Practice Essentials
Pneumothorax, which is the presence of air within the pleural space, is considered to be one of the most common forms of thoracic disease. It is classified as spontaneous (not caused by trauma), traumatic, or iatrogenic (see the images below). [1, 2, 3, 4] Chest radiography is the first investigation performed to assess pneumothorax, because it is simple, inexpensive, rapid, and noninvasive; however, it is much less sensitive than chest computed tomography (CT) scanning in detecting blebs or bullae or a small pneumothorax. [3, 5, 6, 7, 8, 9, 10] High-resolution thin-slice CT has been found to have a greater senstivity for blebs and bullae than routine CT. [11]
Prehospital portable ultrasonography (US) may provide diagnostic and therapeutic benefit when conducted by a proficient examiner who used goal-directed and time-sensitive protocols, as determined in an air rescue setting. US is increasingly used in the acute care setting as a readily available bedside tool, especially in the intensive care unit (ICU) and emergency department (ED) settings. This modality provides a rapid imaging option for diagnosis of pneumothorax, but this evaluation should not delay treatment of a clinically apparent tension pneumothorax. [12]
The use of ultrasound for detection of pneumothorax has been studied for both adults and children and has been shown to be particularly sensitive in newborns. [13, 14, 15]
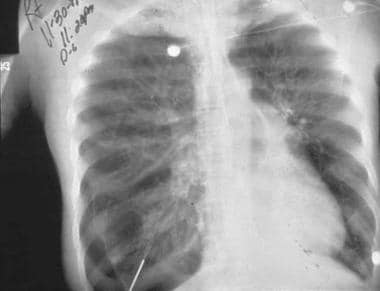
 A large, right-sided pneumothorax has occurred from a rupture of a subpleural bleb.
A large, right-sided pneumothorax has occurred from a rupture of a subpleural bleb.
 A true pneumothorax line. Note that the visceral pleural line is observed clearly, with the absence of vascular marking beyond the pleural line.
A true pneumothorax line. Note that the visceral pleural line is observed clearly, with the absence of vascular marking beyond the pleural line.
Spontaneous pneumothorax may be either primary (occurring in persons without clinically or radiologically apparent lung disease) or secondary (in which lung disease is present and apparent). Most individuals with primary spontaneous pneumothorax (PSP) have unrecognized lung disease; many observations suggest that spontaneous pneumothorax often results from rupture of a subpleural bleb. [1, 2, 3, 16, 17] In a study of spontaneous pneumothorax in 55 children, 9 had visible bullae on initial radiograph, and apical emphysematous-like changes (ELC) were identified in 37 children by CT. The most successful surgical approach was thoracoscopic staple bullectomy and pleurectomy. [3]
Spontaneous pneumothorax in nonventilated patients with COVID-19 has been reported. [18, 19, 20]
In neonates with pneumothorax, [13, 14, 15] ultrasound has been found in some studies to be comparable to chest radiography. A study by Cattarossi et al found that ultrasound was able to detect pneumothorax in all 23 affected patients. [13] Another study, by Raimondi et al, found that in 26 critically ill newborns, sensitivity, specificity, positive predictive value, and negative predictive value were all 100%. [14]
Traumatic pneumothorax is caused by penetrating or blunt trauma to the chest, with air entering the pleural space directly through the chest wall, through visceral pleural penetration, or through alveolar rupture resulting from sudden compression of the chest.
Iatrogenic pneumothorax is a pneumothorax that has developed as a complication of an invasive procedure, such as a pulmonary needle biopsy, placement of a central venous line, or positive pressure ventilation. [21] With the increasing use of invasive diagnostic procedures, iatrogenic pneumothorax likely will become more common, although most cases are of little clinical significance.
Persistent pneumothorax is defined as a continued air leak from an in situ chest drain for more than 48 hours after insertion. This may result from a kink in, or malposition of, the tube; lung parenchymal disease; bronchopleural fistula; or esophageal-pleural fistula. [4]
Complications of pneumothorax
In most reported series, the rate of recurrence of spontaneous pneumothorax on the same side is as much as 30%; on the contralateral side, the rate of recurrence is approximately 10%.
Other complications include the following:
-
Reexpansion pulmonary edema
-
Bronchopleural fistula, which occurs in 3-5% of patients
-
Pneumomediastinum and pneumopericardium
Tension pneumothorax may occur after spontaneous pneumothorax, although it is more common after traumatic pneumothorax or with mechanical ventilation.
Radiography
The diagnosis of pneumothorax is established by demonstrating the outer margin of the visceral pleura (and lung), known as the pleural line, separated from the parietal pleura (and chest wall) by a lucent gas space devoid of pulmonary vessels. (The pleural line appears in the image below.)
A true pneumothorax line. Note that the visceral pleural line is observed clearly, with the absence of vascular marking beyond the pleural line.
The pleural line may be difficult to detect with a small pneumothorax unless high-quality posteroanterior and lateral chest films are obtained and viewed under a bright light. A skin fold may mimic the pleural line; usually, the patient is asymptomatic (see the image below).
 Note that although a skin fold can mimic a subtle pneumothorax, lung markings are visible beyond the skin fold.
Note that although a skin fold can mimic a subtle pneumothorax, lung markings are visible beyond the skin fold.
In erect patients, pleural gas collects over the apex, and the space between the lung and the chest wall is most notable at that point (see the image below).
A large, right-sided pneumothorax has occurred from a rupture of a subpleural bleb.
In the supine position, the juxtacardiac area, the lateral chest wall, and the subpulmonic region are the best areas to search for evidence of pneumothorax (see the image below). The presence of a deep costophrenic angle on a supine film may be the only sign of pneumothorax; this has been termed the deep sulcus sign. The supine radiograph is of particular importance in trauma or critically ill patients. [22]
 Deep sulcus sign in a supine patient in the ICU. The pneumothorax is subpulmonic.
Deep sulcus sign in a supine patient in the ICU. The pneumothorax is subpulmonic.
When a suggested pneumothorax is not definitively observed on an inspiratory film, an expiratory film may be helpful. At end expiration, the constant volume of the pneumothorax gas is accentuated by the reduction of the hemithorax, and the pneumothorax is recognized more easily. Similar accentuation may be obtained with lateral decubitus studies of the appropriate side (for a possible left pneumothorax, a right lateral decubitus film of the chest should be obtained, with the beam centered over the left lung).
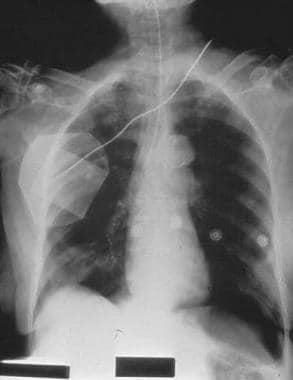
The most common radiographic manifestations of tension pneumothorax are mediastinal shift, diaphragmatic depression, and rib cage expansion (see the image below).
 An older man admitted to ICU postoperatively. Note the right-sided pneumothorax induced by the incorrectly positioned small-bowel feeding tube in the right-sided bronchial tree. Marked depression of the right hemidiaphragm is noted, and mediastinal shift is to the left side, suggestive of tension pneumothorax. The endotracheal tube is in a good position.
An older man admitted to ICU postoperatively. Note the right-sided pneumothorax induced by the incorrectly positioned small-bowel feeding tube in the right-sided bronchial tree. Marked depression of the right hemidiaphragm is noted, and mediastinal shift is to the left side, suggestive of tension pneumothorax. The endotracheal tube is in a good position.
Any significant degree of displacement of the mediastinum from the midline position on maximum inspiration, as well as any depression of the diaphragm, should be taken as evidence of tension (see the image below), although a definite diagnosis of tension pneumothorax is difficult to make on the basis of radiographic findings. The degree of lung collapse is an unreliable sign of tension, since underlying lung disease may prevent collapse even in the presence of tension.
 Right main stem intubation resulting in left-sided tension pneumothorax, right mediastinal shift, deep sulcus sign, and subpulmonic pneumothorax
Right main stem intubation resulting in left-sided tension pneumothorax, right mediastinal shift, deep sulcus sign, and subpulmonic pneumothorax
Pleural effusions occur coincident with pneumothorax in 20-25% of patients, but they usually are quite small. Hemopneumothorax occurs in 2-3% of patients with spontaneous pneumothorax. Bleeding is believed to represent rupture or tearing of vascular adhesions between the visceral and parietal pleura as the lung collapses.
False positives/negatives
Differentiating the pleural line of a pneumothorax from that of a skin fold, clothing, tubing, or chest wall artifact is important. Careful inspection of the film may reveal that the artifact extends beyond the thorax or that lung markings are visible beyond the apparent pleural line. In the absence of underlying lung disease, the pleural line of a pneumothorax usually parallels the shape of the chest wall (see the images below).
A true pneumothorax line. Note that the visceral pleural line is observed clearly, with the absence of vascular marking beyond the pleural line.
Note that although a skin fold can mimic a subtle pneumothorax, lung markings are visible beyond the skin fold.
Artifactual densities usually do not parallel the course of the chest wall over their entire length. Avascular bullae or thin-walled cysts may be mistaken for a pneumothorax. The pleural line caused by a pneumothorax usually is bowed at the center toward the lateral chest wall. Unlike in pneumothorax, the inner margins of bullae or cysts usually are concave rather than convex and do not conform exactly to the contours of the costophrenic sulcus. A pneumothorax with a pleural adhesion also may simulate bullae or lung cysts.
Computed Tomography
CT scanning of the chest is being used with increasing frequency in patients with pneumothorax. CT may be necessary to diagnose pneumothorax in critically ill patients in whom upright or decubitus films are not possible.
As indicated in a study by Warner et al, CT scanning may prove helpful in predicting the rate of recurrence in patients with spontaneous pneumothorax. The authors found that patients with larger or more numerous blebs, as demonstrated on thoracic CT, are more likely to experience recurrences. [23]
CT demonstrates focal areas of emphysema in more than 80% of patients with spontaneous pneumothorax, even in lifelong nonsmokers. These areas are situated predominantly in the peripheral regions of the apex of the upper lobes. (In patients in whom emphysema is not apparent on CT, it often is evident at surgery or on pathologic examination.)
Multidetector CT (MDCT) has been found to be highly effective in measuring the volume of pneumothoraces. [24, 25, 26]
Degree of confidence
Rahal et al performed a study of the value of CT in pediatric primary spontaneous pneumothorax by evaluating preoperative CT scans for the diagnostic accuracy of bleb disease. All patients underwent video-assisted thoracoscopic surgery (VATS), and 34 of 39 patients were found to have blebs. Of the 39 patients, 28 underwent preoperative CT scans, and 17 of the 28 were diagnosed with blebs, which were confirmed on VATS. However, of the 11 patients in whom blebs were not identified on CT, 7 were found to have blebs on VATS. The positive and negative predictive values of preoperative CT for detecting ipsilateral bleb disease were 100% and 36%, respectively, with a sensitivity of 71%. [27]
In a study by Mitlehner et al of 35 patients with primary spontaneous pneumothorax, localized emphysema with or without bulla formation was identified on CT in 31 patients (89%) and on radiographs in 15 patients (43%). [16] Abnormal findings were observed in the lung ipsilateral to the pneumothorax on 28 CT scans (80%) and on 11 chest radiographs (31%); abnormal findings were observed in the contralateral lung on 23 CT scans (66%) and on 4 chest radiographs (11%). In most patients, the abnormal findings consisted of a few localized areas of emphysema (n < 5) measuring less than 2 cm in diameter.
Ultrasonography
The use of ultrasound for detection of pneumothorax has been studied for both adults and children. [3, 9, 10, 13, 14, 15] On ultrasonography, the sliding movement or lung pulse at the pleural interface indicates the absence of a pneumothorax. [10]
In a meta-analysis by Chan et al of the diagnostic accuracy of chest ultrasonography versus supine chest radiography for the diagnosis of pneumothorax in trauma patients in the ED, the diagnostic accuracy of ultrasonography was found to be superior to that of supine chest radiography. According to the researchers, if 30 of 100 patients had traumatic pneumothorax, ultrasonography would miss 3 cases and overdiagnose 1 (false positive), whereas radiography would miss 16 cases and overdiagnose none. [28]
A study by Kumar et al found that in 8 patients who developed pneumothorax after flexible bronchoscopy and transbronchial lung biopsy, ultrasonography was able to detect pneumothorax in all the cases. [10]
In a study of spontaneous pneumothorax in 55 children, 9 had visible bullae on initial radiograph, and apical emphysematous-like changes (ELC) were identified in 37 children by CT. The most successful surgical approach was thoracoscopic staple bullectomy and pleurectomy. [3] In neonates with pneumothorax, [13, 14, 15] ultrasound has been found in some studies to be comparable to chest radiography. A study by Cattarossi et al found that ultrasound was able to detect pneumothorax in all 23 affected newborns. [13] Another study, by Raimondi et al, found that in 26 critically ill newborns, sensitivity, specificity, positive predictive value, and negative predictive value were all 100%. [14]
-
A large, right-sided pneumothorax has occurred from a rupture of a subpleural bleb.
-
A true pneumothorax line. Note that the visceral pleural line is observed clearly, with the absence of vascular marking beyond the pleural line.
-
Note that although a skin fold can mimic a subtle pneumothorax, lung markings are visible beyond the skin fold.
-
Deep sulcus sign in a supine patient in the ICU. The pneumothorax is subpulmonic.
-
An older man admitted to ICU postoperatively. Note the right-sided pneumothorax induced by the incorrectly positioned small-bowel feeding tube in the right-sided bronchial tree. Marked depression of the right hemidiaphragm is noted, and mediastinal shift is to the left side, suggestive of tension pneumothorax. The endotracheal tube is in a good position.
-
Right main stem intubation resulting in left-sided tension pneumothorax, right mediastinal shift, deep sulcus sign, and subpulmonic pneumothorax
-
Pneumomediastinum from barotrauma may result in tension pneumothorax and obstructive shock.
-
A patient in ICU developed pneumopericardium as a manifestation of barotrauma.
