Practice Essentials
The appendix is a blind-ending tubular structure arising from the cecum. Appendicitis results from an acute inflammation of the appendix and creates the most common abdominal surgical emergency. Acute appendicitis is a common gastrointestinal disease affecting 5.7–57 per 100.000 individuals each year, with the highest incidence being in children and adolescents. [1] Imaging studies in patients with a clinical suspicion of acute appendicitis can reduce the negative appendectomy rate, which has been reported to be as high as 15%. [2]
(A color Doppler ultrasonogram of appendicitis is shown below.)
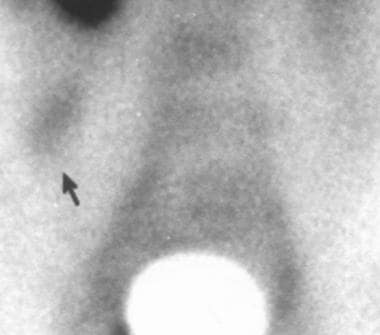
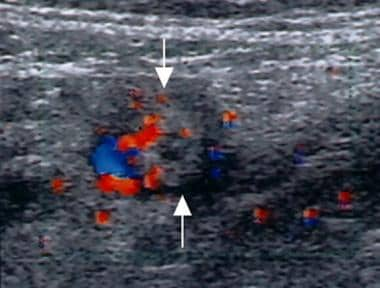 Suppurative appendicitis; transverse view, color Doppler ultrasound image. Circumferential colors are observed in the wall of the inflamed appendix (arrows), a strong indicator of acute appendicitis.
Suppurative appendicitis; transverse view, color Doppler ultrasound image. Circumferential colors are observed in the wall of the inflamed appendix (arrows), a strong indicator of acute appendicitis.
A diagnosis of acute appendicitis is usually made on the basis of a patient's clinical history in conjunction with physical examination and laboratory studies. Because the surgical aim is to operate early—before appendiceal rupture and peritonitis develop—patients who present with typical findings undergo immediate surgery without radiologic evaluation. However, such imaging is advisable in patients with atypical symptoms, which can occur in infants and small children, the elderly, and young women (see the image below).
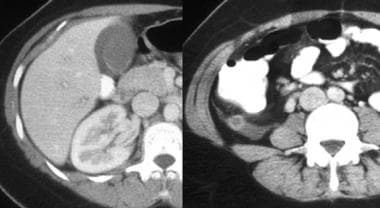 Atypical presentation of appendicitis in a young woman; computed tomography scan. The patient presented with an elevated white blood cell count and right upper quadrant pain. Left, there is pericholecystic fluid and free fluid in the right paracolic gutter, which is caused by retrocecal appendicitis. Right, the appendix, observed in axial section, has an increased diameter and an enhancing thickened wall.
Atypical presentation of appendicitis in a young woman; computed tomography scan. The patient presented with an elevated white blood cell count and right upper quadrant pain. Left, there is pericholecystic fluid and free fluid in the right paracolic gutter, which is caused by retrocecal appendicitis. Right, the appendix, observed in axial section, has an increased diameter and an enhancing thickened wall.
Imaging modalities
Controversy exists as to whether imaging is required in patients with the classic history and physical findings of acute appendicitis. Opinion varies as to whether these modalities should be performed in all patients with suggested appendicitis or if radiology should be reserved for select patients with atypical or confusing clinical presentations.
According to the American College of Radiology (ACR), computed tomography is the most accurate imaging study for evaluating suspected acute appendicitis and alternative etiologies of right lower quadrant pain. In children, ultrasound is the preferred initial examination, because it is nearly as accurate as CT for the diagnosis of acute appendicitis in this population without use of ionizing radiation. In pregnant women, ultrasound is preferred initially, with MRI as a second imaging examination in inconclusive cases. [3] In a retrospective review of MRI in 42 pregnant patients for detection of acute appendicitis, accuracy was 88.1%, sensitivity 60%, specificity 91.9%, positive predictive value 50%, and negative predictive value 94.4%. [4]
The Prospective Observational Study on Acute Appendicitis Worldwide (POSAW) of 4282 patients in 116 worldwide surgical departments from 44 countries reported imaging played a cardinal role in the diagnosis of acute appendicitis. Reliable imaging in patients with clinical suspicion of appendicitis reduced the rate of negative appendectomy by almost 15%. About one third (28.8%) of patients did not undergo any radiologic examination, whereas the majority (43.3%) underwent US and 21.2% had a CT scan. [5]
Multidetector computed tomography scanning and graded-compression Doppler ultrasonography are powerful imaging methods that substantially improve diagnostic accuracy in patients with clinically equivocal appendicitis. [6] Continuous improvements in imaging technology, technique, and interpretation that have been achieved over the past 15 years have substantially increased the accuracy of imaging methods. US and CT scanning have gained acceptance as the primary imaging techniques for acute appendicitis by virtue of their ability to directly image the appendix, adjacent fat, and gut. [7]
Graded-compression US of the right lower quadrant (RLQ) has been shown to be a useful examination because of this technique’s safety and high accuracy (approximately 90%) in the diagnosis of acute appendicitis. Advantages of US include lack of radiation exposure, noninvasiveness, short acquisition time, and the potential for diagnosis of other causes of abdominal pain, particularly in the subset of patients who are women of childbearing age. Several authors suggest that US should be the first imaging method used in pregnant women and pediatric patients because x-ray exposure is especially undesirable in these groups. [4, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17]
Contrast-enhanced, thin-section (0.5 mm) CT scanning has become the preferred imaging technique in the diagnosis of acute appendicitis and its complications, with a high diagnostic accuracy of 95-98%. The literature suggests that limited helical CT scanning with rectal contrast is a highly accurate, time-efficient, cost-effective way to evaluate adult patients with equivocal presentations for appendicitis. CT scanning is particularly preferred in patients in whom appendiceal perforation is suspected, because the diagnostic accuracy remains high and because CT scanning is useful for characterizing periappendiceal inflammatory masses. Ultrasonography has been found to be highly specific but nonsensitive for perforated appendicitis. [8]
Other advanced radiologic examinations, such as magnetic resonance imaging (MRI), scintigraphy, and color Doppler US, have been used in the diagnosis of acute appendicitis, with a diagnostic accuracy of approximately 91-95%. [18, 9, 19, 10]
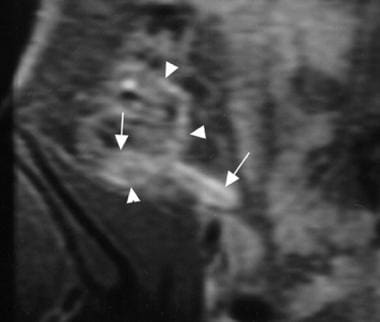 Acute suppurative appendicitis in a 15-year-old boy; contrast-enhanced, fat-suppressed, T1-weighted, spin-echo coronal magnetic resonance image. A markedly enhanced and thickened inflamed appendix (arrows) with pericecal enhancement due to the extent of inflammation is shown.
Acute suppurative appendicitis in a 15-year-old boy; contrast-enhanced, fat-suppressed, T1-weighted, spin-echo coronal magnetic resonance image. A markedly enhanced and thickened inflamed appendix (arrows) with pericecal enhancement due to the extent of inflammation is shown.
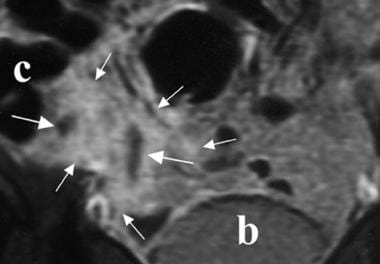 Periappendiceal abscess; contrast-enhanced, fat-suppressed, T1-weighted, spin-echo coronal magnetic resonance image. Fluid collections (long arrows) and a markedly enhanced pericecal area (short arrows) are shown. b = bladder; c = cecum.
Periappendiceal abscess; contrast-enhanced, fat-suppressed, T1-weighted, spin-echo coronal magnetic resonance image. Fluid collections (long arrows) and a markedly enhanced pericecal area (short arrows) are shown. b = bladder; c = cecum.
 Acute suppurative appendicitis in a 27-year-old woman; scintigraphy study. Pathologic accumulation of technetium-99m human immunoglobulin on the right iliac fossa is observed at 4 hours.
Acute suppurative appendicitis in a 27-year-old woman; scintigraphy study. Pathologic accumulation of technetium-99m human immunoglobulin on the right iliac fossa is observed at 4 hours.
Advantages of MRI include better visualization of abnormal appendices and adjacent inflammatory processes, visualization of the appendix in an atypical location, delineation of pathology, operator independence, and ease of examination of patients who are obese. MRI, as with enhanced CT scanning, can demonstrate the extent of inflammatory infiltration. [20, 21, 22, 23, 11, 19, 4, 10]
The decision to obtain US or CT scan studies depends on institutional preference and the available user expertise, although patient age, sex, and body habitus are important influencing factors. US and CT scanning have similar diagnostic value for detecting an alternative diagnosis in a patient in whom acute appendicitis is suspected. [12, 6, 24, 25, 7, 8]
In a meta-analysis of 6 prospective studies, CT demonstrated superior sensitivity (91%) and specificity (90%) over ultrasonography (sensitivity 78%; specificity, 83%). [26]
Delaying surgery to complete a radiologic investigation for appendicitis was found not to increase the rate of perforation or complications but did decrease the rate of negative appendectomies. The rate of negative appendectomy decreased significantly with CT as compared to clinical evaluation only (9.3% vs 5%). Ultrasonography alone, however, did not result in a rate decrease. [27]
In pregnant patients with acute appendicitis, ultrasound is typically performed first, often followed by MRI if there is uncertainty regarding the diagnosis. In a retrospective study by Ahmed et al of 364 pregnant patients with suspicion of acute appendicitis, US was able to visualize the appendix in only 6 (1.65%), 5 of whom had appendicitis. Pathology confirmed acute appendicitis in 19. Of 141 patients who underwent MRI, appendicitis was correctly diagnosed in 9. [20]
Limitations of techniques
Abdominal radiographs are normal in many patients with acute appendicitis and should not be obtained routinely. An appendicolith is the most specific sign on plain radiographic films, but it is observed in only 10% of patients with appendicitis. Disadvantages of barium enema include a high incidence of nondiagnostic examinations, radiation exposure, insufficient sensitivity, and invasiveness.
A significant disadvantage of US is that it is operator dependent. Research has shown diagnostic accuracy can be improved by combining clinical assessment with sonography. [28] Intestinal peristalsis, pulsations of the iliac artery (when it is close to the appendix), deep respiration in noncooperative patients, and difficulty maintaining the probe at the same location for a long time are disadvantages of color Doppler US in detecting increased vascularity of the appendix.
Disadvantages of CT scanning include radiation exposure, the potential for anaphylactoid reaction if intravenous (IV) contrast is used, lengthy preparation time if oral contrast is used, and patient discomfort if rectal contrast is used.
Disadvantages of MRI include high cost, use of IV contrast, the requirement that patients fully cooperate, difficulty with patients who are claustrophobic, the inability to observe an appendicolith in the lumen (an important finding in acute appendicitis), and the inability to differentiate between gas and an appendicolith in the perforation site.
Disadvantages of radionuclide scanning include long acquisition times (approximately 5 h) and the lack of availability of this modality.
European Association of Endoscopic Surgery (EAES) guidelines
The EAES has made the following recommendations [2] :
-
Ultrasound is reliable in increasing the likelihood of acute appendicitis but not reliable in excluding the diagnosis.
-
CT scanning with IV contrast is superior to ultrasound for appendicitis diagnosis.
-
MRI can provide similar diagnostic accuracy to CT.
-
It is recommended that ultrasound be performed as a first-level diagnostic imaging, although it has lower diagnostic value if confirmation is desired.
-
If after ultrasound the diagnosis is not confirmed or ruled out, CT or MRI should be performed.
-
In obese patients, CT or MRI is more accurate than ultrasound and recommended in cases of doubt of diagnosis.
-
In pregnant patients, MRI is recommended if diagnosis is in doubt.
-
In children, MRI is recommended if diagnosis is in doubt.
American College of Radiology guidelines
According to the American College of Radiology (ACR) recommendations include the following [3] :
-
Computed tomography is the most accurate imaging study for evaluating suspected acute appendicitis and alternative etiologies of right lower quadrant pain.
-
In children, ultrasound is the preferred initial examination, because it is nearly as accurate as CT for the diagnosis of acute appendicitis in this population without the use of ionizing radiation.
-
In pregnant women, ultrasound is preferred initially, with MRI as a second imaging examination in inconclusive cases.
-
Suppurative appendicitis; transverse view, color Doppler ultrasound image. Circumferential colors are observed in the wall of the inflamed appendix (arrows), a strong indicator of acute appendicitis.
-
Atypical presentation of appendicitis in a young woman; computed tomography scan. The patient presented with an elevated white blood cell count and right upper quadrant pain. Left, there is pericholecystic fluid and free fluid in the right paracolic gutter, which is caused by retrocecal appendicitis. Right, the appendix, observed in axial section, has an increased diameter and an enhancing thickened wall.
-
Appendicitis in a young physician; computed tomography (CT) study. Intravenous (IV) contrast was administered to the patient, who had gram-negative sepsis but no abdominal pain on examination. Left, an inconclusive CT scan after administration of oral contrast but no IV contrast. Right, a repeat CT scan study following administration of IV contrast demonstrates the thickened, enhanced appendiceal wall and periappendiceal changes. The retrocecal location of the appendix may have attenuated abdominal symptoms.
-
Acute suppurative appendicitis in a 15-year-old boy; contrast-enhanced, fat-suppressed, T1-weighted, spin-echo coronal magnetic resonance image. A markedly enhanced and thickened inflamed appendix (arrows) with pericecal enhancement due to the extent of inflammation is shown.
-
Acute suppurative appendicitis in a 27-year-old woman; scintigraphy study. Pathologic accumulation of technetium-99m human immunoglobulin on the right iliac fossa is observed at 4 hours.
-
Periappendiceal abscess; contrast-enhanced, fat-suppressed, T1-weighted, spin-echo coronal magnetic resonance image. Fluid collections (long arrows) and a markedly enhanced pericecal area (short arrows) are shown. b = bladder; c = cecum.
-
Normal appendix; barium enema radiographic examination. A complete contrast-filled appendix is observed (arrows), which effectively excludes the diagnosis of appendicitis.
-
Normal appendix; computed tomography (CT) scan. A normal appendix, visualized here at the base of the cecum (arrow), is observed in 44-51% of patients. Thin-section CT scans (5-mm collimation or less) are more useful in identifying the appendix. Oral or rectal contrast should be administered. Intravenous contrast is useful in enabling enhancement and edema of the appendiceal wall to be identified.
-
Distal appendicitis; computed tomography scan. The appendiceal lumen may be normal proximally (left, arrow), but distension and inflammatory changes are noted distally (right, open arrow).
-
Retrocecal appendix; computed tomography scan. Left, the appendix occurs in a retrocecal location in 65% of patients. Right, in this young female, the appendix extends cranially as far as the posterior lobe of the liver. Appendicitis in a patient with a retrocecal appendix may present atypically, with less or poorly localized pain, discomfort on coughing or walking, or flank, rather than right lower quadrant, tenderness.
-
Arrowhead sign; computed tomography scan. The presence of this sign indicates contrast outlining the cecum and funneling into the origin of the appendix, with obstruction of the lumen preventing retrograde flow of barium into the distal appendix.
-
Acute gangrenous appendicitis with calcified appendicolith; computed tomography (CT) scan. A calcified appendicolith in the lumen of an enlarged inflamed appendix is shown.
-
Perforated appendicitis with abscess; computed tomography scan. Note the appendicolith (arrow) and air within the abscess. The terminal ileum lies anterior to the appendiceal abscess, and inflammatory change is noted in its wall, which appears thickened (open arrow).
-
Crohn disease in a young woman; computed tomography scan. The patient presented with acute right lower quadrant pain and fever. She had a normal-appearing appendix, but thickening of the wall of the terminal ileum was noted (arrow) in addition to sclerotic changes of both sacroiliac joints, that was consistent with sacroiliitis in association with Crohn disease.
-
Severe acute pancreatitis in a young man; computed tomography scans. The patient presented with peripancreatic effusions that resulted in right lower quadrant pain. Fluid had tracked down the right paracolic gutter (left, arrow, coronal section) in addition to the anterior pararenal space (right, axial view).
-
Acute suppurative appendicitis; contrast-enhanced, fat-suppressed, T1-weighted, spin-echo axial magnetic resonance image. A markedly enhanced and thickened inflamed appendix (arrows) is shown. a = iliac artery; c = cecum; p = psoas muscle; v = iliac vein.
-
Normal appendix; contrast-enhanced, fat-suppressed, T1-weighted, spin-echo coronal magnetic resonance image. Mild enhancement in the unenlarged appendix, ileum (arrowhead), and cecum is shown.
-
Normal appendix; longitudinal ultrasonogram. A compressible tubular appendiceal structure with an outer diameter of less than 6 mm (arrows) is shown. A = iliac artery; V = iliac vein.
-
Suppurative appendicitis in a 15-year-old boy; longitudinal ultrasonogram. An aperistaltic, noncompressible, blind-ended, fluid-filled, tubular appendiceal structure is shown, and distinct wall layers (arrows) arising from the base of the cecum are observed.
-
Phlegmonous appendicitis; oblique-axial ultrasonogram. A pericecal fluid collection, which is walled off by small-bowel loops (arrowheads) is shown, and an appendicolith with an acoustic shadow (arrow) is observed.
-
Suppurative appendicitis in a 15-year-old boy; longitudinal view, pathologic specimen. An inflamed appendix with appendicoliths in the lumen (arrow) is demonstrated.
-
Gangrenous appendicitis; longitudinal ultrasonogram. A markedly distended appendix (arrows), loss of mucosa and submucosal layers, and prominent echogenic pericecal fat are shown.
-
Distended gangrenous appendix; pathologic specimen.
-
Perforated appendix; longitudinal ultrasonogram. A defect on the tip (large arrow, right side) of the enlarged appendix (short arrows, left side) is observed. c = cecum.
-
Periappendiceal abscess formation; oblique-axial ultrasonogram. A thick-walled, complex, hypoechoic mass adjacent to the cecum (arrows) is shown. The inflamed appendix was not visualized.
-
Computed tomography scan reveals an enlarged appendix with thickened walls, which do not fill with colonic contrast agent, lying adjacent to the right psoas muscle.
