitis. A T12 vertebral body fracture is noted, with disruption of the ossified anterior longitudinal ligament (arrow). An old L1 compression fracture is present.
 Chalk stick fracture. Lateral radiograph shows a fracture through the ankylosed cervical spine, producing a gap at the C6-C7 disk.
Chalk stick fracture. Lateral radiograph shows a fracture through the ankylosed cervical spine, producing a gap at the C6-C7 disk.
Pseudoarthrosis is seen radiographically as areas of diskovertebral destruction and adjacent sclerosis. The changes, which are referred to as the Andersson lesion, may resemble disk infection, although pseudoarthrosis usually develops secondarily to a previously undetected fracture or at an unfused segment. Therefore, an important imaging feature is the involvement of the posterior elements, seen as a linear, hypodense area with sclerotic borders (see the image below).
 Pseudoarthrosis. Lateral radiograph shows a T11-T12 diskovertebral lesion with adjacent sclerosis (Andersson lesion; arrow). Posterior element defect is present (arrowheads). The patient also has a severe kyphotic deformity.
Pseudoarthrosis. Lateral radiograph shows a T11-T12 diskovertebral lesion with adjacent sclerosis (Andersson lesion; arrow). Posterior element defect is present (arrowheads). The patient also has a severe kyphotic deformity.
Enthesopathy is seen radiographically as ill-defined erosions with adjacent sclerosis at the sites of ligamentous and tendinous attachments. With healing, sclerosis decreases and new bone proliferation occurs. Lesions typically are bilateral and symmetrical in distribution. Enthesopathic changes are particularly prominent at certain sites around the pelvis, such as the ischial tuberosity (see the first image below), iliac crest, and femoral trochanters. Other locations include the coracoclavicular ligament attachment site to the inferior clavicle (see the second image below), humeral tuberosity, anterior patella, and plantar aspect of the calcaneum.
 Pelvic enthesopathy. Frontal radiograph shows ill-defined erosions with adjacent sclerosis at the left ischial tuberosity and more established new bone formation on the right side.
Pelvic enthesopathy. Frontal radiograph shows ill-defined erosions with adjacent sclerosis at the left ischial tuberosity and more established new bone formation on the right side.
 Shoulder enthesopathy. Frontal radiograph shows irregular bony proliferation at the coracoclavicular ligament attachment sites to the inferior clavicle and the superior coracoid process.
Shoulder enthesopathy. Frontal radiograph shows irregular bony proliferation at the coracoclavicular ligament attachment sites to the inferior clavicle and the superior coracoid process.
Hip joint involvement typically is bilateral and symmetrical. The hip joint space is narrowed uniformly. Axial migration of the femoral head occurs, and a collar of osteophytes may be seen at the femoral head-neck junction (see the image below).
 Hip joint changes. Frontal radiograph shows uniform joint space narrowing and a collar of osteophytes at the femoral head-neck junction. Left sacroiliac joint ankylosis is present.
Hip joint changes. Frontal radiograph shows uniform joint space narrowing and a collar of osteophytes at the femoral head-neck junction. Left sacroiliac joint ankylosis is present.
Degree of confidence
Radiographs are a reliable means with which to make a diagnosis, particularly if typical radiographic features are present.
The sacroiliitis associated with ankylosing spondylitis should be differentiated from sacroiliitis caused by other diseases. Bilateral, symmetrical sacroiliac joint disease may be found in conditions such as psoriasis, Reiter disease, enteropathic arthropathy, hyperparathyroidism, and osteitis condensans ilii.
Ankylosing spondylitis also may present as a bilateral, asymmetrical sacroiliitis, mimicking psoriasis, Reiter disease, rheumatoid arthritis, and gouty arthritis. Unilateral distribution of sacroiliac disease also may be found in infective arthritis. Therefore, it is important that radiographic features be carefully analyzed to look for signs of various diseases and that radiographic features be correlated with the overall pattern of bony involvement and with clinical findings.
Spinal abnormalities found in ankylosing spondylitis may be encountered in other diseases, such as enteropathic arthropathy, psoriasis, and Reiter disease. Careful analysis and classification of bony outgrowths in the vertebrae are helpful in differentiating the various conditions. In addition to ankylosing spondylitis, syndesmophytes are found in alkaptonuria. Flowing anterior ossification is a feature of diffuse idiopathic skeletal hyperostosis, whereas paravertebral ossification is present in psoriasis and Reiter disease.
Spinal pseudoarthrosis in ankylosing spondylitis often produces marked, destructive diskovertebral changes that may resemble infective spondylodiskitis. The presence of posterior element fracture or defect is an important distinguishing clue.
Computed Tomography
CT scanning may be useful in selected patients in whom ankylosing spondylitis is suggested and in whom initial sacroiliac joint radiographs findings are normal or equivocal. Features such as joint erosions, subchondral sclerosis (see the image below), and bony ankylosis are visualized better on CT scans than on radiographs; however, some normal variants of the sacroiliac joint may simulate the features of sacroiliitis. [3, 16, 17, 4, 18, 19]
 Bilateral sacroiliitis. Axial CT scan shows erosions and iliac side subchondral sclerosis of both sacroiliac joints.
Bilateral sacroiliitis. Axial CT scan shows erosions and iliac side subchondral sclerosis of both sacroiliac joints.
CT scanning supplements bone scintigraphy in evaluating areas of increased uptake, particularly in the spine. Fractures, vertebral scalloping from dural ectasia (see the first image below), and the bony lesions seen in conditions such as pseudoarthrosis (see the second and third images below), spinal canal stenosis, and facet inflammatory disease are detected well using CT scanning, particularly in reformatted coronal, sagittal, or oblique images.
 Dural ectasia. Axial postmyelographic CT scan shows prominent dural ectasia with scalloping of the adjacent vertebra. Partial fusion of the facet joints is noted.
Dural ectasia. Axial postmyelographic CT scan shows prominent dural ectasia with scalloping of the adjacent vertebra. Partial fusion of the facet joints is noted.
 Pseudoarthrosis. Reconstructed midsagittal CT image shows an L1-L2 diskovertebral lesion with adjacent sclerosis.
Pseudoarthrosis. Reconstructed midsagittal CT image shows an L1-L2 diskovertebral lesion with adjacent sclerosis.
 Pseudoarthrosis (same patient as in the previous image). Reconstructed posterior coronal CT image shows bilateral posterior element breaks (arrows).
Pseudoarthrosis (same patient as in the previous image). Reconstructed posterior coronal CT image shows bilateral posterior element breaks (arrows).
Other useful applications of CT scanning include the assessment of atlantoaxial instability, costovertebral disease, manubriosternal disease, and paraspinal muscle atrophy.
Multidetector CT (MDCT) scanning can show more injuries than radiography and MRI can, and it yields more information on fracture morphology. In patients with advanced ankylosing spondylitis, MDCT scanning is the imaging modality of choice for the evaluation of fractures of the cervical spine. It complements MRI, which better shows spinal cord and soft-tissue injuries.
According to one study, the use of MDCT in patients with ankylosing spondylitis may also be beneficial for the evaluation of pulmonary disease, even in asymptomatic patients who do not have pulmonary function test abnormalities and in those in the early stages of disease. [20]
Magnetic Resonance Imaging
MRI may have a role in the early diagnosis of sacroiliitis. Detection of synovial enhancement on MRI has been found to correlate with disease activity, as measured by laboratory inflammatory markers. MRI (vertebral corner inflammatory or fatty lesions) may also be used to predict development of new radiographic syndesmophytes. [3] Advantages of MRI include direct visualization of cartilage abnormalities, detection of bone marrow edema, improved detection of erosions, and the absence of ionizing radiation. Yu et al found MRI to be more sensitive than either radiography or CT scanning in the detection of early cartilage changes and bone marrow edema of the sacroiliac joints. [21] Although sensitive in the detection of sacroiliitis, MRI is not specific for diagnosing ankylosing spondylitis as the cause of sacroiliitis. [13]
MRI has been found to be superior to CT scanning in the detection of cartilage changes, bone erosions, and subchondral bone changes. [22] MRI is also sensitive in the assessment of activity in relatively early disease. Affected sites include the diskovertebral junction and the peripheral joints. In general, areas of increased T2 signal correlate with the presence of edema or vascularized fibrous tissue. [23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 12]
In established disease, MRI detects pseudoarthrosis, diverticula associated with cauda equina syndrome, and spinal canal stenosis. In patients with complications of fracture or pseudoarthrosis, MRI is useful in the assessment of spinal canal compromise and cord injury (see the images below).
 Pseudoarthrosis. Sagittal T1-weighted MRI shows a prominent T11-T12 diskovertebral lesion (arrows) with posterior element involvement (arrowheads).
Pseudoarthrosis. Sagittal T1-weighted MRI shows a prominent T11-T12 diskovertebral lesion (arrows) with posterior element involvement (arrowheads).
 Pseudoarthrosis (same patient as in the previous image). Sagittal T2-weighted image shows the linear area of high signal intensity extending obliquely from the T11-T12 diskovertebral lesion (arrows) to the posterior elements (arrowheads).
Pseudoarthrosis (same patient as in the previous image). Sagittal T2-weighted image shows the linear area of high signal intensity extending obliquely from the T11-T12 diskovertebral lesion (arrows) to the posterior elements (arrowheads).
MRI may be used to assess the integrity of intervertebral disks and spinal ligaments in cases involving spinal fractures. MRI is considered to be mandatory for patients with neurologic symptoms, especially for patients who experience a symptom-free interval and for those who experience neurologic deterioration after established spinal cord injury.
MRI may be useful in the early diagnosis of inflammatory changes in the feet of patients with ankylosing spondylitis. MRI may detect erosive bone, soft-tissue, cartilage, tendon, and joint abnormalities, even in patients who do not have clinical signs and symptoms of foot involvement.
MRI has been found to have a role in monitoring the treatment of patients with active ankylosing spondylitis. The degree of spinal inflammation may be detected before and after therapy with drugs such as the tumor necrosis factor-alpha receptor fusion protein etanercept and the interleukin-1 receptor antagonist anakinra.
In a study of patients with ankylosing spondylitis, whole-body MRI showed that disease activity significantly decreased with anti-TNF (etanercept) therapy. Whole-body MRI was also able to detect more inflammatory lesions than clinical examination alone. The results of this study suggested that whole-body MRI improves the detection of inflammatory changes and the assessment of the course of those changes under anti-TNF therapy. [33]
Nuclear Imaging
Bone scintigraphy may be helpful for patients with suggested ankylosing spondylitis in whom radiographic findings are normal or equivocal. Qualitative assessment of the accumulation of radionuclides in the sacroiliac region may be difficult because of normal uptake in the location. Quantitative analysis may be more useful in these patients. Ratios of sacroiliac joint–to-sacral uptake of 1.3:1 or more are considered abnormal (see the image below). [34, 35]
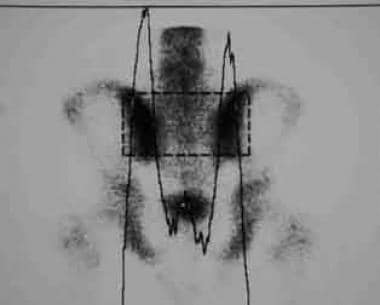 Quantitative scintigraphy. Increased sacroiliac joint uptake is seen, with a sacroiliac joint–to-sacral uptake ratio that exceeds 1.7:1 on each side.
Quantitative scintigraphy. Increased sacroiliac joint uptake is seen, with a sacroiliac joint–to-sacral uptake ratio that exceeds 1.7:1 on each side.
An increase in bone scintigraphic uptake also may be useful in the evaluation of active disease. Sites affected include the peripheral joints and entheses. An important application is in patients with long-standing disease who develop new pain, with or without a recent history of trauma. Focal areas of uptake may indicate a fracture or pseudoarthrosis. Application of single-photon emission CT (SPECT) scintiscans may help to better localize the structures involved. In these patients, the sites of increased scintigraphic uptake must be correlated with further imaging by radiography, tomography, or CT scanning.
Degree of confidence
Scintigraphy has high sensitivity but low specificity in the diagnosis of sacroiliitis. Several factors potentially affect calculation of the sacroiliac joint-to-sacrum ratio. These factors include a prominent sacral tubercle that may produce increased uptake in the sacrum and the influence of age and sex on radionuclide uptakes in the sacroiliac joints and sacrum. In patients with advanced disease, the radionuclide uptake may not appear abnormal.
Although sensitive in the detection of active disease in the spine, increased radionuclide accumulation is not specific for the diagnosis of ankylosing spondylitis. Correlation with other radiologic and clinical findings is important.
-
Bilateral sacroiliitis. Frontal radiograph shows bilateral sacroiliac joint erosions and iliac side subchondral sclerosis.
-
Bilateral chronic sacroiliitis. Frontal radiograph shows complete fusion of both sacroiliac joints.
-
Lateral radiograph shows anterior corner erosions at the T12 and L1 vertebral bodies. The typical shiny corner sign (or Romanus lesion) is present (arrows).
-
Vertebral body squaring. Lateral radiograph shows squaring of L3 and L4 vertebral bodies, L3-L4 anterior syndesmophyte, and lumbar facet joint fusion.
-
Interspinous ossification. Frontal radiograph shows T12-L2 lateral syndesmophytes and interspinous ligament ossification extending from the T12 to L1 and L2 to L4 levels.
-
Vertebral fusion. Lateral radiograph shows solid ankylosis of all cervical facet joints from C2 downwards. Extensive anterior and posterior syndesmophytes are noted.
-
Bamboo spine. Frontal radiograph shows complete fusion of the vertebral bodies. Extensive facet joint ankylosis and posterior ligamentous ossification produce the trolley track appearance.
-
Disk calcification. Lateral radiograph shows L2-L3 and L3-L4 disk calcifications, as well as L2-L4 anterior syndesmophytes.
-
Thoracolumbar junction fracture. Lateral radiograph shows features of established ankylosing spondylitis. A T12 vertebral body fracture is noted, with disruption of the ossified anterior longitudinal ligament (arrow). An old L1 compression fracture is present.
-
Chalk stick fracture. Lateral radiograph shows a fracture through the ankylosed cervical spine, producing a gap at the C6-C7 disk.
-
Pseudoarthrosis. Lateral radiograph shows a T11-T12 diskovertebral lesion with adjacent sclerosis (Andersson lesion; arrow). Posterior element defect is present (arrowheads). The patient also has a severe kyphotic deformity.
-
Pelvic enthesopathy. Frontal radiograph shows ill-defined erosions with adjacent sclerosis at the left ischial tuberosity and more established new bone formation on the right side.
-
Shoulder enthesopathy. Frontal radiograph shows irregular bony proliferation at the coracoclavicular ligament attachment sites to the inferior clavicle and the superior coracoid process.
-
Hip joint changes. Frontal radiograph shows uniform joint space narrowing and a collar of osteophytes at the femoral head-neck junction. Left sacroiliac joint ankylosis is present.
-
Bilateral sacroiliitis. Axial CT scan shows erosions and iliac side subchondral sclerosis of both sacroiliac joints.
-
Pseudoarthrosis. Reconstructed midsagittal CT image shows an L1-L2 diskovertebral lesion with adjacent sclerosis.
-
Pseudoarthrosis (same patient as in the previous image). Reconstructed posterior coronal CT image shows bilateral posterior element breaks (arrows).
-
Bilateral facet joint ankylosis. Axial CT scan shows complete fusion of both T12-L1 facet joints.
-
Dural ectasia. Axial postmyelographic CT scan shows prominent dural ectasia with scalloping of the adjacent vertebra. Partial fusion of the facet joints is noted.
-
Pseudoarthrosis. Sagittal T1-weighted MRI shows a prominent T11-T12 diskovertebral lesion (arrows) with posterior element involvement (arrowheads).
-
Pseudoarthrosis (same patient as in the previous image). Sagittal T2-weighted image shows the linear area of high signal intensity extending obliquely from the T11-T12 diskovertebral lesion (arrows) to the posterior elements (arrowheads).
-
Quantitative scintigraphy. Increased sacroiliac joint uptake is seen, with a sacroiliac joint–to-sacral uptake ratio that exceeds 1.7:1 on each side.
