Practice Essentials
Pulmonary edema is differentiated into 2 categories: cardiogenic and noncardiogenic. The latter, noncardiogenic pulmonary edema (NPE), is caused by changes in permeability of the pulmonary capillary membrane as a result of either a direct or an indirect pathologic insult (see the images below). NPE results in acute hypoxia secondary to a rapid deterioration in respiratory status. Many causes of NPE exist, including drowning, acute glomerulonephritis, fluid overload, aspiration, inhalation injury, brain trauma, allergic reaction, and inflammatory processes. The correct diagnosis relies on clinical and radiologic findings, despite some overlap in the clinical and imaging findings between the different causes. To differentiate cardiogenic from noncardiogenic pulmonary edema, in NPE, pulmonary capillary wedge pressure is not elevated and remains less than 18 mmHg. [1, 2, 3, 4]
Less common than other forms of NPE seen in emergency departments, neurology units, or intensive care units (ICUs), neurogenic pulmonary edema usually arises quickly subsequent to significant neurologic insult, being found in patients with intracranial hemorrhage, traumatic brain injuries, and epileptic seizures. [5, 6]
Chest radiography is the examination of choice in NPE. Most patients with NPE are seriously ill and immobile, and there may be transportation problems regarding computed tomography (CT) scanning and magnetic resonance imaging (MRI) units. Conventional chest radiography is readily and universally available, and it has the added advantage of portability. In conjunction with the clinical presentation, radiographic findings are generally sufficient to arrive at a diagnosis of NPE. However, the specificity of chest radiographs, particularly portable, anteroposterior (AP) images, is low, and it may not be possible to differentiate the various causes of lung parenchymal shadowing on radiographs alone. Ssedation may be required to obtain images that are not degraded by motion artifacts. [7]
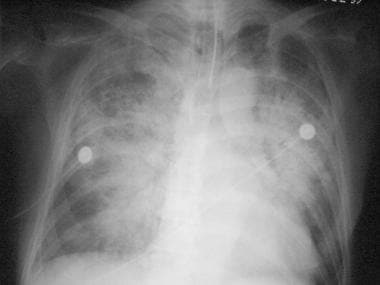 Anteroposterior chest radiograph shows interstitial and alveolar pulmonary edema.
Anteroposterior chest radiograph shows interstitial and alveolar pulmonary edema.
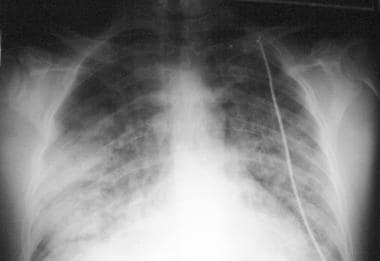 Anteroposterior chest radiograph shows bilateral alveolar opacities in a patient with subarachnoid hemorrhage who developed neurogenic pulmonary edema.
Anteroposterior chest radiograph shows bilateral alveolar opacities in a patient with subarachnoid hemorrhage who developed neurogenic pulmonary edema.
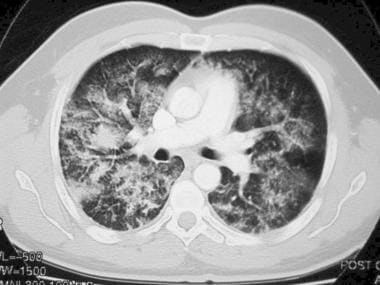 Axial, contrast-enhanced computed tomography (CT) scan shows alveolar and interstitial pulmonary edema.
Axial, contrast-enhanced computed tomography (CT) scan shows alveolar and interstitial pulmonary edema.
An initial and rapid increase in pulmonary vascular pressure due to pulmonary vasoconstriction or pulmonary blood flow can lead to pulmonary microvascular injury. An increase in vascular permeability consequently results in edema formation, as suggested by the frequent observation of pulmonary hemorrhage in NPE (ie, the blast theory).
Two major components contribute to the pathogenesis of NPE: elevated intravascular pressure and pulmonary capillary leak. Therefore, hemodynamic cardiogenic and noncardiogenic components exist. These components often work in concert, as in pulmonary edema after epileptic convulsions or intracranial pressure elevation. The hemodynamic component is relatively brief and may unmask pure NPE, such as that seen in experimental seizures.
Whether the hemodynamic changes produce a pulmonary capillary leak through pressure-induced mechanical injury to the pulmonary capillaries or whether some direct nervous system control over pulmonary capillary permeability exists remains uncertain. The neuro-effector site for nervous system–induced pulmonary edema appears to be relatively well established in regions about the caudal medulla, where nuclei regulating systemic arterial pressure, as well as afferent and efferent pathways to and from the lungs, are located.
NPE is a rare but severe adverse effect of acetazolamide and should be considered when acetazolamide is prescribed after routine cataract surgery. [8] NPE has also been reported after naloxone administration and after termination of cardiopulmonary bypass support during cardiac surgery. [9, 10]
NPE has also been tied to calcium-channel blocker overdose, with a case study reporting the development of refractory NPE in a female aged 27 years who ingested 18,000 mg of verapamil. Although her condition worsened to severe hypoxic respiratory failure, she subsequently achieved full recovery following venovenous extracorporeal membrane oxygenation (VV-ECMO). [11]
Fluid retention and NPE are known to develop during stem cell mobilization in the treatment of patients with systemic immunoglobulin light chain (AL) amyloidosis. A case report by Oka and Ono found that using cell‐free and concentrated ascites reinfusion therapy (CART) controlled fluid retention in the study patient, a male aged 63 years with systemic AL amyloidosis. [12]
A case report from Yi and Li discussed a male aged 55 years with esophageal cancer whose death from NPE was associated with the intravenous administration of 100 mL of nonionic, iso-osmolar iodine contrast medium (iodixanol). Digestive tract symptoms in the patient were followed by shock and respiratory and circulatory failure. The investigators concluded that in patients who receive iso-osmolar contrast medium, gastrointestinal events “may be the prodromal symptoms of [NPE].” [13]
High-altitude pulmonary edema (HAPE) is a fatal form of severe high-altitude illness. This form of NPE occurs secondary to hypoxia. Clinical diagnosis is characterized by fatigue, dyspnea, and dry cough with exertion. If left untreated, HAPE can progress to dyspnea at rest, rales, and cyanosis; it has a mortality rate of up to 50%. Clinical diagnosis would include at least 2 of the following symptoms or complaints: chest tightness or pain, cough, dyspnea at rest, and decreased exercise tolerance. Two of the following exam findings would be noted: central cyanosis, rales/wheezes, tachycardia, and tachypnea. Chest x-ray may show patchy alveolar infiltrates with normal-sized mediastinum/heart. Ultrasound may show B-lines consistent with pulmonary edema, and ECG may show signs of right-axis deviation and/or ischemia. In a patient with infiltrates on chest x-ray, rapid correction of clinical status and SpO2 (percentage of oxygen saturation) with supplemental oxygen is pathognomonic of HAPE. [14]
Transfusion reactions are adverse events that occur after transfusion of blood products such as whole blood, fresh frozen plasma, platelets, cryoprecipitate, granulocytes, intravenous immune globulin, allogenic and autologous stem cells, and packed red blood cells. Transfusion-related acute lung injury (TRALI) is a clinical syndrome in which acute NPE is associated with hypoxia that occurs during or after a transfusion. It is the leading cause of death from transfusion. Chest radiography shows bilateral pulmonary infiltrates. Clinical characteristics of TRALI include acute dyspnea, hypoxemia, fever, hypotension, tachycardia, leukopenia, thrombocytopenia, and normal pulmonary artery occlusion pressure due to NPE. Once the transfusion has stopped, gradual recovery may take 2 to 4 days. Chest x-ray shows improvement within 2 to 5 days. [15]
Rare reports have emerged of NPE resulting from gadolinium-based contrast administration for MRI. In one such case, reported by Nguyen and Pham, a generally healthy woman aged 23 years developed, after receiving gadolinium-based contrast, NPE “with a moderate oxygenation impairment and no mucosal or cutaneous features of anaphylaxis.” The patient quickly recovered after positive-pressure ventilation was initiated. [16]
On initial evaluation, a patient with NPE may be found to lack acute cardiac disease or inappropriate fluid balance, to have no peripheral edema, and to possess flat neck veins. A peripheral distribution of bilateral infiltrates may be demonstrated on chest imaging, with evidence of excessive pulmonary vasculature congestion or cardiomegaly being absent. A lack of acute systolic or diastolic dysfunction may be confirmed via echocardiogram. Such findings suggest that the source of the pulmonary edema is noncardiogenic. [1]
A study by Karaman and Ozkaya looked at the differential diagnosis of negative pressure pulmonary edema (NPPE), a form of NPE “that results from the generation of high negative intrathoracic pressure following forced spontaneous breathing against upper airway obstruction after nasal or upper airway surgery.” The investigators stated that NPPE can, postoperatively, be mistaken for coronavirus disease 2019 (COVID-19). They pointed out, however, that although hypoxemia, respiratory distress, and, on chest CT scan, ground-glass opacities occur with both NPPE and COVID-19, patients with NPPE display the opacities primarily in central areas, as opposed to peripheral areas, as seen in COVID-19. Moreover, vascular clarity is decreased in NPPE, while in COVID-19, the areas of opacity demonstrate vascular dilatation. [17]
Acute respiratory distress syndrome (ARDS) may be the most recognized type of NPE. Its acute onset is “secondary to an underlying inflammatory process such as sepsis, pneumonia, gastric aspiration, blood transfusion, pancreatitis, multisystem trauma or trauma to the chest wall, or drug overdose.” [1]
Findings necessary for a diagnosis of ARDS include bilateral infiltrates on chest radiography, a ratio of partial pressure of oxygen (PaO2) to fraction of inspired oxygen (FiO2) of under 300 mmHg, and a positive end-expiratory pressure (PEEP) of 5 cmH2O. [1]
ARDS develops in almost 5% of patients in whom COVID-19 has been diagnosed. A correspondence exists between the extravascular lung water index (EVLWI), which is a marker of pulmonary edema, and ARDS-related mortality. A 2021 observational study reported that EVLWI is markedly elevated in COVID-19 patients with ARDS in comparison with COVID-19–free individuals with ARDS. The investigators proposed that EVLWI could be used to monitor the progression of COVID-19–related ARDS in the ICU. [18]
A retrospective study by Bregel et al indicated that NPE is one of the main risk factors (along with increased D-dimer levels, thrombocytopenia, and ICU hospitalization) for thrombosis in multisystem inflammatory syndrome in children (MIS-C). MIS-C is associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes COVID-19. [19]
Radiography
The heart is usually enlarged in cardiogenic pulmonary edema, but it may be normal in lung injury and NPE. However, the heart may also be of normal size in cardiogenic edema after acute myocardial infarction. Pulmonary vascular plethora often occurs with upper lobe blood diversion in cardiogenic cases; vessels of the upper lobe are balanced to cephalic in fluid overload but are normal in lung injury. Pleural effusion may be seen in all 3 causes. Septal lines indicative of interstitial edema are more frequent with cardiogenic causes than with others.
(Radiographs of pulmonary edema are shown below.)
Anteroposterior chest radiograph shows interstitial and alveolar pulmonary edema.
Anteroposterior chest radiograph shows bilateral alveolar opacities in a patient with subarachnoid hemorrhage who developed neurogenic pulmonary edema.
The infiltrates of cardiogenic pulmonary edema are usually diffuse, and air bronchograms are rare. Infiltrates in nephrogenic pulmonary edema are classically described as having a bat-wing distribution, whereas those in lung injury tend to be more peripheral. Although the peripheral infiltrate is fairly specific for lung injury, the diffuse variety is seen with equal frequency in lung injury. The presence of air bronchograms is also fairly specific for lung injury.
One of 3 patterns is seen: a normal chest, bilateral perihilar pulmonary edema, or generalized pulmonary edema. The early signs of pulmonary edema (interstitial edema) are the septal lines (Kerley B lines), which are horizontal lines seen laterally in the lower zones. The septal lines arise from the pleural surface and are typically 1 mm thick and 10 mm long; unlike blood vessels, these reach the edge of the lung. As the edema progresses, alveolar edema is observed in a butterfly pattern characterized by the central predominance of shadows, with a clear zone at periphery lobes.
Another feature that may be seen is cardiac enlargement, in cases of previous cardiac failure. In its initial stages, ARDS may resemble cardiac pulmonary edema. However, over the course of 24-48 hours following the onset of tachypnea, dyspnea, and hypoxia, ARDS becomes more widespread and uniform. A useful characteristic for differentiating cardiac pulmonary edema from NPE, as well as from pneumonia and other widespread exudates, is the amount of time it takes for the edema to develop and to vanish. If substantial improvement occurs within 24 hours, this is virtually diagnostic of cardiac pulmonary edema.
NPE is a known complication of lung transplantation. [20, 21] Herman and colleagues, however, found chest radiography to be helpful, but not definitive, in distinguishing problems after bilateral lung transplantation and found CT scanning to be excellent for the demonstration of airway problems. In their study, the authors reviewed the postoperative chest radiographic and CT scan findings in 13 patients who underwent bilateral lung transplantation. [22] Portable chest radiography was performed daily for about 10 days, after which upright posteroanterior studies were performed daily for about 10 days and then as clinically required. CT scanning was performed when a complication was suspected.
The reimplantation response (NPE due to ischemia, trauma, denervation, and lymphatic interruption) occurred in 12 patients and usually consisted of bilateral perihilar and basal consolidation. Twelve episodes of acute rejection, an imprecise clinical diagnosis, occurred in 10 patients. Radiographic changes consisted of bibasal (N=2) and right middle and lower (N=2) or left basal consolidation (N=1); no changes were observed in 7 episodes. Following the intravenous administration of steroids, radiographic resolution occurred in 4 cases. [22]
Radiographic findings associated with the reimplantation response and rejection were nonspecific and were mimicked by fluid overload and infection. Bronchial dehiscence and/or stricture formation occurred in 7 patients. In general, chest radiography was inaccurate in the assessment of these complications, and CT scanning was accurate in such assessments. [22]
Degree of confidence
Conventional chest radiographs are universally available. The cause of the pulmonary edema can be determined with a high degree of accuracy by paying careful attention to certain radiographic features.
Milne and colleagues conducted a study of 216 chest radiographs in 61 patients with cardiac disease, 30 with renal failure or overhydration, and 28 with capillary permeability edema. [23] They identified 3 principal and 7 ancillary features; all of these were statistically significant and, in a large percentage of cases, allowed accurate determination of the cause of edema. The 3 principal features found were the distribution of pulmonary flow, the distribution of pulmonary edema, and the width of the vascular pedicle. The ancillary features were pulmonary blood volume, peribronchial cuffing, septal lines, pleural effusions, air bronchograms, lung volume, and cardiac size. Differing constellations of these features, each characteristic of a specific type of edema, were found. Overall accuracy of diagnosis in the Milne study was in the range of 86-89%. The highest accuracy was obtained in distinguishing capillary permeability edema from all other varieties (91%). The lowest accuracy (81%) was obtained in distinguishing chronic cardiac failure from renal failure.
A study by Liebman et al indicated that it is hazardous to accept a portable radiographic diagnosis of congestive heart failure as a cause of pulmonary edema. In their report, the authors assessed the usefulness of portable chest radiographs in defining the amount of physiologic shunting and the severity of NPE. [24, 25] Of the 11 patients, 10 had acute respiratory failure. Radiographic assessment of the amount of pulmonary edema and the severity of left ventricular failure was compared with the physiologic shunt fraction, tracer-measured lung water, and pulmonary arterial wedge pressure. The radiographic scores for edema were not predictive for the shunt fraction or for the tracer-measured lung water. The radiographic score for congestive heart failure was correlated with the wedge pressure but not well enough to be clinically useful.
About 5% of the radiographs were false positive, and 11% were false negative. Radiographic findings lagged behind physiologic derangements. Therefore, the radiographic findings were predictive for the shunt value of the preceding day.
Computed Tomography
CT scanning is seldom used in assessing patients with NPE and ARDS, mostly because of problems in transporting and monitoring these severely ill individuals. In addition, cardiogenic edema can give rise to an appearance similar to NPE on CT scans. (A CT scan of NPE is shown in the image below.)
Axial, contrast-enhanced computed tomography (CT) scan shows alveolar and interstitial pulmonary edema.
Acute respiratory distress syndrome
CT scan findings in NPE are similar to those of ARDS. High-resolution CT (HRCT) scanning demonstrates widespread airspace consolidation, which may have predominant distribution in the dependent lung regions. A reticular pattern with a striking anterior distribution is a frequent finding of follow-up CT scanning in ARDS survivors and is most strongly related to the duration of pressure-controlled, inverse-ratio ventilation. [26]
Tagliabue and colleagues reviewed the findings of 74 patients with ARDS who underwent chest CT scanning. [27] Lung opacities were bilateral in almost all patients and in most cases (86%) were dependent. The opacities were patchy (42%), homogeneous (23%), ground glass (8%), or mixed (27%). Opacities prevailed in basal regions (68%), in comparison to hilar and apical ones. Air bronchograms were frequently seen in areas of consolidation (89%). In contrast to previous reports, pleural effusion was a frequent finding (50%) that did not worsen the patients' prognoses. Often, loculated pneumothorax (32%) was mostly anteromedial. Ineffective position of thoracostomy tubes was detected on CT scans in 13 of 20 patients. Pulmonary air cysts (30%), always multiple and mostly bilateral, were associated with a mortality rate (55%) higher than that of the whole study group (35%). Compared with chest radiography, CT scanning often yielded additional information (66%), with direct influence on patient treatment in 22% of cases.
Gattinoni and coauthors examined 10 patients with full-blown ARDS who were receiving mechanical ventilation with positive end-expiratory pressure (PEEP) and who underwent lung CT scanning. [28] Seven healthy subjects also were included in the study. Three tomographic levels were selected: apex, hilum, and base. The most consistent morphologic finding in ARDS was attenuating in the dependent regions of the lung. Assuming that the 3 levels were a representative sample of the whole lung, the authors computed lung weight from the mean CT scan number and lung gas volume. Through analysis of the CT scan number frequency distribution, the authors found the following definite patterns of distribution:
-
Type 1 - Bimodal, with 1 mode in the normal CT scan number range
-
Type 2 - Unimodal, narrow distribution, with the mode in the CT scan range of water
-
Type 3 - Unimodal, broad distribution in the abnormal CT scan number range
Stark and colleagues described the CT scan features of 28 patients with ARDS. [29] Diffuse lung consolidation, lobar or segmental disease, and multifocal, patchy involvement were observed. Large lung cysts and small cysts producing a Swiss-cheese appearance of the parenchyma were detected. These findings were not regularly appreciated on chest radiographs. The overall mortality was 72.7%. Patients with lung cysts had a trend toward higher mortality (87.5%). Other unexpected findings were basilar lung abscesses and empyema. In 15 patients, CT scans provided additional information that was not obvious on bedside chest radiographs and led to a change in care for 5 patients.
Ultrasonography
Lung ultrasound can provide useful information on ARDS diagnosis when radiography or CT is not available. [7] In addition, it has been used in prehospital assessment in extreme settings (eg, war zones, natural disasters, and extreme-sports settings). For example, ultrasonograhy has been used in the assessment of pulmonary edema in high-altitude missions and after apnea diving. [30]
The bedside lung ultrasound in emergency (BLUE) protocol has been developed for the immediate diagnosis of acute respiratory failure. This protocol requires the mastery of 10 signs indicating normal lung surface (bat sign, lung sliding, A-lines), pleural effusions (quad and sinusoid sign), lung consolidations (fractal and tissue-like sign), interstitial syndrome (lung rockets), and pneumothorax (stratosphere sign and the lung point). These signs have been assessed in adults, with diagnostic accuracies ranging from 90 to 100%, allowing consideration of ultrasound as a reasonable bedside gold standard. [31]
The BLUE protocol has been reported as having a sensitivity of 97%, a specificity of 95%, a positive predictive value of 87%, and a negative predictive value of 99% for diagnosis of acute hemodynamic pulmonary edema. [31]
In the BLUE protocol, profiles have been designed for the diagnosis of pulmonary edema, pneumonia, congestive heart failure, COPD, asthma, pulmonary embolism, and pneumothorax. The B-line is defined using 7 criteria, 3 of which are always present: a comet-tail artifact; arising from the pleural line; and moving in concert with lung sliding (when lung sliding is present). The other 4 criteria are almost always present: long; well-defined; erasing A-lines; and hyperechoic. The resulting sign, lung rockets, indicates that more than 2 B-lines are visible between 2 ribs. Three or four B-lines create the pattern called septal rockets, which correlate with Kerley’s lines (subpleural interlobular septa). Five or more B-lines create a pattern called ground-glass rockets, as they correlate with ground-glass lesions. Lung rockets indicate interstitial syndrome. The B profile associated with hemodynamic pulmonary edema,combines lung sliding with lung rockets at the 4 anterior points. [31]
Echocardiography may also play a role in the differentiation of cardiogenic pulmonary edema from NPE. [32]
Nuclear Imaging
Gallium-67
Raijmakers and co-investigators concluded that a 67Ga pulmonary leak index can be used in distinguishing ARDS from hydrostatic pulmonary edema. In their study, the investigators examined the effectiveness of a noninvasive, bedside, dual-radionuclide method (67Ga circulating transferrin and technetium-99m [99mTc]–labeled RBCs) of measuring pulmonary microvascular permeability to differentiate between hydrostatic pulmonary edema and pulmonary edema due to ARDS. [33] Patients in the study suffered from respiratory insufficiency and bilateral, alveolar pulmonary edema, as demonstrated on chest radiographs. All but one of the patients were mechanically ventilated.
In the Raijmakers et al study, the 2 radionuclides were used to calculate the pulmonary leak index. With various definitions, a supranormal pulmonary leak index for ARDS had a sensitivity of 100%, while its specificity ranged from 46 to 75%. On receiver operating characteristic curves, the pulmonary leak index performed best when ARDS and hydrostatic pulmonary edema were defined only on the basis of risk factors. The index was better than hemodynamic measures, and its performance equaled that of ventilatory variables in discriminating between edema types (if definitions were based primarily on hemodynamic and ventilatory variables, respectively). [33]
FDG–positron emission tomography
According to a study by Chen and Schuster, fluorodeoxyglucose–positron emission tomography (FDG-PET) scanning may be useful for studying neutrophil kinetics during oleic acid–induced lung injury. The investigators measured neutrophil glucose uptake with FDG-PET scanning in anesthetized dogs after intravenous, oleic acid–induced, acute lung injury (N=6) or after low-dose, intravenous endotoxin (which is known to activate neutrophils without causing lung injury) followed by oleic acid (N=7). The authors concluded that the rate of FDG uptake in the lungs during lung injury reflects the state of neutrophil activation. FDG-PET scanning can depict pulmonary sequestration of activated neutrophils, even when alveolar neutrophilia are absent. [34]
Iodine-123
Iodine-123 meta-iodobenzylguanidine (MIBG) results can be considered indicators of pulmonary endothelial cell function.
Koizumi and colleagues studied serial scintigraphic assessment of 123I MIBG lung uptake in a patient with high-altitude pulmonary edema. [35] The initial evaluation was performed 7 days after the patient's admission. The lung-to–upper mediastinum ratios of 123I MIBG uptake were 1.33 for the right lung and 1.12 for the left lung. The second examination, performed 2 months later, showed ratios of 1.39 for the right lung and 1.33 for the left lung. The investigators speculated that the reduction of lung uptake observed in the early recovery stage might be associated with impairment in pulmonary endothelial cell metabolic function in the development of high-altitude pulmonary edema. [35, 36]
-
Anteroposterior chest radiograph shows interstitial and alveolar pulmonary edema.
-
Anteroposterior chest radiograph shows bilateral alveolar opacities in a patient with subarachnoid hemorrhage who developed neurogenic pulmonary edema.
-
Axial, contrast-enhanced computed tomography (CT) scan shows alveolar and interstitial pulmonary edema.
